
Abstract
OBJECTIVE:
The purpose of this study was to investigate differences in regional lumbar lordosis (RLL) and global lumbar lordosis (GLL) angle during slumped sitting and upright sitting among three global subgroups.
METHODS:
A total of 48 young asymptomatic volunteers stood in a comfortable posture, sat upright, and sat in a slumped position for 5 seconds, with inertial measurement units attached to the T10, L3, and S2 vertebrae. According to standing measurement, the participants were categorized into flat-back (GLL
RESULTS:
Both the GLL and RLL in the flat-back group were reduced lumbar lordosis in the upright sitting posture and increased lumbar kyphosis in the slumped sitting postures compared to the other groups (
CONCLUSIONS:
Flat-back posture is a potential source of low back pain during both upright and slumped sitting compared to the normal and hyper-lordosis groups. Posture measurements in a standing and sitting position conducted to assess lordosis should consider the relationship between GLL and RLL.
Introduction
The sagittal plane contour of the human vertebral column comprises a series of reciprocal curvatures that conduce an ideal posture during standing [1, 2]. Balanced sagittal postures such as upright posture are a key point of evaluation and intervention in musculoskeletal pain and surgical planning. Lumbar spine lordosis is a particularly important factor for maintaining a good upright posture and healthy load bearing [1]. However, many other factors influence lumbar lordosis including pelvic orientation, trunk muscle balance, movement pattern, and posture [2, 3, 4, 5].
The relationship between sitting posture and low back pain (LBP) remains controversial among researchers and clinicians [6, 7]. Many previous studies have reported the adverse effects of sitting posture [8, 9]. In the sitting position, the lumbar lordotic curve tends to decrease or flatten compared to the standing position. A change in the lordotic curve between sitting and standing could be caused by the position of the hips. Hip flexion promotes a kyphotic lumbar curve, which makes it difficult to achieve and maintain lumbar lordosis during sitting [3, 4]. Thus, reduced lumbar lordosis during sitting may have adverse consequences, increasing the load and intradiscal pressure on the lumbopelvic region compared to the standing position, and causing discomfort or pain to this region [10].
Several previous studies have reported a lack of evidence for a direct link between sitting and the risk of LBP among sedentary workers [6, 7]. Interestingly, not all subjects who perform prolonged sitting develop LBP, and only 20–50% developing transient LBP [11, 12]. Several studies have suggested that during long periods of sitting, more flexed postures such as slumped sitting are more likely to provoke discomfort than more extended postures. A slumped sitting posture is one of the most common sitting postures while working at a computer or using a smart phone, and it has been associated with back problems in both clinical and research studies [13, 14]. Previous studies have also explored the adverse effects of a slumped sitting posture on movement and muscle activation [15, 16, 17]. Increased trunk flexion transfers weight-bearing onto passive tissues and leads to increased stress on the muscles, ligaments, bones, and intervertebral disks. This is because the altered vertebral curvature modifies the interaction between gravity and each spinal region. In addition, the flexion-relaxation phenomenon, involving inhibitory responses of the back muscles where the transition of load moves toward other passive structures, was exhibited in the end range in standing but in the semi-flexed and slump sitting postures [15]. As a result, semi-flexed and slumped sitting for a sustained period not only leads to relaxation of the spinal-stabilizing muscles and reduced muscular support of the spine but also impairs motor coordination and control, thus promoting LBP [15, 16, 17].
Another controversial point about the relationship between sitting posture and LBP is that lordosis is dynamic and its profile changes during daily posture adjustment movements [1, 2, 18, 19]. Therefore, because the acceptable range of lumbar lordosis is relatively wide, it is necessary to classify it within the normal range to identify patterns of sagittal alignment and functional movements [20]. Some previous studies have suggested that regional lumbar lordosis (RLL), including the upper (ULx) and lower (LLx) lumbar lordosis angles, should be considered when assessing spinal posture [21, 22, 23]. Larger proportions of the LLx spine from usual sitting to slumped sitting [21] and of each of the five lumbar segments contribute to lordosis, with the L5 segment contributing almost 40% to overall lordosis, whereas the L1 segment contributes only 5% [22]. To accurately quantify the effects of slumped sitting, it is necessary to consider changes in both global lumbar lordosis (GLL) and RLL angles (ULx and LLx, respectively). Furthermore, Scannell and McGill [3] examined passive tissue stiffness and lumbar position during sitting, standing, and walking, and reported that subjects with hypo-lordosis exhibited more passive tissue strain during sitting than subjects with hyper-lordosis; hyper-lordotic subjects also showed greater spinal extension during standing than the control and hypo-lordosis subjects. Thus, the lordosis angle during standing can affect the lordosis angle and spinal range of motion during sitting [20, 24, 25]. Thus, to quantify the effects of sitting posture and range of movement, it is necessary to divide subjects into groups according to their lordosis angle during standing. Although slumped posture is associated with low back problems and impaired movement patterns, quantitative evidence is lacking. Therefore, the main purpose of this study was to investigate differences in GLL and RLL during slumped sitting among groups classified according to standing lordosis angle. A secondary goal was to investigate the correlation between GLL and RLL during upright and slumped sitting postures.
Methods
Subjects
A total of 48 young healthy subjects (16 males, 32 females) were recruited at Inje University in Gimhae, South Korea, from March to April 2018. No subject had any history of musculoskeletal pathology, surgery or traumatic injury during the previous 12 months. Furthermore, no subjects exhibited any functional restriction or respiratory or neurological disorder, and none reported any pain elsewhere in the spine or lower limbs. Based on the standing measurement, the participants were categorized into the three groups: flat-back (T10–S2
Measurement system
We used three wireless inertial measurement units (IMUs) to measure GLL and RLL. The IMUs each consisted of three transmitters (EBIMU24G; E2BOX, Seoul, South Korea), one receiver (39 mm
Data analysis
The T10, L3, and S2 sagittal angles [26] were acquired during the sitting, slumped sitting, and standing postures using Visual FoxPro in Eulerian coordinates (roll-pitch-yaw angles). All angles are reported as the mean of three 5-second measurements. Based on the standing measurement, the participants were categorized into the three groups: flat-back (T10–S2
Procedures
Prior to performing the task, the participants were asked to stand in a comfortable posture with the feet slightly apart, looking straight ahead. The examiner attached three transmitters mounted on a plastic frame to the T10, L3, and S2 spinous processes [26] using Transpore medical tape (3M, Seoul, South Korea) (Fig. 1). We then conducted measurements in triplicate (5 s each) while the participants were in a standing posture. Following the measurements, the participants were categorized into the three GLL groups. Then, the participants were asked to sit on a table with a comfortable upright posture, with the feet not reaching the floor; measurements were again conducted in triplicate (5 s each). Finally, the participants were asked to sit in a slumped posture with a posterior pelvic tilt, and the same measurements were again acquired. To ensure accurate task performance, verbal feedback was provided for all three postures [4]. For example, keep your pelvis slight anteriorly to keep your back slight lordosis natural (Fig. 1b) and rotate your pelvis backwards and maintain a bent position while looking straight ahead (Fig. 1c).
Experimental condition. a) Placement of the 3 transmitters on the T10, L3, and S2 spinous processes. b) upright sitting side view. c) slump sitting side view.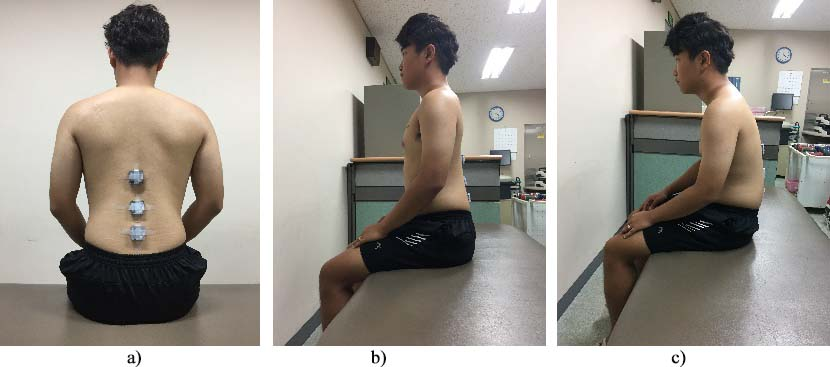
We used the SPSS statistical package (version 18.0 for Windows; IBM Corp., Armonk, NY, USA) to detect differences among the three groups via one-way analysis of variance (ANOVA). All data were tested for normality using the Kolmogorov-Smirnov test, and for homogeneity of variance using Levene’s test. Tukey correction was applied for multiple comparisons. When equal variance was not observed, the Tamhane correction was used. Correlation coefficients (
General characteristics of the participants (
48)
General characteristics of the participants (
All values are mean
A total of 48 asymptomatic young subjects (16 males, 32 females) were categorized into the three groups delineated above. Descriptive statistics for the GLL angle in each group are summarized in Table 1. The T10, L3, and S2 measurements were all repeated three times to evaluate the reliability of the test; the intraclass correlation coefficients (ICCs) and standard errors of measurement are presented in Table 2 for T10, L3, and S2.
Reliability indices for IMU data during standing and sitting (
48)
Reliability indices for IMU data during standing and sitting (
The GLL (T10 to S2) during upright sitting and slumped sitting, and the range of motion during the transition between these postures, all differed significantly among the groups (
Comparison of global and regional trunk angles in slump sitting posture among the standing global lumbar lordosis group (
48)
Comparison of global and regional trunk angles in slump sitting posture among the standing global lumbar lordosis group (
All values are mean
The correlation among the global and regional lumbar lordosis angles in upright and slump sitting posture among the standing global lumbar lordosis group
Global, T10 relative S2 angle; Upper lumbar lordosis, T10 relative L3; Lower lumbar lordosis, L3 relative S2.
Comparison of global angles in slump sitting posture among the standing global lumbar lordosis group.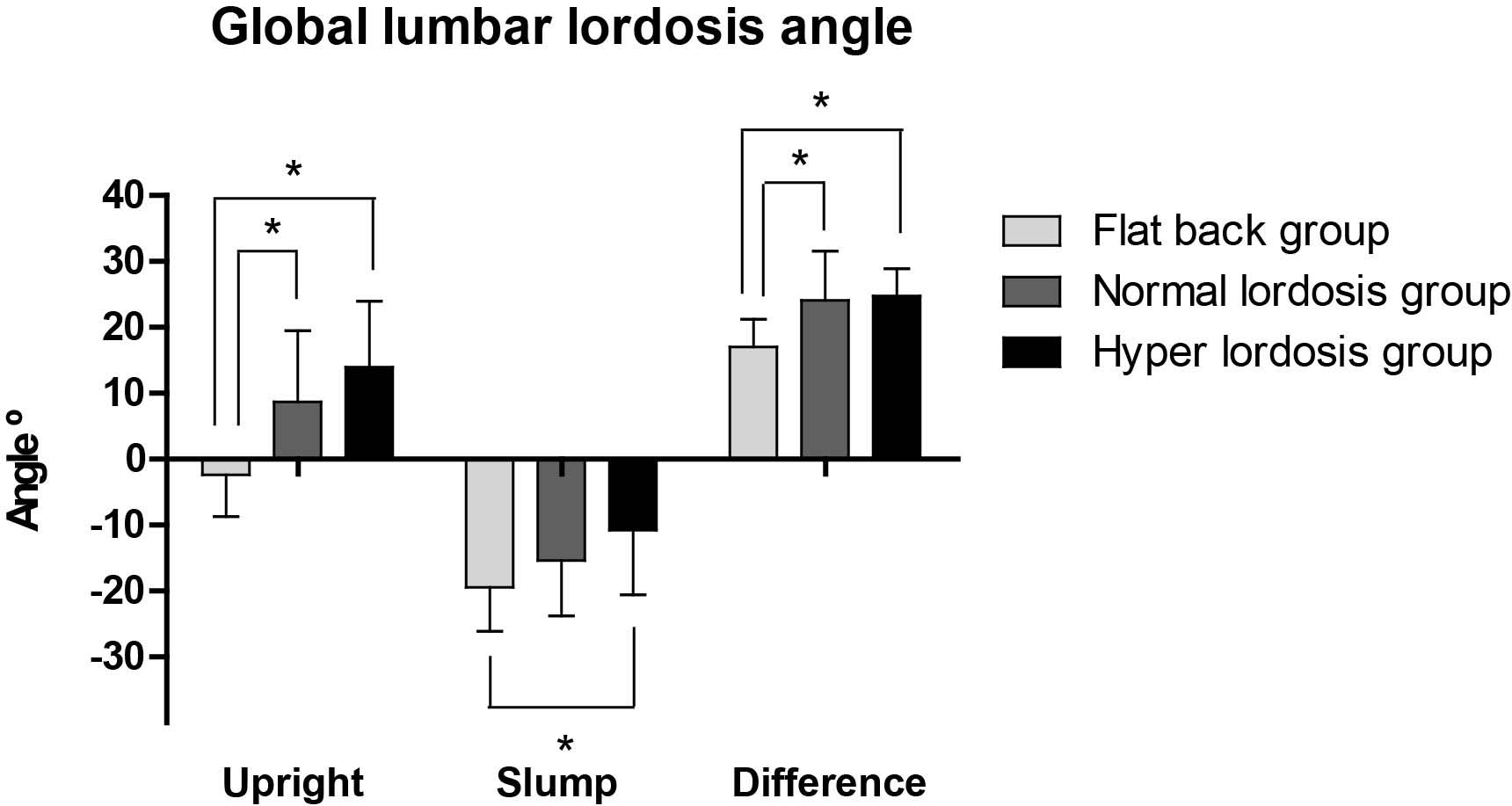
Comparison of upper lumbar lordosis angles in upright and slump sitting postures among the standing global lumbar lordosis groups.
In the flat-back group, the ULx during upright sitting (T10 to L3, 2.43
In the flat-back group, the LLx angle during upright sitting (L3 to S2,
Comparison of lower lumbar lordosis angles in upright and slump sitting postures among the standing global lumbar lordosis group.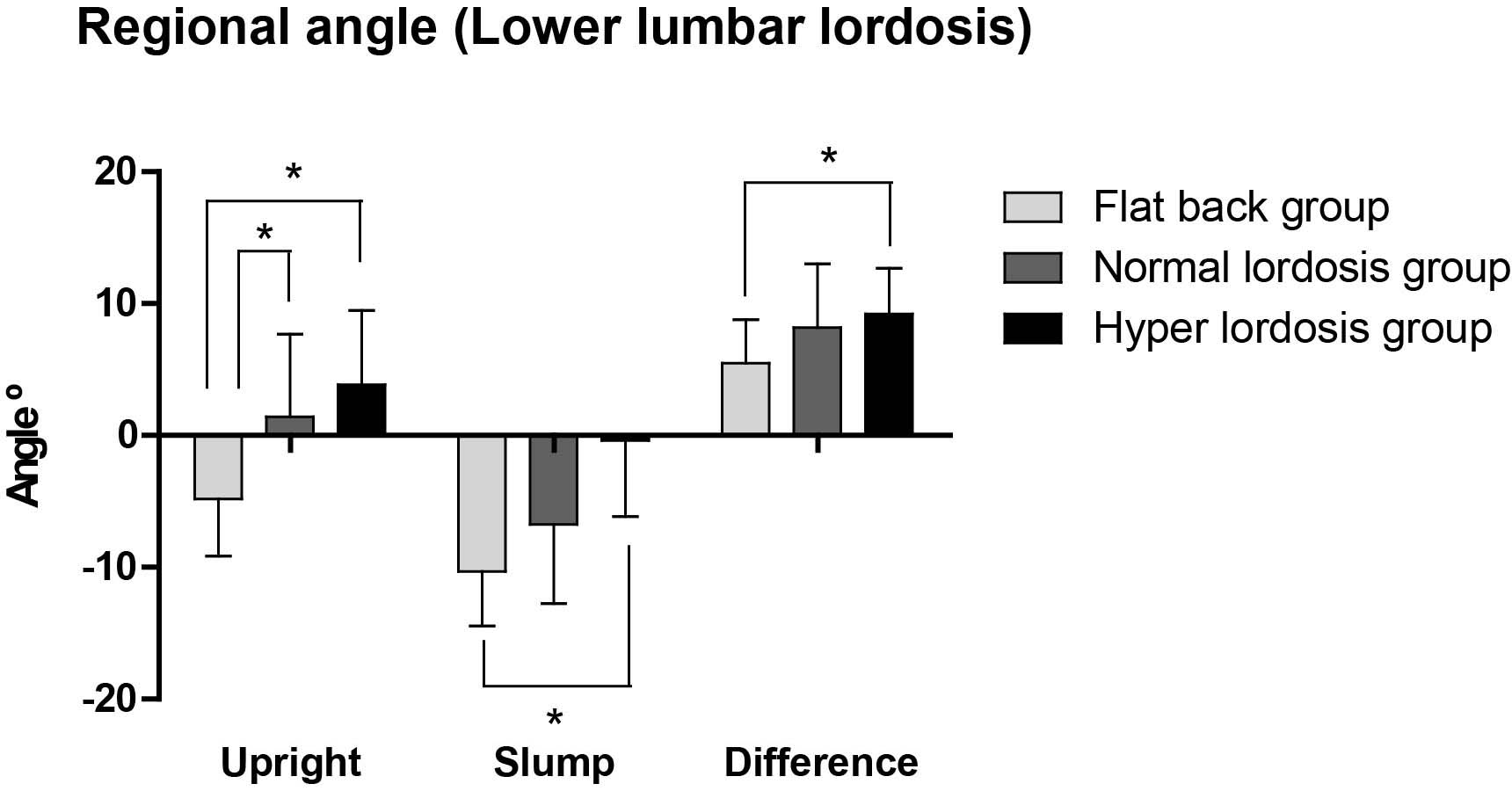
The correlation of global lumbar lordosis angle between standing and sitting a) upright sitting b) slumped sitting.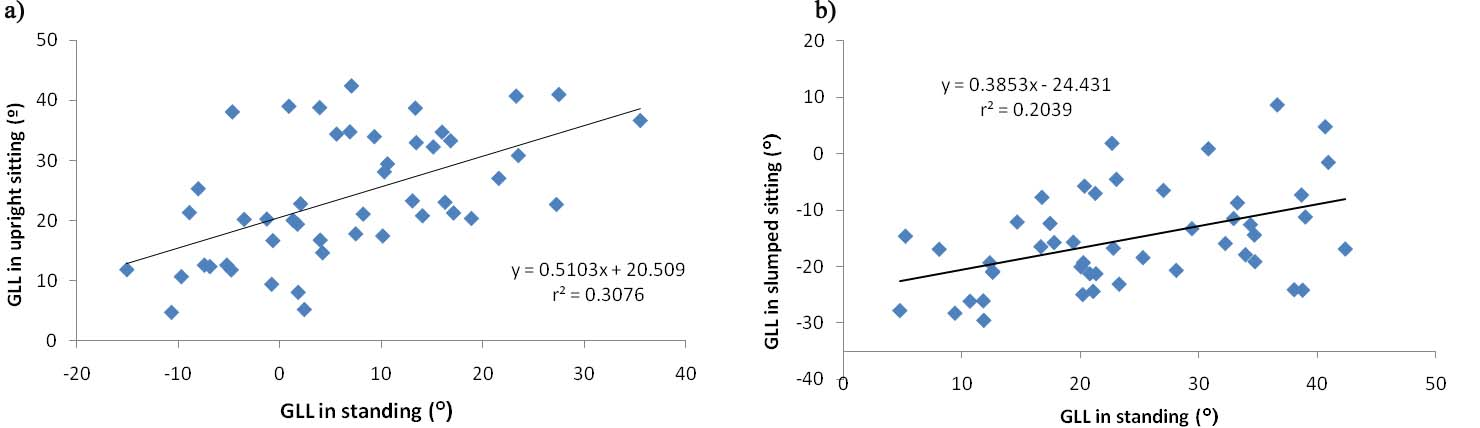
The correlation between global and regional lumbar lordosis angle. a) upright sitting b) slumped sitting.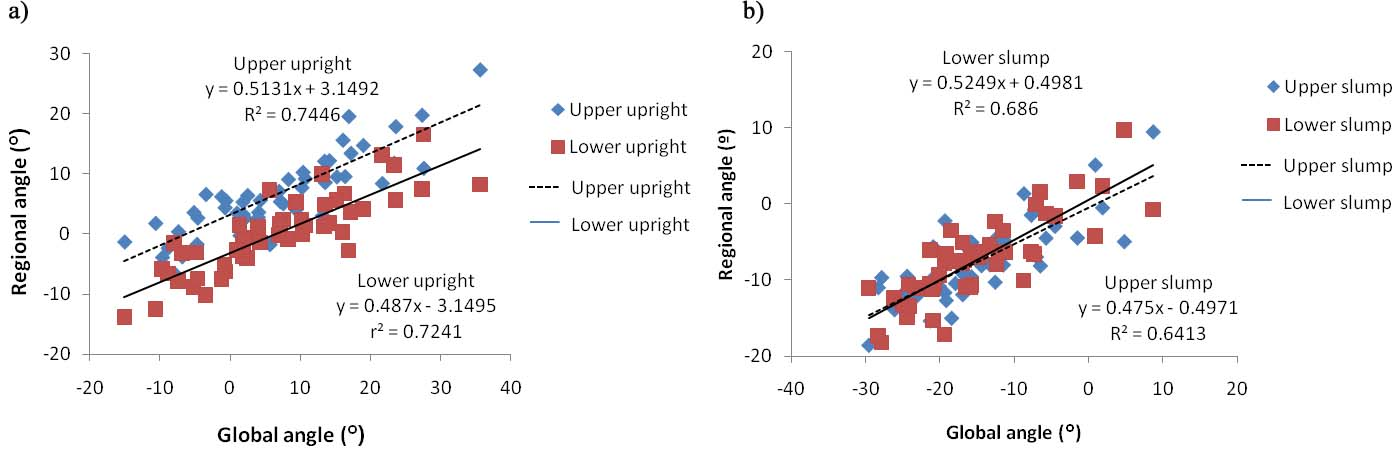
Descriptive statistics for the regression variables of GLL in standing, GLL, and RLL, during upright and slumped sitting, are shown in Table 4. The GLL in standing showed a significant and moderate correlation with the GLL (
In this study, we examined differences in GLL and RLL during upright and slumped sitting among groups classified according to standing lordosis angle, and the correlation between GLL and RLL angles during upright and slumped sitting postures. Our primary findings are that both GLL and RLL in the flat-back group reduced lumbar lordosis in the upright sitting posture and increased lumbar kyphosis in the slumped sitting postures (i.e., close to the end range of lumbar flexion), but the range of motion during the transition from upright sitting to slumped sitting was lower than that in the normal and hyper-lordosis groups.
The flat-back posture is characterized by a reduced lumbosacral and lumbar lordotic curve and posterior tilt of the pelvis. The lack of a normal physiological lumbar curve reduces the shock-absorbing effect of the lumbar region and serves as a predisposing factor for injury. In contrast, the hyper-lordotic posture is characterized by an increased lumbosacral and lumbar lordotic curve and anterior tilt of the pelvis [28]. Excessive lumbar lordosis may be a risk factor for LBP during prolonged periods of standing [29], whereas during sitting, lumbar lordosis is generally reduced by the influence of hip flexion compared to the standing posture [3, 30, 31]. In this study, the flat-back posture group showed reduced lumbar lordosis and increased lumbar kyphosis during upright sitting and slumped sitting compared to the normal and hyper-lordosis groups. Mitchell et al. [21] analyzed differences between ULx (T12 relative to L3) and LLx (L3 relative to S2) in habitual lumbar spine posture and movement in individuals with and without LBP; they reported average ULx values for a lordosis position of
Our results also demonstrated that, when moving from upright to slumped sitting, the range of motion was lower in the flat-back group than in the normal and hyper-lordosis groups. One possible reason for this could be differences in pelvis position; the flat-back group already exhibited a posterior pelvic tilt during upright sitting, such that the range of motion of the LLx required to achieve slumped sitting was smaller than in the other groups.
The current study included healthy subjects, so it is difficult to compare the results with those of studies on patients with LBP. However, previous studies that classified LBP patients into flexion and extension groups showed results similar to those of our study. Dankaerts et al. [5] reported that during slumped sitting, patients with extension-related LBP demonstrated less end-range lumbar flexion than those with flexion-related LBP and healthy controls. Thus, flexion during sitting causes more stress in those with a flat-back posture than in normal and hyper-lordotic individuals. Also, in the flat-back posture, shorter hamstrings can cause increased posterior pelvic tilt when moving from upright to slumped sitting. Even though this study did not measure hamstring length, hypo-lordosis generally leads to reduced hamstring flexibility, which could limit pelvic motion during slumped sitting, thereby reducing the LLx range of motion. Frey et al. [14] demonstrated that during the sit-and-reach test, individuals with greater anterior pelvic tilt scored higher than those with less marked anterior pelvic tilt; moreover, hamstring flexibility influenced the pelvic angle during sitting. Accordingly, the range of motion during the transition from upright sitting to slumped sitting in our flat-back group was smaller than that of the other groups.
Furthermore, our linear regression analysis of GLL in standing position revealed that 31% of the variance was explained by the GLL and LLx angles during upright sitting. Our results also indicated that the GLL angle adopted during standing was affected more by the GLL and LLx angles than by the ULx angle during upright sitting. This finding is supported by Dunk et al. [32], who suggested that the majority of flexion during sitting occurs at the L5/S1 joint, principally due to rotation of the pelvis via the hips. Our flat-back group also tended to have a more flexed trunk position during both upright and slumped sitting than the other groups. This result suggests that the flat-back posture is a potential source of LBP, because increased flexion increases intradiscal pressure and transfers load to the passive tissues [28, 30]. These results are consistent with those of Scannell and McGill [3], who reported that during sitting over a given period of time, individuals with hypo-lordotic lumbar posture sat farther from their neutral zones than those with hyper-lordotic lumbar posture; their subjects with a hypo-lordotic curve had increased posterior tissue tension. Thus, individuals with a flat-back posture may need to change position frequently during sitting to minimize tissue strain and achieve an even distribution of load throughout the spine, to prevent potential injury [33].
In this study, the GLL angle during upright sitting explained 74% of the ULx and 72% of the LLx angles, and the GLL angle during slumped sitting explained 64% of the ULx and 69% of LLx angles. The ULx and LLx angles in upright and slumped sitting could explain only 22% and 11% of the ULx and LLx angles, respectively. Our findings indicated that the GLL angle is correlated with the ULx and LLx angle in both the upright and slumped sitting postures, while there was a weaker correlation between the ULx and LLx angles during upright and slumped sitting. These findings are partially supported by Mitchell’s study [21] with respect to regional differences in lumbar spine kinematics. They investigated regional differences within the lumbar spine (i.e., in the LLx and ULx) during static postures and functional tasks and reported that, when transitioning from an upright to slumped sitting position, the largest change occurred in the ULx, which showed a moderate positive correlation with the LLx. However, the LLx did not correlate with the ULx during static upright and slumped sitting postures. Furthermore, they concluded that GLL kinematics do not reflect regional lumbar spine kinematics. However, our findings indicated that GLL explains the ULx and LLx angle
Our study had some limitations that should be addressed. First, our participants were all asymptomatic, healthy young subjects, and the range of lumbar lordosis angles among the subjects was narrower than the clinically accepted normal range. In addition, the correlation analysis sample size was too small. Thus, our findings cannot be generalized to the entire population, or to those with LBP or postures such as sway-back. Second, we did not consider overall trunk flexion, thoracic angle, or hip motion and flexibility. Future studies should include measures of total spinal motion during slumped sitting and forward bending in subjects with flat-back and hyper-lordosis postures.
Conclusions
In the present study, we measured changes in global and regional lumbar angles during slumped and upright sitting in three groups classified according to the GLL angle in standing. The flat-back group posture is a potential source of low back pain during both upright and slumped sitting than the normal and hyper-lordosis groups. Posture measurements in a standing and sitting position conducted to assess lordosis should consider the relationship between GLL and RLL. Our findings may help healthcare professionals to manage and interpret spinal posture in younger people.
Footnotes
Acknowledgments
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (Nos 2020R1F1A104919111 and 2019R1A6A3A0109638 412).
Conflict of interest
None to report.