
Abstract
BACKGROUND:
Vibration exercise has been investigated to enhance muscle activation, however, the effect of different amplitude vibratory exercises on cardiovascular stress is less understood.
OBJECTIVE:
Our study aims to explore the acute effect of shoulder vibratory exercises with different postures and amplitudes on the cardiovascular response in healthy adults.
METHODS:
Using a repeated measures randomized design, 36 subjects performed three different sessions with FLEXI-BAR exercise (FBE): (1) zero-amplitude, (2) small-amplitude, (3) large-amplitude. Each session included three different shoulder positions: 45-, 90- and 180-degree flexion. Heart rate variability (HRV), heart rate (HR) and rating of perceived exertion (RPE) were monitored continuously, while systolic blood pressure (SBP), diastolic blood pressure (DBP) and rate-pressure product (RPP) were measured before and after each exercise session.
RESULTS:
Compared with zero-amplitude, both small- and large-amplitude FBE protocols induced higher SBP. By contrast, DBP decreased with small- and large-amplitude. The RPP immediately after the exercise session were higher than at baseline. For high frequency, low frequency of HRV and HR there was a main effect of amplitude.
CONCLUSION:
Small- and large-amplitude FBE increased significantly SBP, RPE, HRV, HR and induced lower DBP, but the changes were modest, suggesting that FBE impose no extra threats to cardiovascular stress.
Introduction
Vibration exercise is currently enjoying popularity as an alternative exercise modality for enhancing muscle strength, power and flexibility, with its mechanical vibration with low frequency (below 50 Hz) and low intensity transmitting the power to the whole body [1, 2, 3]. It has been suggested as an attractive and efficient complement to traditional forms of exercise for athletes, as well as elderly persons and patient populations [4]. Vibration exercise for the shoulder can for example be performed with a pole known as FLEXI-BAR or the Body-Blade [5].
The FLEXI-BAR
Therefore, examining the effects of FBE on acute cardiovascular responses is important for two reasons. First, for safety recommendations it is necessary to determine the level of cardiovascular stress experienced when engaging in FBE. Second, before subjecting heart patients to FBE in different intensities, determining the response in healthy individuals and dose-response relationship is ethically important. The objective of this study was to determine the acute effect of different FBE protocols on the BP, rate-pressure product (RPP), HR, heart rate variability (HRV), and rating of perceived exertion (RPE) among young healthy adults. It was hypothesized that the FBE intensity, postures performed, and their interactions would significantly influence the acute cardiovascular response. We hypothesized that larger intensity and larger degree of shoulder flexion would induce higher cardiovasular stress.
Methods
Experimental approach to the problem
A repeated measures randomized design was performed to determine the cardiovascular response to different FBE conditions.
Each participant underwent three different FBE intensities: (a) zero-amplitude (0 cm), (b) small-amplitude (5 cm) and (c) large-amplitude (20 cm) [3, 7, 13]. All participants performed one sessions only with one intensity FBE and they finished three different sessions in different day, with a minimum of one rest day in between. During each session, the participants were instructed to perform FBE in three different postures with the shoulder flexed in the following positions: (1) 180
Shoulder vibratory exercise in three different postures: a) shoulder flexed 180
The sample size calculation was based on a small effect size [represented by f score in analysis of variance (ANOVA)]. Based on the G*Power 3.1.9.2 ANOVA: Repeated measures, within factors was set, with 3 amplitudes and 3 postures, assuming the effect size: f
Participants were recruited at the Sun Yat-sen University from January to February 2018. The inclusion criteria were right-handed, young healthy adults (age from 20 to 39 years) who voluntarily joined this study. The exclusion criteria were upper extremity deficits, metabolic syndrome and cardiac dysfunction within the last year, and inability to perform FBE continuously for one minute. All participants signed an informed-consent document approved by the Office for Research Ethics of the Sixth Affiliated Hospital of Sun Yat-Sen University (SYSU). On a separate day before the experiment, participants were trained and learned to shake the FLEXI-BAR for at least one minute at each amplitude and specified position, and were taught to be familiarized with the experiment procedure and method. Before session, the participants were prohibitied to drink coffee or tea, smoke and so on.
Procedures
All experiments were conducted in an assessment room. The FLEXI-BAR
Before starting, individuals were instructed sit and rest for 5 minutes. The operator then measured baseline BP, HR and RPE. The individual rested around 2 minutes after these measurements meanwhile HR and HRV were recorded (Fig. 2).
The scheme of experimental session.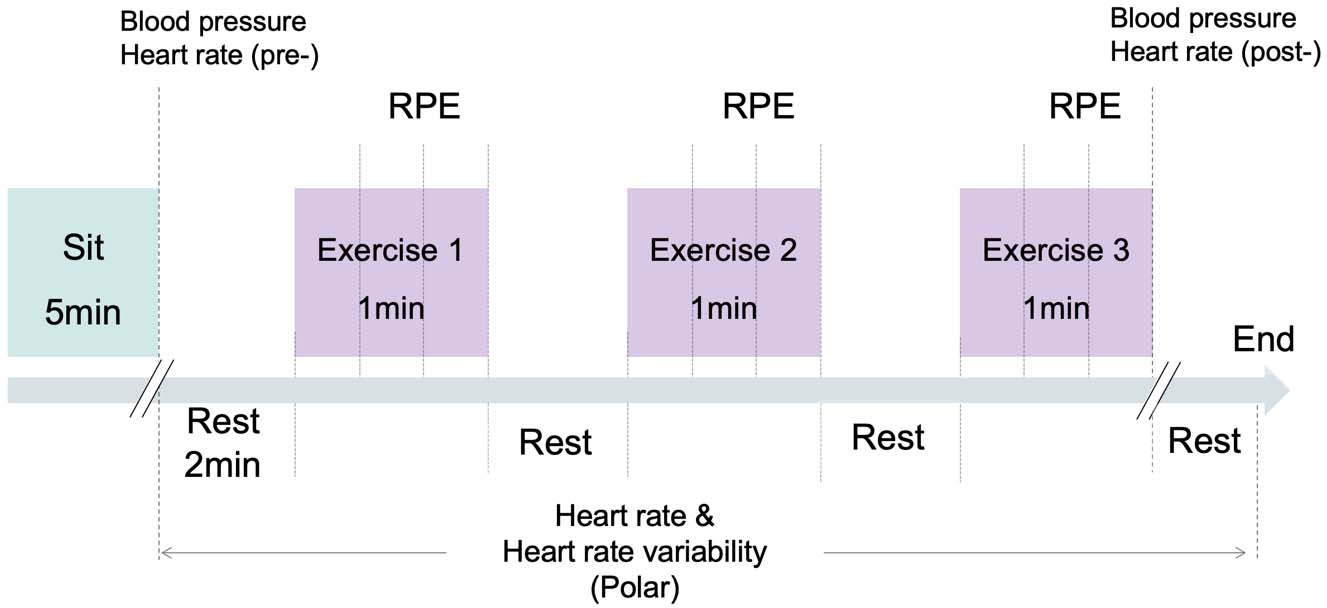
In the pilot study, we found that most participants felt extremely fatigued when performing large-amplitude FBE for more than one minute. Although the Task Force statement suggests a minimal of 2-minute recording to quantify the LF components of HRV while 1-minute to address the HF component, for recording and analysis of HRV at least one minute is required [15]. Thus, to balance the collection of data and the individual’s ability to maintain the required FBE, the duration of 1 minute was chosen in this study. After each exercise, subjects were asked to remain seated and rest until the HR resumed to baseline values before initiation of the next exercise.
The outcomes were diastolic and systolic blood pressure (DBP and SBP, in mmHg), heart rate (b
Before starting the following session, the participants were subjectively evaluated to determine whether they had recovered from the previous FBE session. In case of ongoing fatigue or soreness, the second and third sessions were rescheduled.
IBM SPSS Statistics software was used to statistically analyze the original data (Version 20.0, IBM, Armonk, NY, USA). The basic information was described as the mean and standard deviation. Paired
Another repeated measures ANOVA [(within-subject factors: 1. intensity [zero-, small-, large-amplitude FBE); and 2. Exercise posture (180
Other analyses were used to determine whether the cardiovascular changes were associated with the basic values. The after-session values subtracted the basic values forming the within-session change score, which represent BP and RPP data. As to HR and HRV data, the change score (before and after each session) was calculated by subtracting the baseline values from the after-exercise value. We performed Pearson’s product moment correlations to define the level of association between the change value and the basic score for all variables, respectively.
We set
Results
Characteristics of participants
A total of 36 participants were enrolled in this study (16 men and 20 women; mean age: 22.54
Baseline SBP, DBP, HR and HRV data of study participants
Baseline SBP, DBP, HR and HRV data of study participants
The flow chart of participants and path of testing.
a) Changes of the systolic blood pressure after vibration with different amplitudes; b) Changes of the diastolic blood pressure after vibration with different amplitudes; c) Changes of the rate-pressure product after vibration with different amplitudes.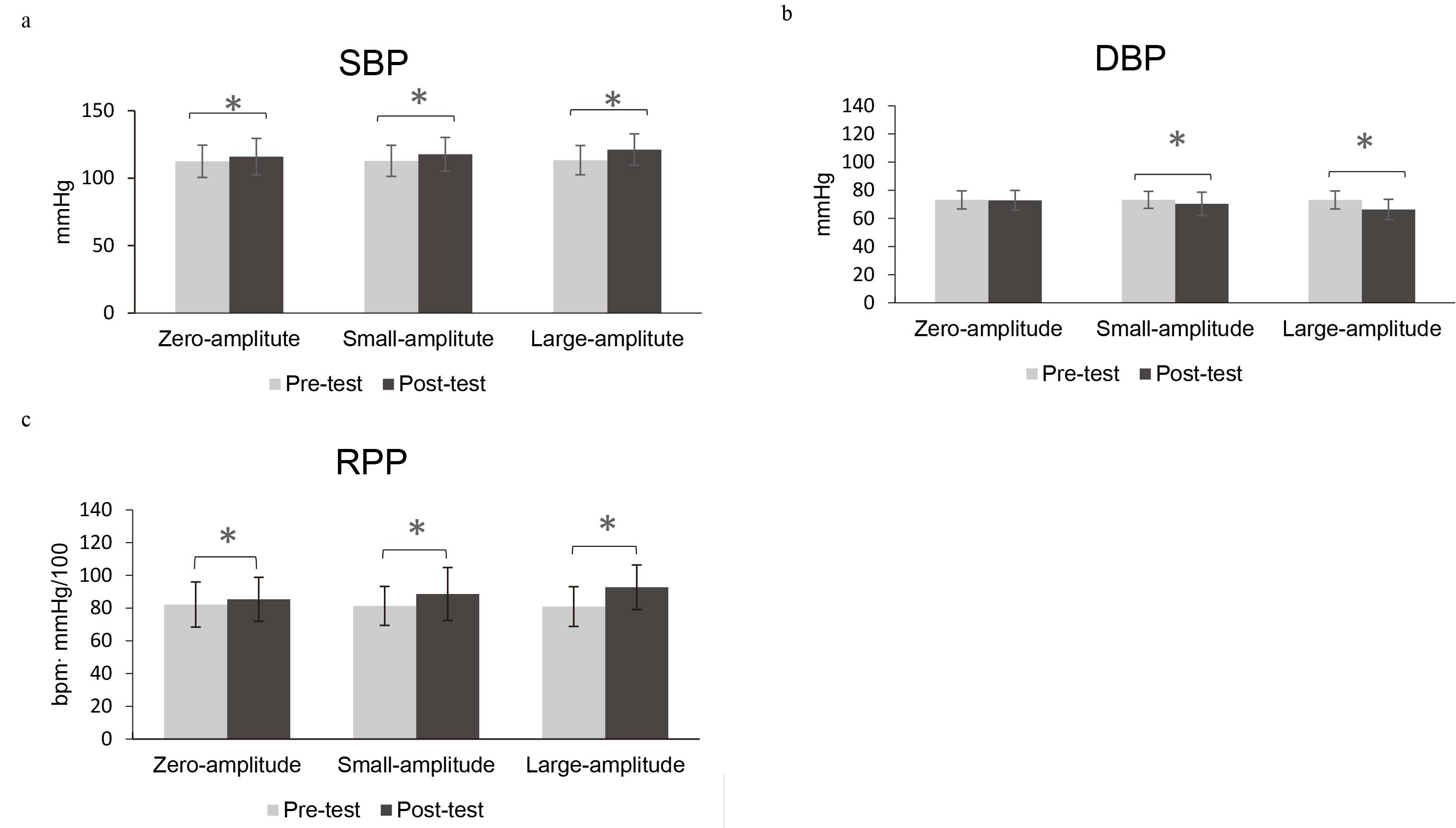
a) Effect of FBE amplitude on low frequency for heart rate variability; b) Effect of FBE amplitude on high frequency for heart rate variability.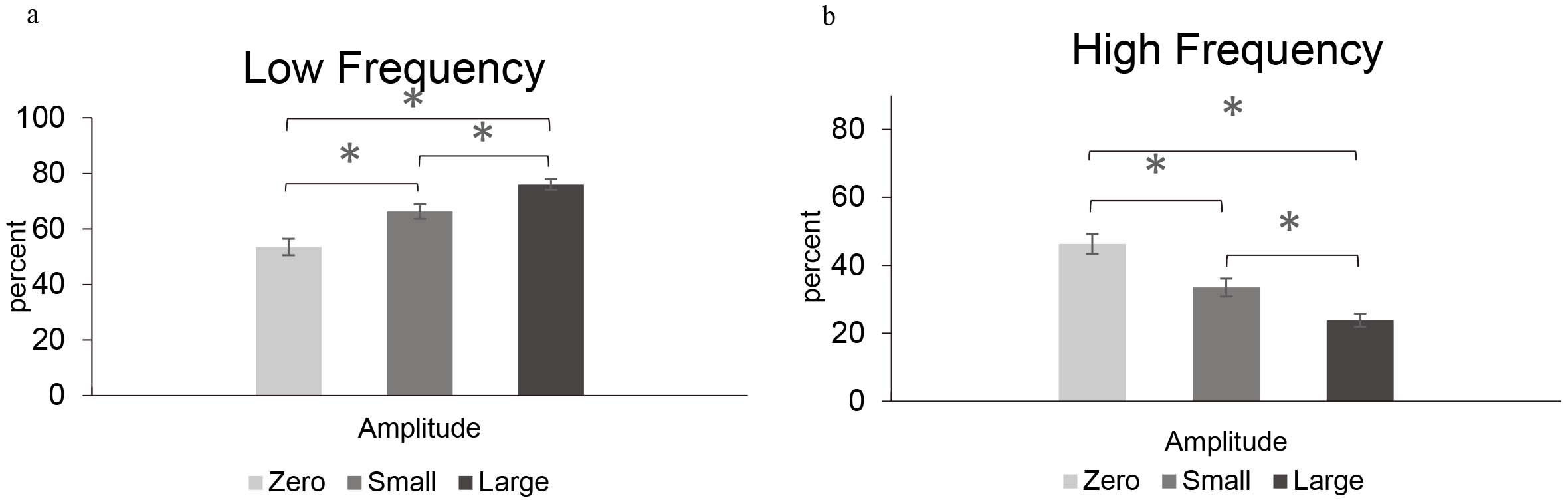
a) Effect of FBE amplitude on heart rate; b) Effect of FBE shoulder posture on heart rate.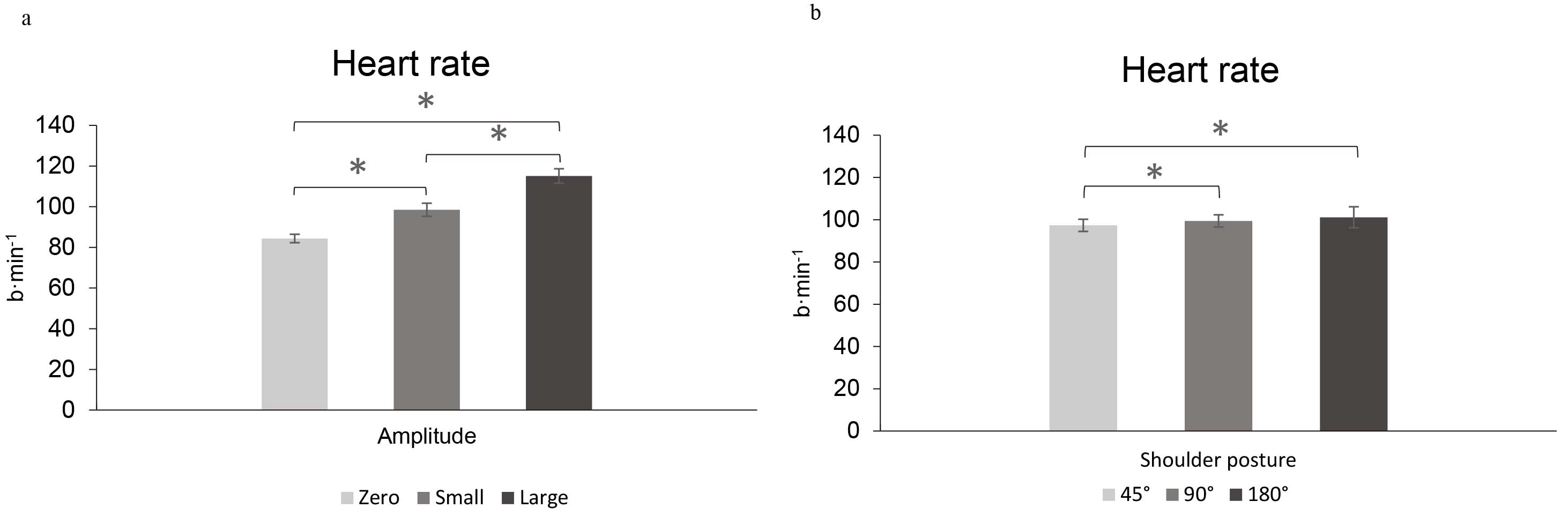
The correlation of washout period among all three sessions was interesting because the phase of session 1 and session 2 (mean 1.21 days, SD
Cardiovascular change
Systolic blood pressure, diastolic blood pressure, rate-pressure product changes
Effect of FBE on rating of perceived exertion using the Borg scale.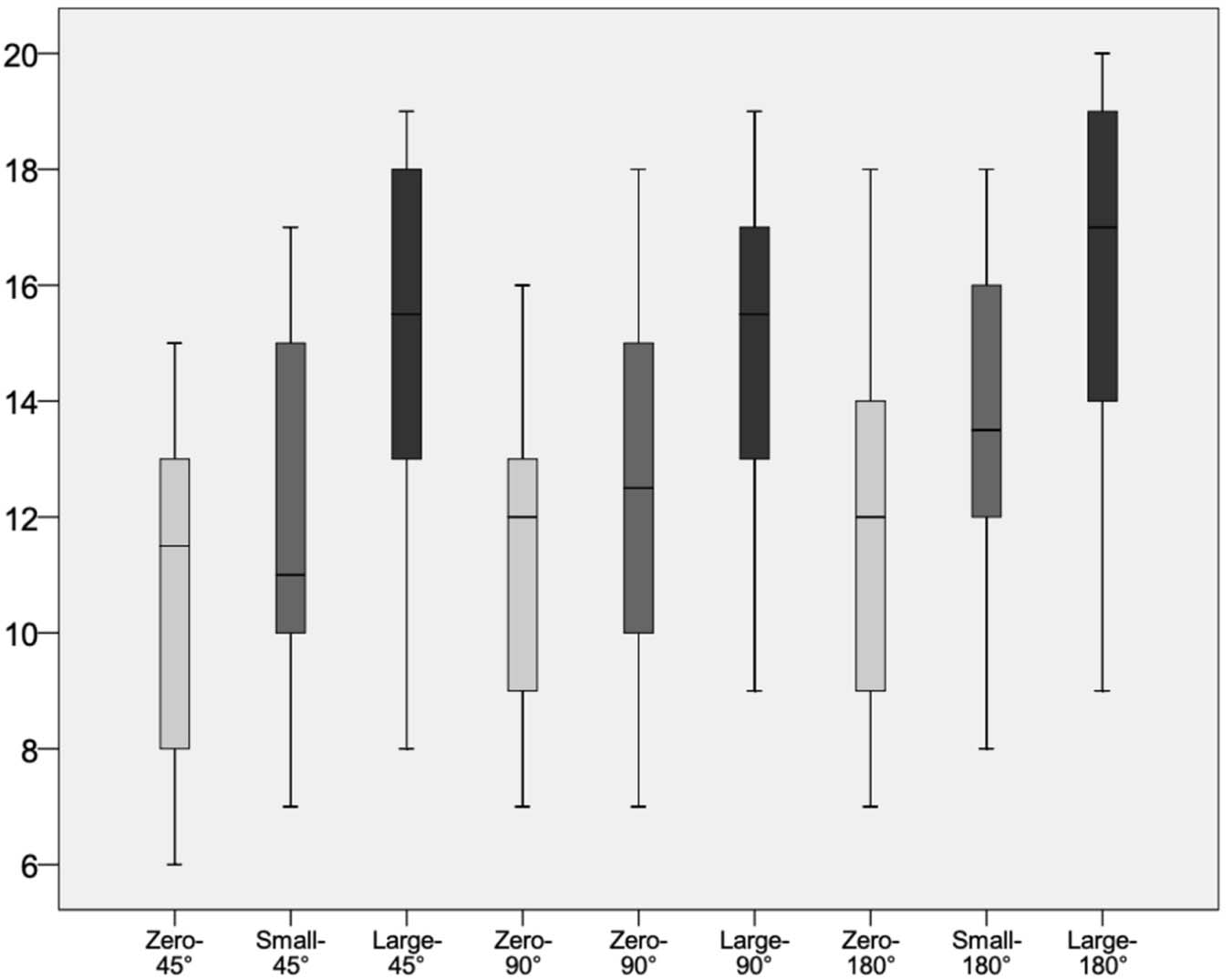
The amplitude
The RPP (F2, 666
| Amplitude*posture interaction effect | Main effect of amplitude | Main effect of posture | Post-hoc contrast analysis (main effect of amplitude) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Zero- Vs small-amplitude | Zero- Vs large-amplitude | Small- Vs large-amplitude | ||||||||||
| Variable |
|
|
|
|
|
|
Mean difference (95% CI) |
|
Mean difference (95% CI) |
|
Mean difference (95% CI) |
|
| HR | 1.47 | 0.232 | 93.71 |
|
8.78 |
|
|
|
|
|
|
|
| HRV-HF | 0.11 | 0.978 | 31.47 |
|
2.96 | 0.059 | 12.79 (5.60, 19.98) |
|
22.46 (15.47, 29.45) |
|
9.67 (2.36, 16.97) | 0.006 |
| HRV-LF | 0.11 | 0.979 | 31.30 |
|
3.02 | 0.056 |
|
|
|
|
|
0.006 |
The results of amplitude*posture interaction effect
A significant main effect of amplitude (F2, 66
Low frequency for heart rate variability
The main effect of amplitude (F2, 66
Heart rate response
There was a significant main effect of amplitude (F2, 62
Rating of perceived exertion changes
The pooled RPE data are shown in detail (Fig. 7). Out of the 315 FBE trials for each amplitude protocol (9 exercises
Association with the baseline values
The Pearson’ s product moment correlations results showed that no baseline RPP, DBP, and SBP in different amplitude was significant correlated with the respective change scores except for RPP (
Out of 9 different FBE posture and amplitude combinations (3 amplitudes
Discussion
FBE has been gaining popularity worldwide for many years, both for rehabilitation purposes as well as recreational training environments [19]. Investigating the acute cardiovascular response to FBE can provide critical evidence for physiotherapist to form the exercise intensity and ensure safety. This is the first study to examine the cardiovascular response to different FBE amplitude and posture in healthy adults. As hypothesized, the findings of the present study were that addition of large- and small-amplitude FBE increased significantly SBP, RPE, HRV, HR and induced lower DBP, but the increase and decrease was modest. Thus, it seems safe to test this protocol in patients, where after clinical recommendations can be provided.
Our study revealed that there was only mild increase in SBP (
Myocardial workload can be estimated by RPP which provide an indication of the amount of myocardial oxygen requirement [23]. The data suggests the RPP increase significantly after FBE, but there is not main effect of amplitude indicating that oxygen demand in different FBE amplitude should be similar. The histogram in chart indicates that the mean RPP at the end of FBE are 85, 89 and 93 for zero-, small- and large-amplitude respectively (Fig. 3C). This result is evenly much lower than the value induced by another kind of vibration exercise for frailty patients (mean value
One subject withdrew from the study because of hypertension before the trial began. It turned out that the subject had unstable blood pressure and was diagnosed with hypertension after being referred to the doctor. The remaining participants reported no adverse symptoms and signs, and none of them requested to end even one trial, indicating that the FBE protocols performed in our study were safe and fairly tolerated in healthy adults. We also found that the baseline values of SBP, DBP and RPP was not correlated with change of same value after different amplitude FBE. Therefore, FBE did not induce proportionally higher BP and RPP stress to the participants with high baseline scores.
Surprisingly, data demonstrates that 2% (4 participants, 6 trials), 8% (10 participants, 26 trials), and 26% (24 participants, 83 trials) participants reported an RPE
HRV has been applied to evaluating the exercise load [26]. According to the study results, the LF increase and HF decrease suggesting the enhancement of sympathetic activity and the inhibition of parasympathetic activity during the FBE. This finding also corresponds to one similar study which found that HF power significant decreased and LF power increased in immediately after passive vibration [27]. Interestingly, the LF (or HF) immediately after FBE showed significantly higher (or Lower) in the group performing the higher amplitude indicating that a more intense FBE amplitude distinctively enhanced sympathetic activity. This phenomenon may result from the more muscles activation that occurs with higher FBE amplitude.
Compared with no HR changes exerted by the passive whole-body vibration [28], the active FBE impose HR increased. We found that large-amplitude and small-amplitude significantly increased higher HR than zero-amplitude FBE, meanwhile large-amplitude had higher HR than small-amplitude FBE during exercise. Furthermore, the shoulder flexion to 180
Clinically, FBE may hold potential benefits especially for some patients with dysfunction of lower extremities as a kind of aerobic exercise training. In our study, the exercise intensities of large-amplitude FBE were mild compared with resting levels, and only occupied about 34% HR reserve. However, the intensities with addition of large-amplitude FBE were much lower than those moderate aerobic exercise training usually around 60% HR reserve [24, 29]. Besides, over 68% participants of the large-amplitude FBE have much higher RPE (
Limitations as well as strengths exist in our study. Firstly, the HRV components were recorded continuously within 1 min, limited by the length of each training session. The Task Force statement suggests a minimal of 2-min recording to quantify the LF components of HRV while 1-min to address the HF component [31]. The duration of HRV recording may thus lead to measurements that are not completely exact. However, this was equal during all conditions, allowing at least for comparison between conditions. Furthermore, considering the individual responses, the small- and large-amplitude FBE might led to soreness and high RPE for those unaccustomed to regular exercise. This might partially explain the various outcome of RPE changes in different subjects. Further research is needed to examine the cardiovascular stress of long-lasting FLEXI-BAR training (e.g. 2-min or 5-min) in well-trained and homogeneous populations, as well as in clinical populations with cardiovascular disease. Secondly, standardization of the amplitudes does not seem robust enough in our study. It is difficult for participants to continuously and accurately maintain the amplitude without visual or auditory feedback. Thus, using a custom-made rack combined with test leader’s continuous observation and oral correction can offer the visual or auditory feedback to reduce the amplitude deviation, and this method had been standardized in the pilot study. It would be better to use a device like amplitude-monitoring sensor with good validity. Finally, the training protocol with different shoulder flexion angle was limited in sitting position, which may reduce the neuromuscular output thus minimize the exercise intensity on cardiovascular system. Since the training posture could alter the effect of FBE, to what extent different posture may modulate the cardiovascular response will require further investigation.
Conclusions
This study shows that addition of large-and small-amplitude FLEXI-BAR training increased significantly SBP, RPE, HRV, HR and induced lower DBP, but the increase and decrease was modest, suggesting that shoulder vibratory exercises impose no extra threats to cardiovascular stress for young healthy people and the present protocol of FBE are probably unsuitable to be an aerobic training exercise. Further study is needed to examine whether shoulder vibratory exercise protocol would be safe and provide a favorable effect for patients in musculoskeletal rehabilitation.
Footnotes
Acknowledgments
This work was financlly supported by the National Natural Science Foundation of China (81472155) and Guangzhou Science, Technology and Innovation Commission (201802010039).
Conflict of interest
None to report.