
Abstract
BACKGROUND:
Recent clinical studies have revealed the advantages of using suspension devices. Although the supine, lateral, and forward leaning bridge exercises are low-intensity exercises with suspension devices, there is a lack of studies directly comparing exercise progression by measuring muscular activity and subjective difficulty.
OBJECTIVE:
To identify how the variations in the bridge exercise affects trunk muscle activity, the present study investigated changes in neuromuscular activation during low-intensity bridge exercises. We furthermore explored whether the height of the suspension point affects muscle activation and subjective difficulty.
METHODS:
Nineteen asymptomatic male participants were included. Three bridge exercise positions, supine bridge (SB), lateral bridge (LB), forward leaning (FL), and two exercise angles (15 and 30 degrees) were administered, thereby comparing six bridge exercise conditions with suspension devices. Surface electromyography and subjective difficulty data were collected.
RESULTS:
The rectus abdominis activity was significantly higher with the LB and FL exercises compared with the SB exercise (
CONCLUSIONS:
Relatively higher inclination angle was not effective in overall activation of the trunk muscles; however, different bridge-type exercises could selectively activate the trunk muscles. The LB and SB exercises could be good options for stimulating the internal oblique abdominis, and the erector spinae muscle, while the FL exercise could minimize the erector spinae activity and activate the abdominal muscles.
Introduction
Using an unstable surface to aid sports training and rehabilitation procedures is effective for activating targeted muscles and improving balance [1, 2, 3]. Previous clinical studies recommend using an unstable board, Swiss ball, and trampoline to increase muscle activity and enhance joint position senses [3, 4, 5]. Despite its effectiveness, difficulty controlling perturbation limits extensive application in patients [6]. Active use of unstable surfaces is generally restricted to athletic training or for patients in an advanced rehabilitation stage [2, 3].
Recent studies have suggested using suspension devices, hanging from the ceiling, as an alternative to unstable surfaces [6, 7, 8]. Exercises using a suspension device place the individual in a relatively lower position, such as lying down [7, 8]. Although latest clinical research has revealed the advantages of using suspension devices in rehabilitation procedures [9], further studies are necessary to identify a specific exercise protocol with this approach.
Previously, the effects of the bridge exercise applied with a suspension device have been demonstrated [10, 11]. It is one of the most frequently prescribed rehabilitation exercises for patients with low back pain or those requiring trunk muscle strengthening [7, 9, 12, 13]. The supine bridge (SB) progression with a suspension device reportedly helped to activate local abdominal muscles [12]. In addition, Guthrie et al. compared the effects of the traditional bridge exercise and the bridge exercise with a suspension device by measuring the thickness of the transverse abdominis and suggested that the bridge exercise with a suspension device is suitable for activating the transverse abdominis muscles [11]. However, these previous studies focused only on the SB; therefore, studies investigating the effects of various bridge exercise progressions with a suspension device are required.
The SB and forward leaning (FL) bridge exercises are effective in changing neuromuscular control of the erector spinae (ES) muscle [13]. Gwon et al. demonstrated that the side bridge exercise with a suspension device may alleviate pain and improve strength in patients with chronic low back pain. Although the SB, side bridge, and FL bridge exercises are of low intensity with suspension devices, there is a lack of studies directly comparing exercise progression by measuring muscular activity and subjective difficulty.
Suspension height is a major factor determining exercise intensity [5, 7, 10]. Though previous studies have shown that height of suspension influences the effect of the exercise [7, 10], contrasting results have also been reported. Lee et al. demonstrated that the height of the suspension point helps activate core muscle activity. In contrast, Calatayud et al. reported that a low-level suspension point can effectively stimulate the musculature. Therefore, the present study hypothesized that differences in the bridge form of exercise might activate the abdominal muscles differently.
In this study, we investigated changes in neuromuscular activation during low-intensity bridge exercises with a suspension device to determine whether differences in the bridge exercise affect trunk muscle activity differently. We furthermore aimed to determine whether the height of suspension affects muscular activation and subjective difficulty.
Methods
Participants
Using convenience sampling, participants were recruited from a local university. Sample size was determined using G-power 3.1.3 software, by setting two-way repeated measure design, significance level of 0.05, and power of 0.8. Absence of musculoskeletal disorder during the last six months was an inclusion criterion. To reduce biases due to differences between the sexes and concerns of disturbing signal due to fat tissue, the present study included only male participants with a body mass index
Averaged subjects’ demographic data
Averaged subjects’ demographic data
Surface electromyography (sEMG) data were collected using an sEMG device (QEMG-4/LXM3204, LAXTHA, Daejeon, Korea); signals were sampled with 1000 Hz frequency. The data obtained were computerized with the EMG acquisition software (Telescan 2.89, LAXTHA, Daejeon, Korea). Band-pass (20–450 Hz) and notch filters (60 Hz) were used. Four channels of surface electrodes were attached, running parallel to the muscle fibers, on the right (dominant) side of each participant. Sites of electrode placement were: of the rectus abdominis (RA) muscle was attached approximately 3 cm lateral to the umbilicus, of the internal oblique abdominis (IO) muscle was attached 1 cm medial and inferior to the anterior superior iliac spine, of the lumbar level of ES muscle was attached at the belly of the ES at the level of the third lumbar spine, and of the rectus femoris (RF) muscle was attached approximately at the midpoint at the line between the anterior superior iliac spine and patella [5, 16]. A ground electrode was placed on the anterior superior iliac spine. If hair was present, the skin surface was shaved and cleaned with alcohol. After attaching the electrodes, signal check was performed to get good electrode-skin contact.
For identifying the subjective difficulties of each exercise, Borg’s rating of perceived exertion scales (Borg 6–20 RPE scale) were used after performing each exercise. Borg designed the rating of perceived exertion (RPE) scale, which is widely believed to be one of the best indicators of the degree of physical strain [17].
Procedures
Before performing the exercise protocols, each participant performed two trials at maximal voluntary muscle contraction (MVC) for the included muscles against manual resistance. The primary researcher applied the maximal manual resistance for each muscle, according to specific protocols, following clinical literature on muscle testing [18]. The highest sEMG value of each muscle, recorded through testing each muscle, was used for subsequent normalization.
The present study administrated three bridge exercise positions, SB, LB, FL, and two exercise angles (15 and 30 degrees), and thereby compared six bridge exercise conditions with sling devices. During the exercises, distal portions of both the legs were placed in the sling suspension system (Redcord Trainer AS, Norway). The exercise sequence was randomly determined with each participant picking up six unidentified cards serially.
After 3 minutes of practice and rest for acclimation to each exercise, the participant performed the three types of bridge exercise with two exercise angles using sling device. For the SB, participants were in the supine position with neutral hip and knee extension. While making a line vertical to the ground between the axis of suspension and ankle joint; level of the ankle strap was determined by a wedge placed under the buttocks. Using digital inclinometer, 15 and 30 degrees inclination of wedge was ensured, and the wedge was subsequently removed during exercise procedures. For the LB, participants were in side-lying position with the right side towards the ground. Similar to the SB, level of the ankle strap was determined using a wedge placed under the right greater trochanter. For the FL, participants were instructed to place their elbows in slings supported by a suspension device while in the kneeling position and then to lean the trunk forward. The end posture was defined as maintaining a neutral pelvis and neutral lumbar lordosis with relaxation of the thorax with the head upright. The digital inclinometer set above the sling rod confirmed that the magnitude of leaning was 15 and 30 degrees.
During the three exercises, a neutral lumbar spine position was ensured by the examiner (anterior and posterior iliac spines in line), and the participant was instructed to maintain this position for 10 seconds, controlled by a metronome. The first and last 3 seconds were eliminated, and the activity from middle 4 seconds was used for further analysis. The participants were allowed to rest 3 min between trials.
Statistical analysis
The sEMG signal was calculated with root mean square formula and widow length set at 0.01 second. The data were averaged and demonstrated as %MVCs. The paired ratios between the RA, IO, and ES were also calculated. PASW Statistics (version 18.0; SPSS, Chicago, IL, USA) program was used to reveal the significant differences in %MVCs and Borg RPE scores among the exercise conditions. The Kolmogorov-Smirnov test was performed for the normal distribution of data before parametric statistical analyses. Adopting the two factors (bridge exercise types and exercise angles) in the present study design, two-way repeated ANOVA was performed to test for differences. For identifying each pair-wise comparison, the post hoc analysis with Bonferroni correction was performed. Throughout the analyses, set alpha level was 0.05.
Results
The mean values of normalized EMG data and Borg RPE score data are given in Table 2. Exercise angle significantly affected the muscular activities of RA, and Borg RPE score, which were significantly higher with a 30 degrees inclination, compared with 15 degrees (
The average and standard deviation of included muscle activities, ratio data, and Borg RPE score
The average and standard deviation of included muscle activities, ratio data, and Borg RPE score
Comparison of muscle activities during the different exercise conditions. 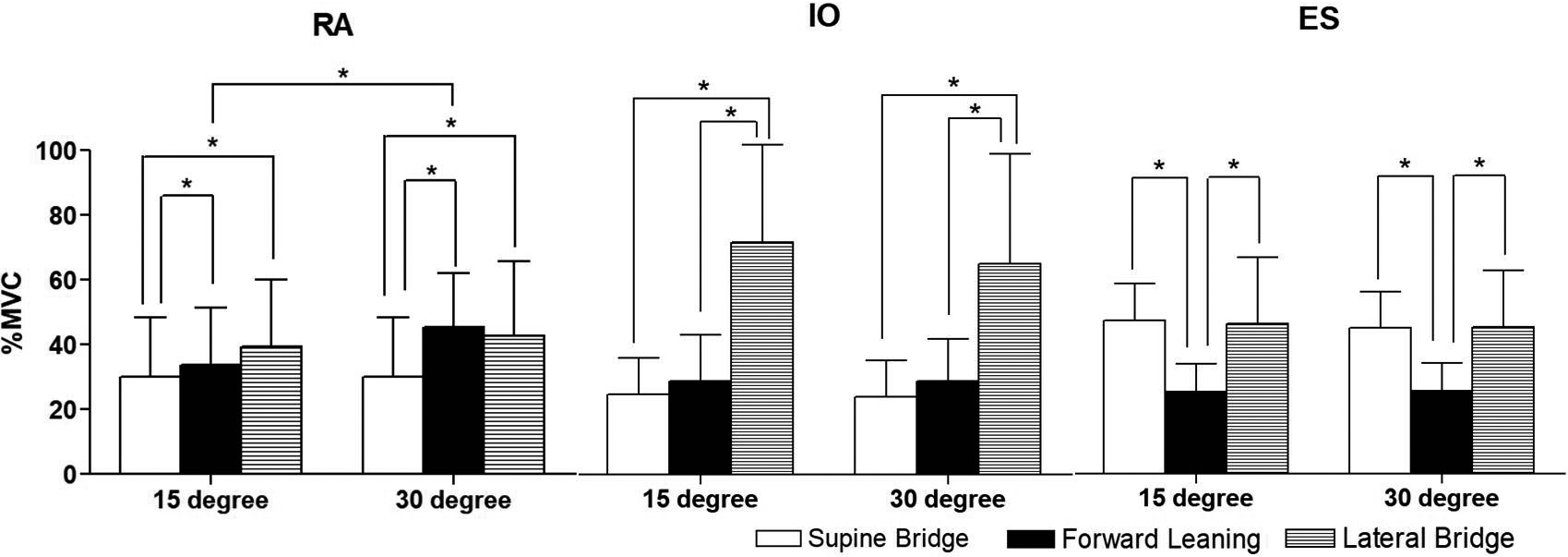
Comparison of ratio values and Borg RPE scale among the exercise conditions. 
Significant difference in RA, IO, ES, ratio values, and the Borg RPE score (
The bridge exercise with the LB position also showed significantly greater Borg RPE score than the exercises in the SB and the FL position (
The present study investigated the influence of exercise type and angle on trunk muscle activity and subjective difficulty during the three types of bridge exercises using a suspension device. Stevens et al. reported that stabilization exercises, including bridge exercises, improve trunk stability by activating the RA and IO muscles. However, the present results demonstrate that the bridge type of exercise activated the muscles at about 30–40% MVC, except the rectus femoris [19]. Considering that 30% MVC is insufficient to strengthen the abdominal muscles in an asymptomatic population [20], such bridge exercises with a suspension device might not be appropriate for symptomatic populations such as those with low back pain.
The LB exercise activated the internal oblique abdominis significantly more than other exercise conditions, regardless of the exercise angle. Moreover, the ratio between the IO and the RA in the LB exercise was higher than that of the SB and FL exercises. Previous studies have indirectly interpreted transverse abdominis muscle activity by collecting sEMG signals from the internal oblique site [5, 21], such as the IO with the transverse abdominis. Therefore, the LB exercise, as used in the present study, might be an effective option for selectively activating deep abdominal muscles. Studies on the LB exercise reported similar results regarding internal oblique activity. Escamilla et al. suggested that side positional bridge exercises are better for oblique and lumbar paraspinal muscle recruitment. Furthermore, it has also been reported that the side bridge exercise helps activate abdominal oblique muscles [5].
The present results show that the LB primarily activated the internal oblique abdominis, while the SB exercise demonstrated the highest ratio between the ES and the RA than other exercise conditions. The FL type of bridge exercise seemed inappropriate for increasing trunk muscle activity. However, it remains controversial whether a high level of muscular activation is a better exercise program for rehabilitation [23, 24]. Excess activation of the ES during relaxation phase was demonstrated in a participant with chronic low back pain [24]. Although the FL exercise does not activate the IO and ES muscles, it is effective for activating the abdominal muscles such as the RA.
The present results show significant differences in RA activity, IO/RA ratio, and ES/RA ratio between the exercise angles. A 30 degrees bridge type of exercise activated the RA more significantly compared with a 15 degrees exercise angle, similar to a previous study which reported that a high suspension position is effective for activating trunk muscles [10]. In contrast, the ratio was relatively higher with a 15 degrees exercise angle compared to 30 degrees. This manifests that selective activation of the IO and ES were preferentially accomplished with a relatively lower suspension.
The present study not only collected electromyography signals but also measured subjective difficulty by using the Borg 6–20 RPE as the perceived exertion scale. The muscular activation of the RA and IO were higher with the LB exercise. However, the Borg RPE was also higher than for other exercise conditions. The 13 points of the Borg RPE scale for the LB includes a “somewhat hard” level [17]. A previous study recommended that exercises with RPE
There are some limitations to the present study. First, we could not collect EMG data from both sides of the muscles influenced by the exercises, especially the LB. Second, the present study investigated only bridge exercises. Due to the high intensity of the plank type of exercises involving the upper extremities, the prone bridge and lateral plank exercises were excluded from this study.
Conclusion
The LB exercise is an excellent option for stimulating the IO abdominal muscles, and the SB exercise for the ES muscle. The FL exercise may be better than the SB or LB exercises to minimize ES activity and activate the abdominal muscles. A relatively higher exercise angle, by adopting a high-level suspension point, was effective for activating the RA but not the IO or ES muscles. Consequently, prescribing bridge-type exercises and adopting different exercise angles should selectively activate the trunk muscles.
Footnotes
Acknowledgments
This research was supported by Kyungsung University Research Grants of 2019.
Conflict of interest
The authors have no conflicts of interest to report.