
Abstract
BACKGROUND:
In clinical practice, knee flexion at the prone position for manual muscle testing of hamstrings and hip extension at the supine position for stretching of hamstring muscles are typically proposed.
OBJECTIVE:
Although different positions have been proposed for different purposes in hamstrings, the understanding of the changing the functional role of hamstrings with position changes is poorly understood.
METHODS:
The electromyographic (EMG) activity and hip extension force were compared among different postures; hip neutral, internal, and external rotation. EMG and force were measured in prone position during knee flexion and those were additionally measured in supine position during hip extension. In supine position, additional measurements were made in hip neutral, internal and external rotation.
RESULTS:
Hamstrings showed high EMG activity during knee flexion. Knee flexion force in prone position was significantly decreased at hip extension force in supine position. In supine position, EMG activity was significantly higher in semitendinosus (ST) than biceps femoris (BF) during internal rotation.
CONCLUSIONS:
It should be noted that bi-articular muscles may have different functional dependencies on the corresponding muscles for each joint. In addition, because the altered alignment of the hamstring muscles that was affected by hip rotation had a significant effect on muscle activity, and hip rotation may be helpful for selective training of medial or lateral hamstrings.
Introduction
In clinical practice, the conventional methods of physical examination and intervention for the hamstrings were passively accepted and performed without scientific inquiry. Currently, in manual muscle testing (MMT), hamstring contraction is induced by knee flexion in prone position, but in hamstring stretching, it is induced by hip extension in supine position. That is, the changes in the muscle activity of the hamstrings that occur during position changes and the joints involved are not given much consideration. An in-depth understanding is needed to establish an effective treatment strategy for the hamstrings.
The hamstrings are divided into the medial hamstring (MH) and lateral hamstring (LH) according to anatomical location. The MH includes the semimembranosus (SM) and semitendinosus (ST), whereas the LH includes the biceps femoris (BF). The MH and LH seem to have the same functional role, as both are involved in knee flexion and hip extension; however, in tibial rotation, the MH plays a role in internal rotation (IR), whereas the LH participates in external rotation (ER). In fact, although the hamstring muscles perform the same action during knee flexion or hip extension, the amount and sequence of muscle activation differ between the MH and LH. For example, the LH is initiated first and the MH is subsequently activated during gait with transition from the swing to the stance phase. This timing can be reversely changed in anterior cruciate ligament (ACL) deficiency [1, 2].
The MH and LH show different electromyographic (EMG) activities during movement in the sagittal plane and EMG activity ratios during axial rotation in the transverse plane [3, 4, 5, 6]. For this reason, during MMT, measurements should be made separately for the MH and LH after applying tibial rotation [7]. For example, in MMT of the MH, the patient is placed in prone position with
In this study, EMG activity and muscle force were measured during maximal voluntary isometric contraction (MVIC) at knee flexion in prone position and at hip extension in supine position, and comparisons were made between the positions. In addition, the effects of hip rotation on the EMG activities of the MH and LH were investigated.
Materials and methods
Participants
A total of 32 adults (18 men and 14 women; age, 20.8
Instrumentation
The EMG activity of the hamstrings was measured using a Delsys-Trigno Wireless EMG system (Delsys Inc., Boston, MA, USA). The sampling rate was 2,000 Hz, and the band pass filter was set in the range of 20–450 Hz. A notch filter of 60 Hz was used. Delsys EMGWorks Acquisition was used for data collection, and Delsys EMGWorks Analysis 4.3.1.0 was used for data analysis. The amplitude of the EMG signals was quantified by the root mean square (RMS) value. Muscle force was measured using a tension gauge (Re-live Inc., Jeonju, Korea), and data were recorded in real time on a laptop connected via Bluetooth. A tension gauge connected to a sling was provided to measure the muscle force during MVIC.
Characteristics of the subjects
Characteristics of the subjects
Force measurements using a tension gauge in the prone position during knee flexion (a) and in the supine position during hip extension (b).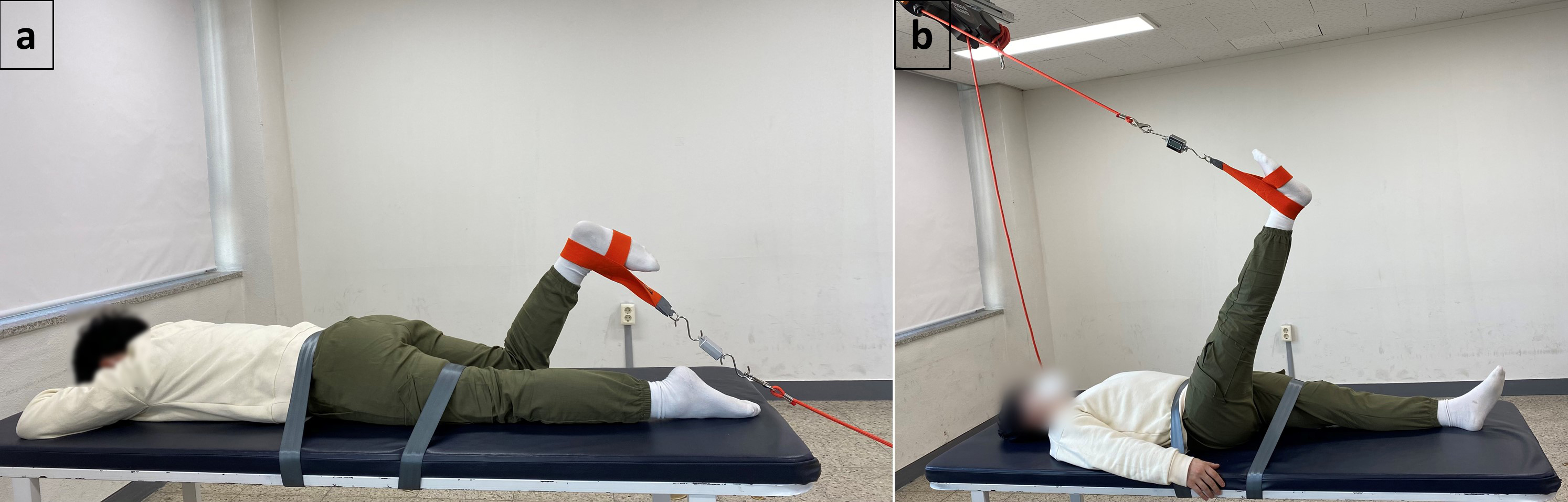
Forces measured at four different positions during maximum voluntary isometric contraction
Data are presented as mean
The subjects lay prone on the treatment table for EMG measurement in the MMT position. The participants’ self-reported dominant leg and the pelvis and non-dominant leg were fixed to the treatment table with straps [14]. For the dominant leg, the distance from the lateral epicondyle of the femur to the lateral malleolus of the fibula was measured using a (nylon-coated stainless steel blade) measuring tape and recorded as an external moment arm. MVIC was conducted three times during tibial neutral rotation (NR) at 60
Influence of hip rotation on electromyographic activity (% Max)
Influence of hip rotation on electromyographic activity (% Max)
Data are presented as mean
The Shapiro-Wilk test was used to determine the normality of the data. The significance of age, height, weight, and force between the groups was verified using an independent-samples
Results
Age, height, and weight did not show any significant differences between groups A and B (Table 1). The knee flexion force in NR measured in the MMT position was significantly higher compared with the hip extension force in both IR (
Electromyographic (EMG) activity of the hamstrings during maximal voluntary hip extension contraction, normalized to the EMG activity during maximal voluntary knee flexion contraction. *Significant difference compared with NR (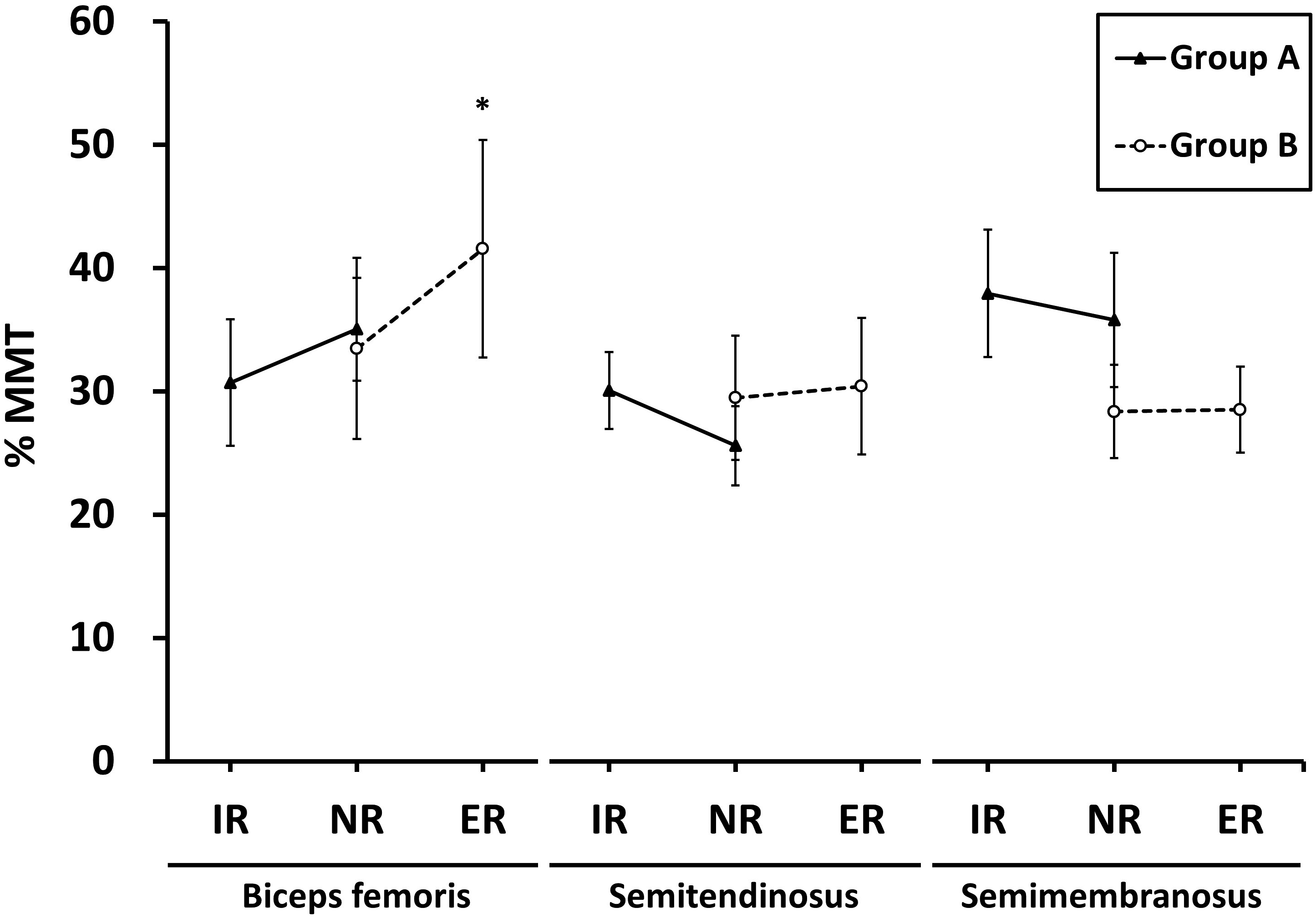
The % MMT was calculated by normalizing the values measured at hip rotation in supine position (Fig. 2). The EMG activities of the ST and SM tended to decrease in NR as compared with IR and to increase in ER as compared with NR. By contrast, the BF tended to show an increasing % MMT in the order of IR, NR, and ER. The EMG activity in ER was significantly higher than that in NR (
The % Max calculated in terms of the percentage to the highest EMG value measured among the different hip rotation positions in supine position (Table 3) [17]. The change in % Max according to hip NR was significantly higher in the SM than in the BF in group HER (
Discrepancy in functional role of the hamstrings as a knee flexor or hip extensor
The hamstrings are the primary hip extensor and knee flexor. The hip extension force of the hamstrings measured in this study was significantly lower than the knee flexion force by 17.73–27.11%. If the internal torque from the muscle during maximum isometric contraction does not change, the same external torque value should be provided in the opposite direction. The external force, which is the resistance in this study, and the length of external moment arm constituting the external torque are inversely proportional. During both hip extension and knee flexion, maximal resistance was exerted on the ankle; however, because of the different locations of the rotation axis, the length of the external moment arm in hip extension was about twice as long as that in knee flexion. If the internal torque of the hamstrings was the same in both positions, the inversely proportional external force should be halved in supine position because the external moment arm length was doubled. However, the decrease in the measured values in this study was less than that. This indicates that the internal torque of the hip extensors was higher than that of the knee flexors. This discrepancy can be explained by the difference in the net force produced during hip extension and knee flexion. Unlike the EMG activity, force does not reflect a single value from a particular muscle but rather the net result of all the muscles involved in the movement. In hip extension, the gluteus maximus (GM) and posterior head of the adductor magnus participate as primary muscles in addition to the hamstrings, and the middle and posterior heads of the gluteus medius and the anterior head of the adductor magnus participate as secondary muscles [18]. Unlike during knee flexion, many other muscles contribute to torque generation during hip extension.
When the hamstrings acted as a hip extensor in supine position rather than as a knee flexor in prone position, the EMG activity decreased by 58.44–74.40%. The reduced EMG activity in supine position can be partly explained by several factors. First, it can be due to increased muscle length. When the knee and hip joints were tested at various angles from 0
Effect of hip rotation on force and EMG activity
If the knee joint is locked by full knee extension, hip rotation can be partially affected by the hamstrings. For the knee joints, the shape and length of the medial and lateral femoral condyles differ, and this causes tibial ER in the last 20
This study might be the first to investigate the force and EMG activity of the hamstrings according to hip rotation. The force remained constant with no decrease in both IR and ER as compared with that in NR. Although some decrease in EMG activity was observed in individual muscles during hip rotation, the net force was constant because of the corresponding increase in other muscles. For example, the % Max of the BF decreased in IR but increased in both the ST and SM. Another possibility is that the changes in the EMG activity may not directly lead to changes in muscle force. At increased muscle lengths, fewer motor units can produce the same torque as that in the case of shorter muscle lengths [5, 19, 34]. In previous studies on tibial rotation, a significant decrease in force was observed only in IR, which was believed to be due to the reduced EMG activity of the LH [27]. In this study, in terms of EMG activity, the BF showed high agreement with the inference with respect to the anatomical location, and ST and SM showed some agreement in relative comparison. The BF showed a significantly increased % Max in ER as compared with NR and a minimum value in IR. The reason for the increased EMG activity of the BF in ER would be that the direction of the muscle fibers, which was inserted in the lateral side of the head of the fibula and twisted from the ischial tuberosity, was closely aligned in a straight line with the hip rotation, which led to more efficient muscle contraction. In the ST and SM, % Max tended to increase in both muscles in IR as compared with NR, and the ST showed significantly higher % Max in IR than the BF. In the previous study, unlike the SM, the EMG activity of the ST was stable even at short muscle lengths [35]. In conclusion, hip IR and ER positively affected the EMG activities of muscles that were anatomically related.
Conclusion
The findings of this study suggest that the involvement of the hamstrings was greater during knee flexion than during hip extension. Bi-articular muscles may have different functional dependencies for each involved joint. In clinical practice, selective training of the MH and LH through hip rotation may be possible to some extent. In particular, if the timing of the MH and LH is changed, as in the case of ACL deficiency, hip rotation may be applicable because differentiation of the MH and LH is required during rehabilitation [1, 2].
Footnotes
Acknowledgments
This work was supported by 2019 Woosong University Academic Research Funding, and the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education [NRF-2017R1C1B5076885].
Conflict of interest
None to report.
Ethical considerations
This study was approved and monitored by the Institutional Review Board of Woosong University (1041549-180419-SB-59).