
Abstract
BACKGROUD:
Reliable scapular upward rotation and anterior-posterior tilt data are required for patients with subacromial impingement syndrome (SIS). Only a few studies have explored the reliability of such measurements derived using a modified inclinometer.
OBJECTIVES:
To determine the relative and absolute reliability of scapular upward rotation and anterior-posterior tilt measurements derived using a modified digital inclinometer in patients with SIS.
METHOD:
Seventeen SIS patients were assessed twice within 1 week. We determined the relative and absolute measurement reliability by calculating the intraclass correlation coefficient (ICC), standard error of measurement (SEM), and minimal clinically important difference (MCID). Both intra- and interrater reliability were determined.
RESULTS:
The intra-rater reliability (both measurements) was high (0.72–0.88), and the interrater ICC was high to excellent (0.72–0.98). Clinically acceptable SEM and MCID values were obtained for scapular upward rotation (SEM: 4.28–9.33
CONCLUSIONS:
Measurements of scapular upward rotation and anterior-posterior tilt using a modified digital inclinometer reliably reveal scapular position and kinematics in patients with SIS.
Keywords
Introduction
Subacromial impingement syndrome (SIS) is the most common type of shoulder injury, accounting for 44–60% of all complaints of shoulder pain [1]. The injury mechanism may be either intrinsic or extrinsic. Intrinsic factors are joint problems, such as changes in the shape of the acromion process. Extrinsic factors include changes in periscapular muscle activation and/or scapular position/kinematics [2]. Scapular upward rotation and posterior tilt are decreased during shoulder elevation in SIS patients compared to healthy subjects; this triggers SIS by narrowing the subacromial space, and the acromion process moves forward and downward [3, 4, 5]. Therefore, measurements of scapular upward rotation and anterior-posterior tilt are required to identify SIS problems and treatment effects.
Various methods of measurement have been used to these ends. Lukasiewicze et al. [6] and Turgut et al. [7] measured scapular position and movements using a three-dimensional motion analyzer (3DMA) and found that posterior tilt was reduced in SIS patients compared to normal subjects. McClure et al. [8] similarly measured scapular kinematics in SIS patients and found that upward scapular rotation was reduced. In previous study, it was reported that the reliability of 3MDA was 0.88–0.97, which is excellent [9]. Watson et al. [10] reported that a dual inclinometer reliably measured shoulder upturn in patients with shoulder pain (intraclass coefficient [ICC]: 0.81–0.94). However, 3DMAs are expensive laboratory instruments, and it is difficult to set-up to measure the scapula anterior-posterior with a dual inclinometer. There is a need for a device that easily measures scapular upward rotation and anterior-posterior tilt in the clinic setting.
Recently, a modified digital inclinometer (featuring rotator rods) was used to these ends; it easily measured scapular position and movement, and the measurements could be checked digitally. Johnson et al. [11] assessed the reliability and validity of using such an instrument to measure scapular upward rotation in healthy subjects and those with shoulder pain. The validity (compared to that of active magnetic tracking) was 0.74–0.92, and the reliability was 0.89–0.96. Scibek et al. [12] reported that the reliability of scapular anterior-posterior tilt measurement was 0.93–0.99, and the validity was 0.63–0.86 in healthy subjects [13].
As SIS patients exhibit less scapular upward rotation and posterior tilt during shoulder elevation than normal subjects, reliable measurement methods are needed to identify scapula problems in SIS patients and provide appropriate intervention programs. Although the assessment of scapula upward rotation and posterior tilt using a modified inclinometer can be easily used in clinical practice and are reliable methods, there are no studies measured in SIS patients. In clinical practice, patients with SIS are evaluated for both movements, but if the reliability of the two scapula motions tests is measured separately, bias may occur due to the influence of various factors (characteristics of subjects, environment, etc.). So, it may be important to measure the reliability of both tests together, however no study exists on the use of a (reliable) modified inclinometer [11, 13] to simultaneously measure scapular upward rotation and anterior-posterior tilt. In addition, upward rotation and anterior-posterior may be measured repeatedly by the same therapist depending on the course of treatment, but in some cases, it may be measured by another therapist. So, in order to confirm whether it is a useful test method that can be used clinically, it is necessary to measure the reliability within and between testers. However, in previous works, only intrarater (not interrater) reliability was assessed.
Therefore, we measured the relative and absolute intra- and interrater reliability of scapular upward rotation and anterior-posterior tilt measurements derived using a modified inclinometer. We compared SIS patients to normal subjects.
Demographic characteristics of the participants
Demographic characteristics of the participants
Abbreviations: SD, standard deviation.
The modified digital inclinometer.
Measurement of scapular upward rotation. A: Resting position, B: shoulder elevation 60
Scapular palpation point of the inclinometer for measurement of upward rotation (A) and anterior-posterior tilt (B).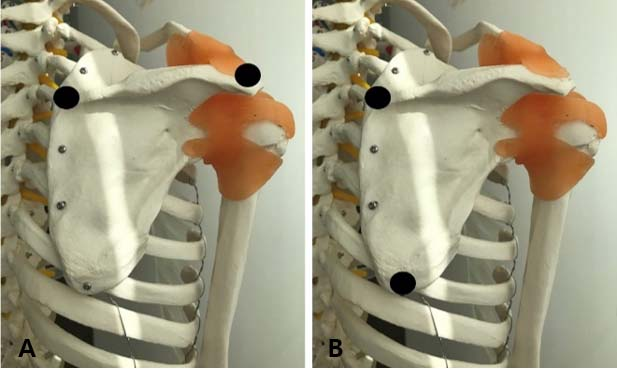
Measurement of scapular anterior-posterior tilt. A: Resting position, B: shoulder elevation 60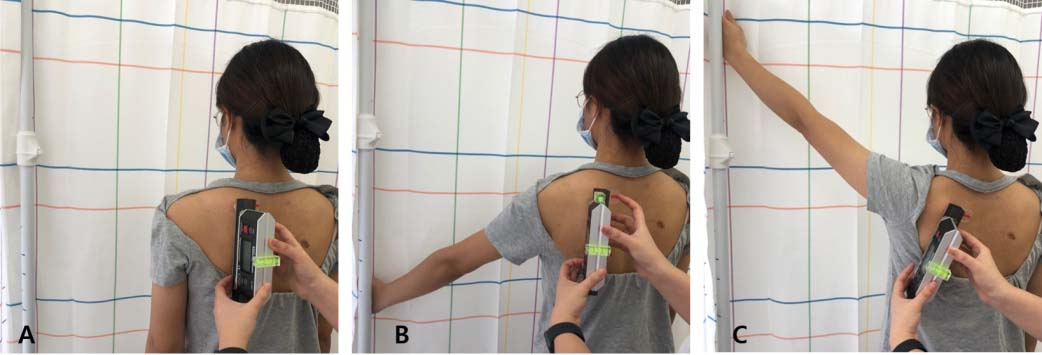
Participants
This cross-sectional study enrolled 17 SIS outpatients (male: 9, female: 8) diagnosed by a rehabilitation physician with unilateral shoulder pain. Inclusion criteria were a shoulder pain score on a visual analog scale of 3–7; shoulder flexion of 120
Procedure
Scapula upward rotation and anterior-posterior tests were performed twice within 1 week and it was measured again a week after the initial measurement to measure the intra-reliability. All testers were measured by two examiners, examiner 1 has 3 years of clinical experience and examiner 2 has 14 years of clinical experience. All participants completed demographic questionnaires prior to the measurement of scapular upward rotation and anterior-posterior tilt. Examiner 1 attached markers to the scapular inferior angle, posterolateral acromion, and scapular spine root. The unaffected side was measured, followed by the affected side, at various shoulder elevations. When the test of examiner 1 was completed, the marker was removed, and the marker area was wiped with alcohol. Because participants may feel tired, examiner 2 conducted the same method after 20 minutes. These subsequent measurements were collected after 1 week. Participants were asked not to engage in sporting activities that may affect the examination for one week.
Measurement of scapular upward rotation and anterior-posterior tilt
A modified digital inclinometer (Fig. 1) was used to measure scapular upward rotation and anterior-posterior tilt. A cuboid was used to install two rods and cylinders on a modified digital inclinometer. To measure anterior-posterior tilt, two cylinders 1 cm in diameter and 2 cm in height were attached under the cuboid. To measure upward rotation, two plastic locator rods (approximately 7 cm in length) were attached between the cuboid and the cylinders. The left cylinder and rod were fixed, but the right cylinder and rod were movable and were adjusted to abut the scapula. A small bubble was placed on top of the inclinometer to ensure that the inclinometer was perpendicular to both the horizontal and sagittal planes during measurement [11, 13]. Scapular upward rotation was measured with subjects in the resting position (Fig. 2A) and then with the shoulder elevated to 60
Scapular anterior-posterior tilt was measured in the resting position and at shoulder elevations of 60
Statistical analyses
The Kolmogorov-Smirnov test was used to confirm that parameters were normally distributed. We estimated relative intra- and interrater reliability by deriving ICC
Intra-rater reliability of scapular upward rotation and anterior-posterior tilt measurements
Intra-rater reliability of scapular upward rotation and anterior-posterior tilt measurements
Interrater reliability of scapular upward rotation and anterior-posterior tilt measurements
Absolute reliability of scapular upward rotation and anterior-posterior tilt measurements
Abbreviations: UR, upward rotation; APT, anterior-posterior tilt.
The difference of scapula upward rotation and anterior-posterior tilt between affected and non-affected side
The intra-rater relative reliability for scapular upward rotation (examiner 1: 0.79–0.86, examiner 2: 0.81–0.87) and anterior-posterior tilt (examiner 1: 0.72–0.80, examiner 2: 0.84–0.88) measurements on the unaffected side was high. The intra-rater reliability for upward rotation (examiner 1: 0.72–0.86, examiner 2: 0.75–0.81) and anterior-posterior tilt (examiner 1: 0.79–0.81, examiner 2: 0.79–0.81) measurements on the affected side was also high (Table 2). The interrater relative reliability of scapular upward rotation measurements (both sides) was high to excellent (0.81–0.98), and the relative reliability of scapular anterior-posterior tilt measurements (both sides) was high (0.72–0.88; Table 3). The absolute reliability of upward rotation measurements ranged from 4.3 to 9.3
Discussion
We explored whether scapular upward rotation and anterior-posterior tilt are reliably measured using a modified inclinometer in patients with SIS. Both measurements exhibited high intra- and interrater reliability. The intra-rater relative reliability was high to excellent because, first, skin palpation was used to assess scapular position and movement. In an autopsy study, Lewis et al. [15] investigated the validity of this method. The difference in measurements was only 0.46–1.46 cm compared to when a pin was placed on the scapular landmark; skin palpation validly assessed scapular position. We used skin palpation to measure scapular upward rotation and anterior-posterior tilt. The scapular posterolateral acromion, inferior angle, and spine root protrude and thus are easy to palpate. Second, the inclinometer was modified. As the scapula is slightly rounded, error may be introduced if the inclinometer is attached directly to the scapula. Therefore, we attached locator rods and cylinders to the inclinometer and placed them on previously palpated scapular landmarks. Reliability was high to excellent because the inclinometer body remained vertical at all times. Johnson et al. [11] found that the ICC of scapular upward rotation measurements using a modified digital inclinometer was 0.89–0.96 for those with and without shoulder pain. Tucker and Ingram [16], working with healthy males, found values of 0.892–0.975 (good). In another study, the reliability of scapular anterior-posterior tilt measurements using a modified inclinometer was excellent (0.97–0.99) [12]. The method is reliable.
We are the first to derive interrater reliability for simultaneous assessment of scapular upward rotation and anterior-posterior tilt using a modified inclinometer. The ICCs were high to excellent, for the reasons given above. Examiner 1 had 3 years of clinical experience, and examiner 2 had 14 years of experience. Thus, even less experienced clinicians produce reliable results. The method is simple.
ICCs usefully evaluate the reliability of equipment and measurement methods [17], but they do not provide information on variation. The ICC is a proportional exponent of reliability; error variance is biased by between-object variance [18]. The SEM is the variation that can be caused by measurement inaccuracies or noise [19]. The SEM and MCID are clinically relevant measures [20] and thus more meaningfully interpret measurement data and identify differences between two measurements. Our SEM for scapular upward rotation was higher than those of Tucker et al. [16] (1.1–1.8
We found no significant difference in either upward rotation or anterior-posterior tilt between the affected and unaffected sides. There are two reasons for this. Although scapular position is influenced by the dominant arm [21, 22], our patients were mismatched in terms of the affected side and the dominant arm. In addition, changes in neuromuscular control came into play. SIS patients exhibit less upward rotation and posterior tilt than normal subjects [6, 7, 8]. These movements are generated by periscapular muscles, and changes in muscle activation patterns on the affected side influence the unaffected side [3, 23]. Unilateral arm muscle activity increases tension in the opposite-side shoulder and neck muscles [23].
In order to identify the problems of patients with SIS and to determine the effectiveness after treatment, the measurement of the scapula upward rotation and anterior-posterior tilt is necessary. Scapula upward rotation and anterior-posterior tilt measurements using a modified inclinometer in patients with SIS was showed high reliability. In addition, the reliability between the examiners measured by the examiner with much clinical experience and the examiner with little clinical experience was also high. Therefore, the measurement of scapula upward rotation and posterior tilt using a modified inclinometer can be consider as a reliable method that anyone can measure regardless of the degree of clinical experience. Also, this equipment has the advantage of being easy to use in clinical practice because it is inexpensive and does not require high-level technology. Therefore, we recommend using a modified inclinometer for evaluating the scapula upward rotation and anterior-posterior tilt in patients with SIS.
This study has some limitations. First, scapular upward rotation and anterior–posterior tilt were measured to shoulder elevations of only 120
Conclusions
We evaluated the reliability of scapular upward rotation and anterior-posterior tilt measurements made using a modified inclinometer in SIS patients. Intra- and interrater reliability were high to excellent. The modified inclinometer reliably evaluates such patients.
Footnotes
Acknowledgments
None.
Conflict of interest
The authors have no conflict of interest to report.