
Abstract
BACKGROUND:
Musculoskeletal disorders in acromegaly compromise upper and lower limb activity. Corresponding changes can be better assessed by a functional capacity test incorporating multitasking, such as the Glittre Activities of Daily Living Test (GA-T).
OBJECTIVES:
To evaluate functional capacity in adults with acromegaly using the GA-T and to correlate functional capacity with hand function and health-related quality of life.
METHODS:
The GA-T was applied to 36 patients with acromegaly and an equal number of healthy individuals. Additionally, participants completed the Acromegaly Quality of Life (AcroQoL) questionnaire and underwent a chronic pain assessment using a map of the human body, a hand function evaluation using the Cochin Hand Functional Scale (CHFS), and a handgrip strength test.
RESULTS:
Relative to the comparison group, patients with acromegaly required more time to perform the GA-T, showed worse hand function, and reported that squatting to accomplish shelving tasks was the major difficulty. GA-T time was correlated with the AcroQoL global score, handgrip strength, and the CHFS (
CONCLUSIONS:
Patients with acromegaly exhibited a reduced functional capacity as assessed by the GA-T. Additionally, an association was identified between the total GA-T time and both hand function and quality of life.
Introduction
Acromegaly is a chronic and disabling disease, with prevalence and incidence rates varying from 2.8 to 13.7 and 0.2 to 1.1 cases per 100,000 people, respectively [1, 2]. Most cases are caused by growth hormone (GH)-secreting pituitary adenomas [3, 4]. Excess GH/insulin-like growth factor 1 (IGF-1) causes a set of clinical manifestations and increased morbidity and mortality, which may result in reduced physical function. Despite major efforts in recent decades, little has been achieved regarding the delayed diagnosis of acromegaly, which increases the number of disease-related complications at the time of diagnosis [5]. Furthermore, although reversing excess GH improves clinical complaints and life expectancy, several acromegalic traits persist due to irreversible changes, especially those involving bones and joints, which may negatively impact the functional capacity of these individuals [6, 7].
Arthropathy is a common complication of acromegaly and is present in approximately 75% of cases [8]. The main symptom is joint pain, but stiffness, hypomobility and functional limitations are also common [7]. In addition, the joint impairment caused by excess GH does not seem to completely regress after hormonal normalization, such that therapies are often unable to restore joint function to its previous state [9]. Although acromegalic arthropathy shares features with primary osteoarthritis (OA), the joint spaces are often widened rather than narrowed in patients with long-term control [10]. OA affects both the spine and large and peripheral joints, and involvement of the latter is almost always symmetrical [10].
In addition to several metabolic disorders, excessive GH causes the proliferation of many structures, including connective tissue, cartilage, bones, and muscles, causing musculoskeletal disorders and acral overgrowth. In the hands, there is soft tissue hypertrophy, excessive bone and cartilage growth, and deformity emergence. In addition, carpal tunnel syndrome and swelling of the hands and fingers can lead to nerve compression and reduced muscle strength [11, 12, 13]. In patients with acromegaly, in fact, musculoskeletal disorders are responsible for the main functional disability of the hands [14]. Although there is significant soft tissue growth in the hands of patients with acromegaly [14], even after long-term remission, little is known about the functional repercussion of these abnormalities. Moreover, the clinical and radiographic courses of acromegalic arthropathy, including those involving the hands, are not related and thus require further studies [7].
Clinical disorders involved in acromegaly make it a disease with a considerable impact on health-related quality of life (HRQoL), which is currently considered an important outcome in chronic disease treatment [9]. Although joint problems do not reduce the life expectancy of patients with acromegaly, they are associated with considerable impairment in physical functioning and psychological well-being, reducing HRQoL [9]. Interestingly, when investigating the impact of various dysfunctions on the HRQoL of patients, there is a significant influence on daily and habitual activities and in those that affect overall health [15]. With successful therapy, there is only partial improvement in HRQoL in patients with acromegaly, and moreover, the relationship between GH-IGF-1 levels and the subjective perception of HRQoL is not good [16].
In patients with acromegaly, several complications can cause exercise intolerance, including musculoskeletal disease, metabolic disorders, acromegalic cardiomyopathy and respiratory dysfunction [15]. Considering that most activities of daily living (ADLs) are performed at submaximal effort levels, submaximal tests can reliably reflect the level of functionality of an individual. Among the available tests to measure the functional capacity of patients with systemic diseases, one of the best-tolerated tests with good reproducibility used in patients with acromegaly is the 6-minute walk test (6MWT) [17]. However, because it is a walking activity only, the 6MWT does not assess limitations in activities performed with the upper limbs, which are usually highly involved in typical ADLs [18].
The sum of the various disorders present in patients with acromegaly reduces their functional capacity and consequently strongly compromises HRQoL, which justifies the continuous search for assessment methods that encompass the functional evaluation of this population. However, to the best of our knowledge, no previous study has addressed mobility in ADLs in patients with acromegaly. In this context, the Glittre ADL-test (GA-T) was created to evaluate the functional status of individuals using multiple tasks that require upper and lower limb muscle activity [18]. These tasks are similar to ADLs, such as walking, getting up from a chair, stair climbing/descending, crouching, kneeling, carrying, and lifting objects. In addition to being an easily administered and reliable test, the GA-T assesses exercise functional capacity by simulating daily activities in a field test, thus better reflecting real-life situations [19, 20]. Because patients with acromegaly have important functional limitations involving upper and lower limb movements, the GA-T may be an interesting tool because it standardizes the use of activities involving multiple ADLs. This test has been established as an innovative instrument for the evaluation of patients with various cardiac and pulmonary conditions [19, 20, 21, 22, 23]. We hypothesized that individuals with acromegaly experience many difficulties in completing the multiple tasks of the GA-T and that poor performance during the test is related to worsening of manual function and quality of life. Thus, the objectives of the present study are to assess functional capacity in adults with acromegaly using the GA-T and to correlate functional capacity with hand function and HRQoL in this population.
Material and methods
Participants
Between March and September 2019, a cross-sectional study was conducted with 45 patients with acromegaly aged
Instruments and measurements
Acromegaly Quality of Life questionnaire
The Acromegaly Quality of Life (AcroQoL) questionnaire was used to evaluate HRQoL. This is an acromegaly-specific questionnaire that assesses the specific dimensions affected by the condition [25]. There are 22 items divided into 2 scales: 1 that assesses physical characteristics (8 items) and 1 that assess psychological aspects (14 items). The AcroQoL scores range from 22 to 110 points, and a higher score is associated with a better HRQoL. In addition to the AcroQoL, patients were asked to report the presence of chronic pain (longer than 3 months) and to locate their major chronic pain on a map of the human body; this evaluation criterion has been widely used to evaluate patients with pain [26, 27].
Cochin Hand Functional Scale
The Cochin Hand Functional Scale (CHFS) was used to assess the level of hand ability and functionality in the performance of daily activities [28, 29]. The CHFS contains 18 items concerning ADLs that require manual skills, such as cooking, dressing, and personal hygiene. This scale requires approximately 3 minutes to complete and considers only the experiences of the individual during the past month. Each item has 6 possible answers, as follows: without difficulty (0); with very little difficulty (1); with some difficulty (2); with much difficulty (3); nearly impossible to do (4); and impossible to do (5). The score is the sum of all items and ranges from 0 to 90; the higher the score is, the greater the hand dysfunction [28, 29].
Isometric handgrip strength
Isometric handgrip strength (IHGS) was measured using a hydraulic isometric dynamometer (SH5001, Saehan Corporation, Korea) with the hand on the dominant side of the body. Participants were comfortably seated in a chair with no arm rest, with the feet flat on the floor and hips and knees flexed at 90
Schematic representation of the Glittre ADL-test. The test consisted of carrying a backpack containing a 2.5-kg weight for women and a 5-kg weight for men while completing a circuit with the following activities. The participant rose from a seated position and walked on a 10-m flat course interposed halfway by a stairway with 2 steps to ascend and 2 to descend. After completing the course, the individual approached a 2-tier shelf containing 3 objects weighing 1 kg each placed on the highest shelf (shoulder height) that had to be moved 1 by 1 to the bottom shelf (waist height) and then down to the floor. Then, the objects were placed on the bottom shelf again and finally on the top shelf. Then, the individual turned and walked back over the course; immediately after completing 1 lap, another lap was started to complete the same circuit. The participant had to complete 5 laps in the shortest possible time.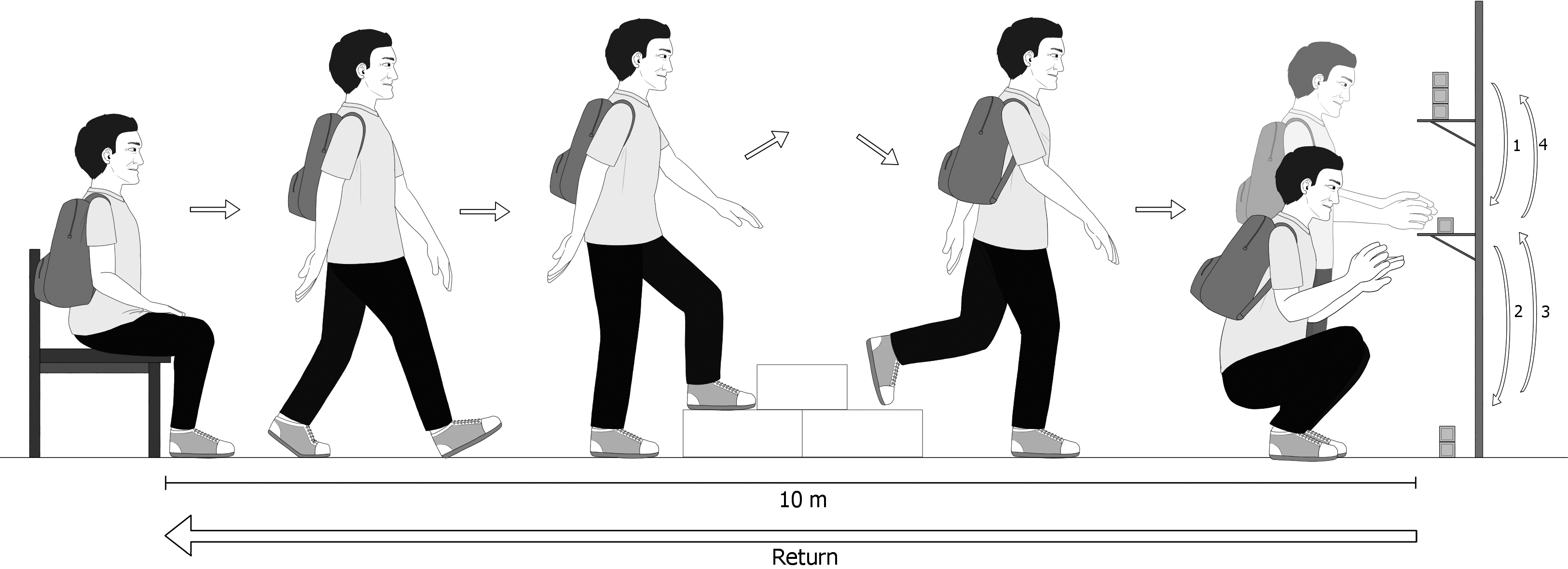
The GA-T (Fig. 1) was performed as proposed by Skumlien et al. [18], with the participant having to complete 5 laps in the shortest possible time. The instructions were standardized, and there was no incentive during the test. Two tests were performed with a minimum interval of 30 minutes of rest to avoid learning and training effects, and the GA-T with the shortest time spent performing ADLs was used for analysis [31, 32, 33].
Statistical analysis
Nonparametric methods were applied because no variables presented a normal distribution (Gaussian) according to rejection of the normality hypothesis by the Shapiro-Wilk test in at least 1 of the 2 groups (acromegaly group or comparison group). The results are expressed as median values and interquartile ranges or as frequencies (percentages). The acromegaly group and the comparison group were compared using the Mann-Whitney test for numerical variables and the chi-square test or Fisher’s exact test for categorical variables. The association between the GA-T total time and the numerical variables was analyzed by the Spearman correlation coefficient (
To provide context for interpreting the null findings, a post hoc power analysis was performed using GPower 3.1.1 software based on the actual sample size (
Demographic characteristics, clinical data, hand function, handgrip strength, quality of life, and Glittre ADL-test results of the acromegaly and comparison groups
Demographic characteristics, clinical data, hand function, handgrip strength, quality of life, and Glittre ADL-test results of the acromegaly and comparison groups
The values shown are the median (interquartile range) or number (%). Bold type indicates significant differences. List of abbreviations: BMI: body mass index, AcroQoL: Acromegaly Quality of Life questionnaire, CHFS: Cochin Hand Functional Scale, IHGS: isometric handgrip strength, SpO
Bland-Altman plot for the total time between the two tests (T1 and T2).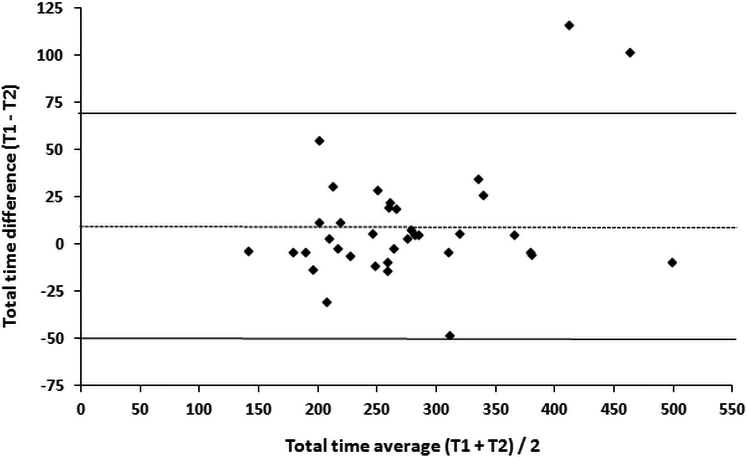
Relationships of total time with the global score of the Acromegaly Quality of Life questionnaire (AcroQoL) (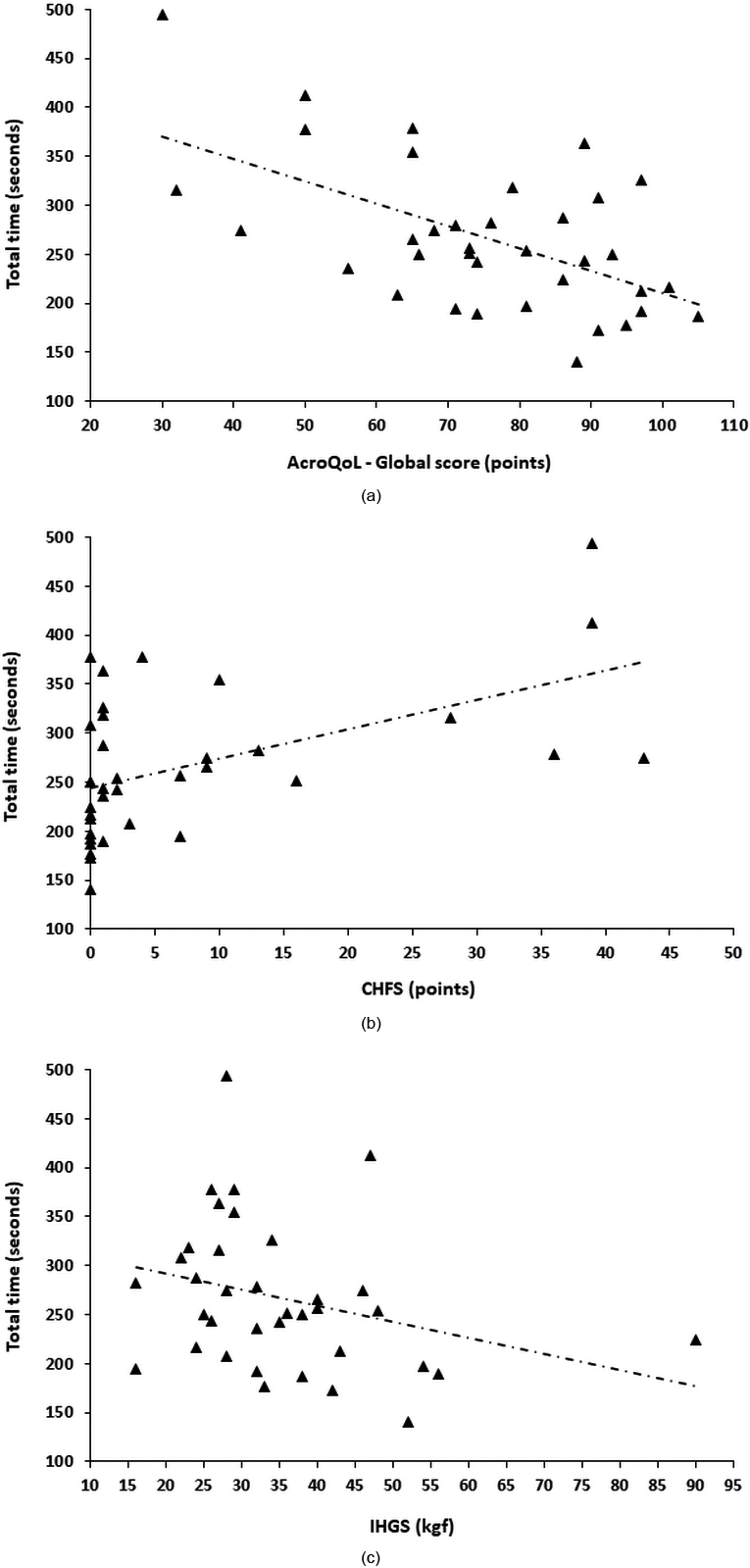
Among the 45 patients who were evaluated for inclusion in the study, 9 were excluded for the following reasons: refusal to participate in the study (
Regarding the GA-T, we observed a significant difference between the patient group and the comparison group in the total time required to complete the test [253 (209–314) seconds vs. 184 (139–207) seconds, respectively,
When comparing the medians of the 2 GA-T trials performed by the patients, no significant difference was noted, although the time to complete the second trial was shorter [268 (224–319) seconds vs. 260 (214–318) seconds,
We also evaluated the associations between the GA-T total time and the other variables studied in patients with acromegaly. In this analysis, the total GA-T time correlated negatively with the AcroQoL global score (
Spearman’s correlation coefficients for Glittre ADL-test results, clinical data, quality of life, hand function, and handgrip strength
Spearman’s correlation coefficients for Glittre ADL-test results, clinical data, quality of life, hand function, and handgrip strength
Bold type indicates significant differences. List of abbreviations: AcroQoL: Acromegaly Quality of Life questionnaire, CHFS: Cochin Hand Functional Scale, IHGS: isometric handgrip strength.
Comparison between Glittre ADL-test time, major chronic pain, and the highest difficulty reported at the end of the test
The values shown are the median (interquartile range) or number (%). Bold type indicates significant differences.
Finally, we evaluated whether the demographic, clinical, and functional variables could independently predict performance during the multiple GA-T tasks (Table 4). In the stepwise forward regression analysis, age (
Forward stepwise regression model for Glittre ADL-test time using demographic, clinical, and functional data
List of abbreviations: B: regression coefficient, SEB: standard error of the regression coefficient, R: correlation coefficient, R
The present study shows several interesting findings that should be highlighted. First, patients with acromegaly required more time to perform the multiple tasks of the GA-T and had worse hand function while performing ADLs than individuals in the comparison group, indicating that the functional limitations of patients with acromegaly negatively affect daily activities. Second, GA-T time was associated with both hand function and HRQoL in patients with acromegaly, reflecting the essential role of routine evaluation of these components in clinical practice. Third, in contrast to most individuals in the comparison group who had no difficulty performing the GA-T tasks, the patients with acromegaly reported that squatting was the most difficult ADL to perform in the GA-T, possibly because squatting requires hip strength and knee strength, which are impaired in patients with acromegaly. Fourth, the various GA-T task difficulties reported by the patients at the end of the test differentially affected the total time needed to complete the test, suggesting that acromegalic arthropathy affects patients differently due to varying joint involvement. Fifth, the major chronic pain reported by patients with acromegaly before the GA-T was mainly located in the lower limbs and was associated with GA-T time. Thus, chronic pain in the lower limbs may have impaired squatting and therefore the patients’ performance in completing the shelving tasks during the GA-T. Finally, we observed that age and CHFS score were the only factors that explained the GA-T time, emphasizing that aging and worsening hand function strongly impact performance during the test.
The functional capacity to perform ADLs is best predicted by global tests that replicate daily activities than by tests focused on isolated components of functional activity; thus, it has been recently suggested that tests involving at least 3 different tasks be used to evaluate ADLs [34, 35]. In the present study, compared with the individuals in the comparison group, the patients with acromegaly required more time to perform the GA-T, with a median time of 253 seconds (or 4.22 minutes), which is substantially longer than the time described for healthy Brazilian adults for whom the mean time to complete the GA-T was 2.84
In our study, patients with acromegaly reported squatting to accomplish the shelving tasks to be the activity causing the greatest difficulty in the GA-T, although other complaints reported at the end of the test (including the stair tasks and the manual tasks) differentially impacted the total test time. Squatting is a notoriously complex exercise, in terms of both biomechanics and neuromuscular demands. In the squatting exercise, several conditions can influence muscle activity, including knee angle, foot width, rotation of the lower limbs and center of gravity [38, 39]. In addition, muscle activation of the lower extremities can change based on knee alignment during execution of the exercise and influence squatting and ascending/descending stairs [38, 39]. In patients with acromegaly, the major limiting factor of functional capacity has been attributed to arthropathy, which can involve the spine, knees and hips and negatively impact the squatting and stair tasks in the GA-T [9, 37]. The pathogenesis of acromegalic arthropathy involves, in the initial phase, excess GH-IGF-1 with stimulation of osteophytes and hypertrophy of cartilage and, in the advanced phase, repeated intra-articular trauma and exaggerated repair reactions resulting in irreversible degenerative arthrosis and worsened articular geometry [7, 9, 40]. Notably, the main site of chronic pain in our sample was the lower limbs-reported by almost 40% of patients- and this may have negatively impacted squatting and, consequently, performance on the GA-T. Interestingly, Guedes da Silva et al. [15] observed that the distance walked during the 6MWT by patients with acromegaly was not significantly different from that walked by individuals in the comparison group. Thus, we believe that the differences in the performance of patients with acromegaly between the GA-T and the 6MWT may be due to the incorporation of multitasks imposed by the GA-T, including squatting.
A number of changes occur in the hands of patients with acromegaly, including excessive acral growth, arthrosis, widened joint spaces, and cartilage hypertrophy, which together may culminate in joint pain, hypomobility and functional limitations [7, 9, 10, 14]. Compared to the individuals in the comparison group, we observed that the patients with acromegaly had worse hand function evaluated by the CHFS, which is a self-administered scale that is easy to apply and has been used to measure hand impairment in various clinical conditions [41, 42]. Importantly, we also observed an association between the CHFS and the GA-T total time, suggesting that the symptoms related to the joints of the hands and impaired movement may affect ADLs and negatively impact performance during the GA-T. Because acromegaly results in impairment of the hands and because these changes can potentially affect the performance of ADLs to varying degrees, we believe that the assessment of hand function and its effect on functional capacity in patients with acromegaly may be of interest in routine clinical practice. This could enable early counseling and the early initiation of physical therapy in patients already presenting with impaired hand function.
Because it is a low-cost and quickly applied measure, isometric dynamometry for the assessment of IHGS has been used to estimate total body strength in different groups of individuals [43]. Similar to the study by Walchan et al. [12] and Homem et al. [13], our study showed a reduction in IHGS in patients with acromegaly compared to individuals in the comparison group. In acromegaly, several factors contribute to peripheral muscle weakness, including the direct effect of GH on muscles, acromegalic arthropathy, and metabolic disorders associated with the disease, such as hypothyroidism, hypoadrenalism, and diabetes [15]. In these patients, there is also hypertrophy of type I fibers and atrophy of type II fibers, generating significant functional changes with a reduction in muscle strength and endurance [15]. These abnormalities also explain, at least in part, the association between IHGS and the GA-T total time because some of the ADLs incorporated into the GA-T depend on hand muscle strength.
In addition to controlling excess GH, treating associated comorbidities and reducing mortality, addressing HRQoL is increasingly becoming an objective in the management of acromegaly as therapeutic options improve [3]. In the present study, we observed significant correlations between the different AcroQoL dimensions (global score, physical function, and psychological function) and GA-T total time, suggesting that both physical characteristics and psychological aspects influence patient performance during the GA-T. In fact, factors such as disease activity, pain, reduced joint mobility, depression, and emotional imbalance can strongly impact the overall state of patients with acromegaly, cause major restrictions in ADLs, and significantly influence the perception of HRQoL when evaluated using questionnaires, such as the AcroQoL [44, 45]. Using the 6MWT in patients with acromegaly, Guedes da Silva et al. [15] found a significant correlation between the AcroQoL global score and the main outcome of the 6MWT, which is the distance walked (
The GA-T was initially developed and validated for patients with COPD, although it has been recently evaluated in several clinical conditions, including cardiovascular disease, community-acquired pneumonia, cystic fibrosis and the postoperative period of bariatric surgery [22, 23, 46, 47]. However, there are still no tests available in clinical practice that simultaneously incorporate ADLs performed with the upper and lower limbs of patients with acromegaly, and therefore, we evaluated the importance of the GA-T in this population. Because all patients with acromegaly performed the test in duplicate, we found a high ICC between the measurements of the 2 GA-T trials, indicating that the GA-T total time was quantitatively reproduced the 2 different times it was performed. However, the median total time in the second test was slightly lower, which indicates a possible learning effect. Despite the encouraging results, further studies should determine whether modifications to the GA-T are necessary to fit the typical phenotype of patients with acromegaly and to provide data on its validity, reliability, and responsiveness. In addition, GA-T performance in patients with acromegaly needs to be evaluated in regard to important outcomes, such as response to hormone therapy, functional rehabilitation, and survival.
Finally, we built an explanatory model for the total GA-T time. In this model, age and the CHFS score explained 48% of the total GA-T time variability, indicating that the abnormalities in the hand joints of acromegalic individuals are an important contributor to poor performance during the GA-T. Unsurprisingly, age entered our explanatory model. Using a sample of healthy individuals, recently published reference equations for the GA-T showed that age was the strongest predictor of the total GA-T time [32]. Aging diminishes muscle strength and endurance, which are important components of functional capacity [48]. With the aging process, progressive physical deterioration can be even more affected in patients with acromegaly.
The strength of our study is that it is the first to evaluate the GA-T in a population of patients with acromegaly, which revealed that these patients need more time to perform the multiple tasks of the GA-T compared to healthy individuals, possibly due to limitations in both the lower and upper limbs. However, as with any study, ours also has limitations. First, the sample size was relatively small, and the study did not longitudinally evaluate possible changes in the GA-T in patients with acromegaly. Second, the energy expenditure and the physical activity level of patients were not evaluated with activity monitors, and these measures could help us explain some of our findings. Despite these limitations, the GA-T seems to be a potential test to be used in laboratories and clinical practice to evaluate the performance of ADLs in individuals with acromegaly.
Conclusion
This study found that patients with acromegaly showed a reduced functional capacity as assessed through the multiple tasks imposed by the GA-T. The greatest difficulty in performing the GA-T ADLs was attributed to squatting to accomplish the shelving tasks, although other complaints reported at the end of the test (including the stair tasks and the manual tasks) differentially impacted the total test time. Moreover, there were correlations between GA-T time and hand function and HRQoL. Therefore, by including activities that require both lower limb and upper limb performance, the GA-T may be an additional tool to evaluate patients with acromegaly as it aggregates important functional information.
Footnotes
Acknowledgments
The authors wish to thank the Conselho Nacional de Desenvolvimento Científico e Tecnólogico (CNPq; Grant number #302215/2019-0), Brazil, Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ; Grant number #E-26/202.679/2018 and #E-26/010.002124/2019), Brazil, and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES, Finance Code 001), Brazil.
Conflict of interest
The authors have no conflict of interest to report.