
Abstract
BACKGROUND:
Low back pain is a common problem in pregnant woman. Elastic tape is an alternative method that may reduce low back pain.
OBJECTIVES:
To compare the effect of elastic tape to placebo tape in the treatment of low back pain in pregnant women.
METHODS:
Forty pregnant women were allocated into two groups: elastic group (
RESULTS:
After the application of stretched elastic tape, lower back pain was significantly reduced by 29.4% (
CONCLUSION:
Elastic tape reduced back pain and improved physical function in pregnant women compared to the placebo tape.
Introduction
Low back pain that begins from about the second trimester and peaks around the third trimester [1] affects approximately 50% of all pregnant women (range 25%–90%) [2]. It is thought that low back pain in pregnant women is caused by their increasing body weight and abdominal size which subsequently enhances lumbar lordosis. In addition, the hormonal changes during pregnancy produce ligament laxity leading to instability of the spine and pelvic girdle and thereby low back pain [2]. Unfortunately, low back pain in pregnant women negatively affects their physical, psychological and social well-being [3] and, surprisingly, effective management of back pain during pregnancy is relatively unresearched [4].
Elastic tape is a therapeutic tape that can be stretched out to 140% of its original length. Kinesio tape is an elastic tape that was developed by a Japanese chiropractor in the 1970s, and is currently used to treat pain, injury and abnormal function of muscles and joints. It is believed that elastic tape may have a number of mechanisms by which it works including supporting injured muscles and joints, stimulating fascial function, and reducing pain by deactivation of nociceptive stimuli [5]. Elastic tape also stimulates the circulation of blood and lymph by reducing pressure on the floor of the connective tissue under the skin [5].
The effects of elastic tape in non-specific low back pain has been extensively studied [6], but there are only a few studies that examine the effects of Kinesio tape on lower back pain during pregnancy. Kaplan et al. conducted a study in 65 pregnant women with a gestational age between 10 and 30 weeks [7], and found that lower back pain decreased and functional ability improved significantly after five days of wearing the Kinesio tape compared wearing control tape (i.e. no stretch tape). Kalinowski and Krawulska conducted a crossover study in second and third trimester pregnant women and found that Kinesio tape significantly reduced pain intensity on the second and seventh post-application days and improved the physical functioning score on the seventh post-application day compared to placebo [8]. However, some researchers question the beneficial effect of elastic taping in relieving lower back pain [6]. More studies are required to provide stronger scientific evidence for the use of Kinesio tape on lower back pain in pregnancy [9]. In addition, the effects of elastic tape in the treatment of back pain solely in the third trimester in pregnant women, compared with placebo tape, has not been studied. During the third trimester when the fetus is largest and stress on the lumbar spine is greatest, we would expect that any positive effect of elastic taping would be most beneficial.
This study aims to compare the effect between elastic tape and placebo tape in the third trimester in pregnant women. The primary outcome of this study is the change in patients’ pain score. Secondary outcomes include the effect of elastic tape on the pregnant women’s disability score, walking speed and posture change.
Materials and methods
Participants
This was a double-blind randomized controlled trial on pregnant women who attended an antenatal clinic at Srinagarind Hospital, Khon Kaen, Thailand from July 2018 to September 2018. The inclusion criteria were: pregnant women with mechanical low back pain and aged between 18 and 40 years old, with a gestational age between 28 and 38 weeks. In addition, the pregnant women also had to have a lower back pain score of at least one on the visual analog scale (VAS), be able to walk at least 20 meters and have no contraindication for taping such as allergies or skin lesions. The exclusion criteria were: pregnant women with severe musculoskeletal disorders such as disc herniation or spinal fracture, a history of chronic back pain before pregnancy and high risk pregnancy cases such as twins or a pregnancy with underlying diseases. The study conformed to the Physiotherapy Evidence Database (PEDro) for methodological quality (Appendix) and attained a score of 10 as rated by the principal investigator of this study which represents a study of excellent quality. The study was approved by the Ethics Committee Human Research, Faculty of Medicine, Khon Kaen University under project no. HE611027.
Forty participants were divided into two groups according to the gestation period (28–32 and 33–38 weeks). The participants were allocated by block of four randomization into two groups: elastic group (
Both groups received information about the nature, cause, and management of low back pain in pregnancy. The participants were asked not to exercise 24 hours before starting the intervention and patients did not visit a physiotherapy during the study. A simple analgesic such as paracetamol was allowed for severe pain, however, no study participants took any pain killers throughout the experiment.
Characteristics of the participants
Characteristics of the participants
Data are mean (SD). VAS, Visual analog scale, RMDQ, RolandMorris Disability Questionnaire.
Taping technique at the lower back area. A. The I-shaped sections of tape were stretched as the participant bent forward and were applied vertically from the sacroiliac joint to the twelfth rib along both erector spinae muscles. B. The two I-shaped sections of tape were stretched and applied horizontally and covered the spinous process to the coronal line on each side of the body around the fourth-fifth lumbar spine and the last rib level.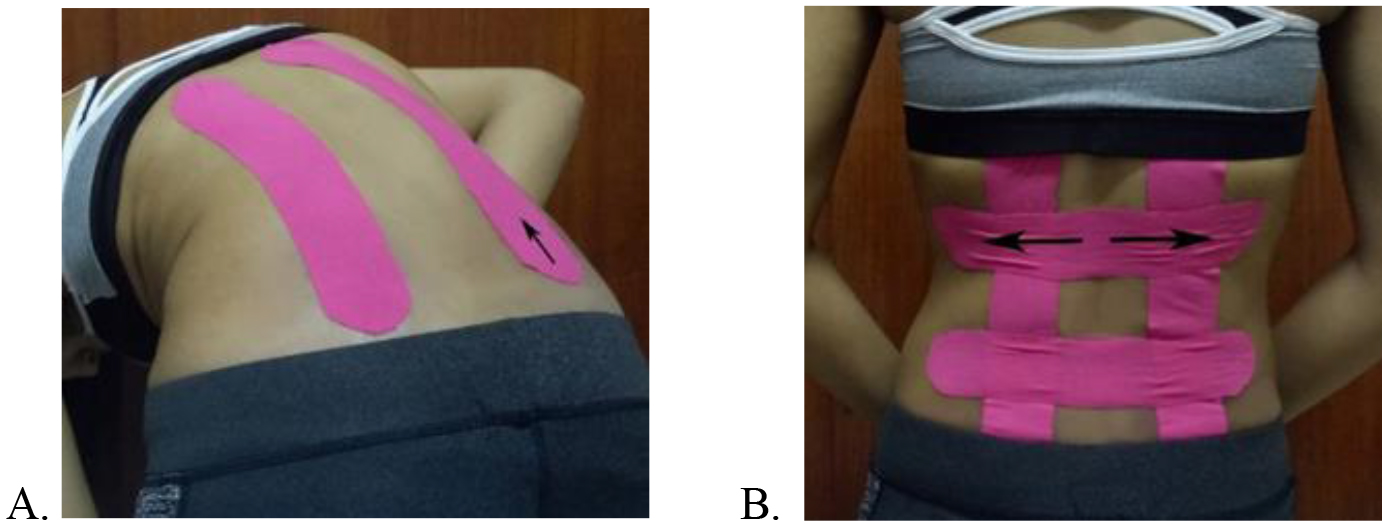
Total posture translation in frontal and sagittal view analyzed form the mobile application. The summation of deviation of postural line from the ideal line. A. in frontal view (total posture translation in frontal view) and B. in sagittal view (total posture translation in sagittal view).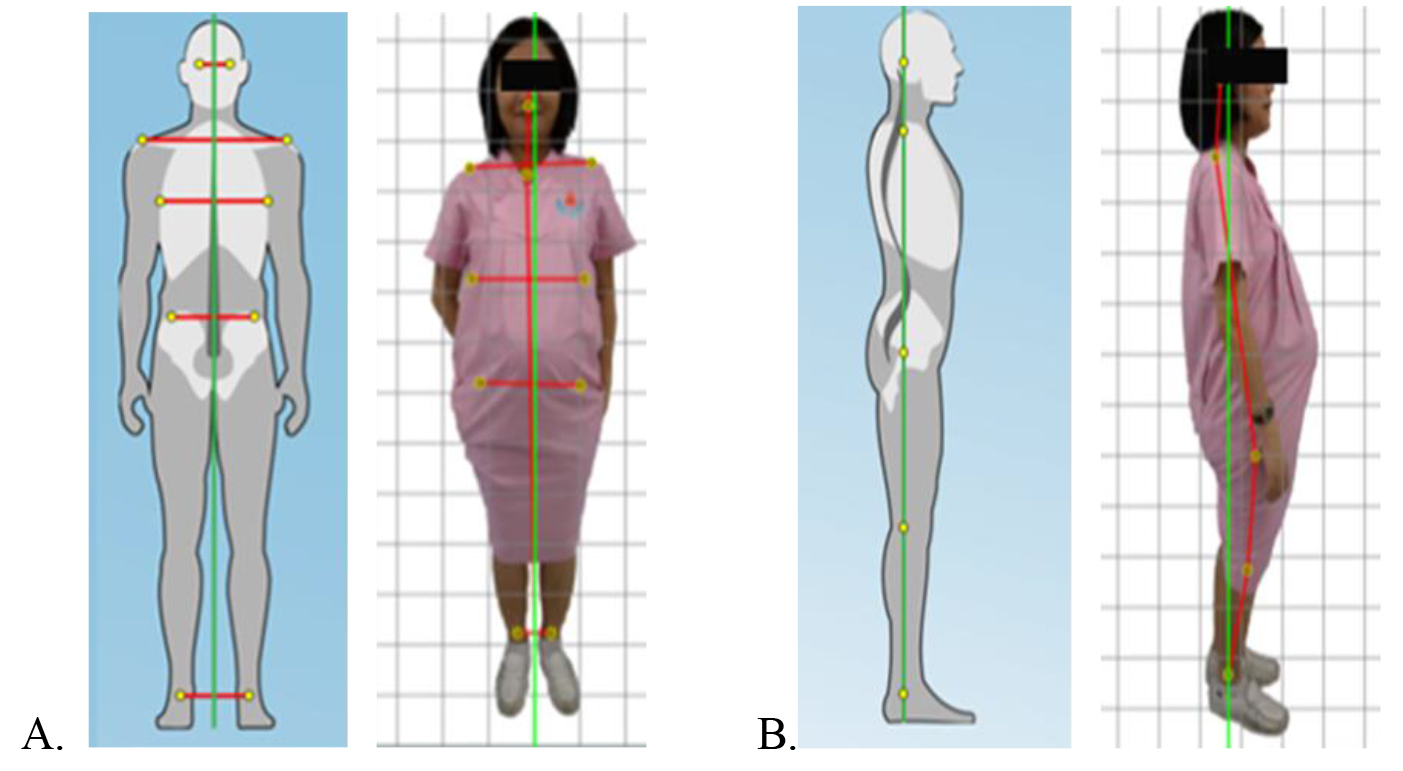
In the elastic group, the participants were taped with 5 cm width and 0.5 mm thickness elastic tape (Kinesio tex
Outcome assessment
Back pain
Ratings of back pain severity at the time of testing
Comparison of pain score, walking speed and RMDQ score at baseline, immediately and one week after wearing the tape (within and between groups)
Comparison of pain score, walking speed and RMDQ score at baseline, immediately and one week after wearing the tape (within and between groups)
Data are mean (SD) along with raw mean difference and 95% confidence interval for the between group change scores.
were made using a VAS. The VAS score ranged from 0 to 10 points with a straight line of 10 centimeters from 0 (no pain) to 10 (the worst pain). The VAS procedure was explained to each participant prior to the study.
Physical function was evaluated using the Roland-Morris Disability Questionnaire (RMDQ). This is a self-administered questionnaire with 24 questions that produces a score from 0 to 24. This paper and pencil questionnaire had been translated into Thai and has good internal consistency [10]. In addition, we also measured the time to walk 20 meters along a straight flat line. Walking speed that is related to low back pain intensity [11] was calculated by dividing the distance (20 m) by the time taken [12]. The average of two tests of walking speed (5 minute seated rest between tests) was analyzed.
Postural change
Posture change was evaluated using a mobile phone application taking photographs of the participants in the frontal and lateral view. The same researcher took pictures each time within about two meters distance from the participant. The pictures were analyzed by the Android application PostureScreen Mobile. The mobile application has shown strong rater reliability and construct validity for postural analysis [13]. The participants were marked on the acromioclavicular joint, episternal notch, lateral side of the eighth rib, anterior superior iliac spine, greater trochanter, lateral femoral epicondyle, center of the ankle. The total postural translation in frontal and lateral views were analyzed (Fig. 3).
2.3.3.1. Total posture translation in frontal view
The application created an ideal line through the center of the body perpendicular to the ground in frontal view. The application also created a postural line between each pair of landmarks from the head to the ground. The summation of the deviation of the postural line from the ideal line at each landmark was analyzed (Fig. 2A).
2.3.3.2. Total posture translation in sagittal view
Similar to the frontal view the application created an ideal line through the center of the body perpendicular to the ground in the sagittal view. The application then created a postural line from the head through the shoulder, greater trochanter, knee down to the ankle joint. The summation of deviation of the postural line from the ideal line in each landmark was analyzed (Fig. 2B).
The outcomes were evaluated before (baseline), immediately after applying the tape (immediately post-tapping) and after one week of wearing the tape (one week tapped). Participants were told to continue living and moving as normal for the whole week and not to change their behaviors.
Statistical analysis
The data were analyzed using SPSS version 26 (SPSS Inc., Armonk, USA). The data are presented as mean and standard deviation (mean
The sample size estimation was calculated based on a type I error (
The effect of elastic tape and placebo tape on pain intensity (visual analog score) at baseline, immediately post-taping and one week taped. 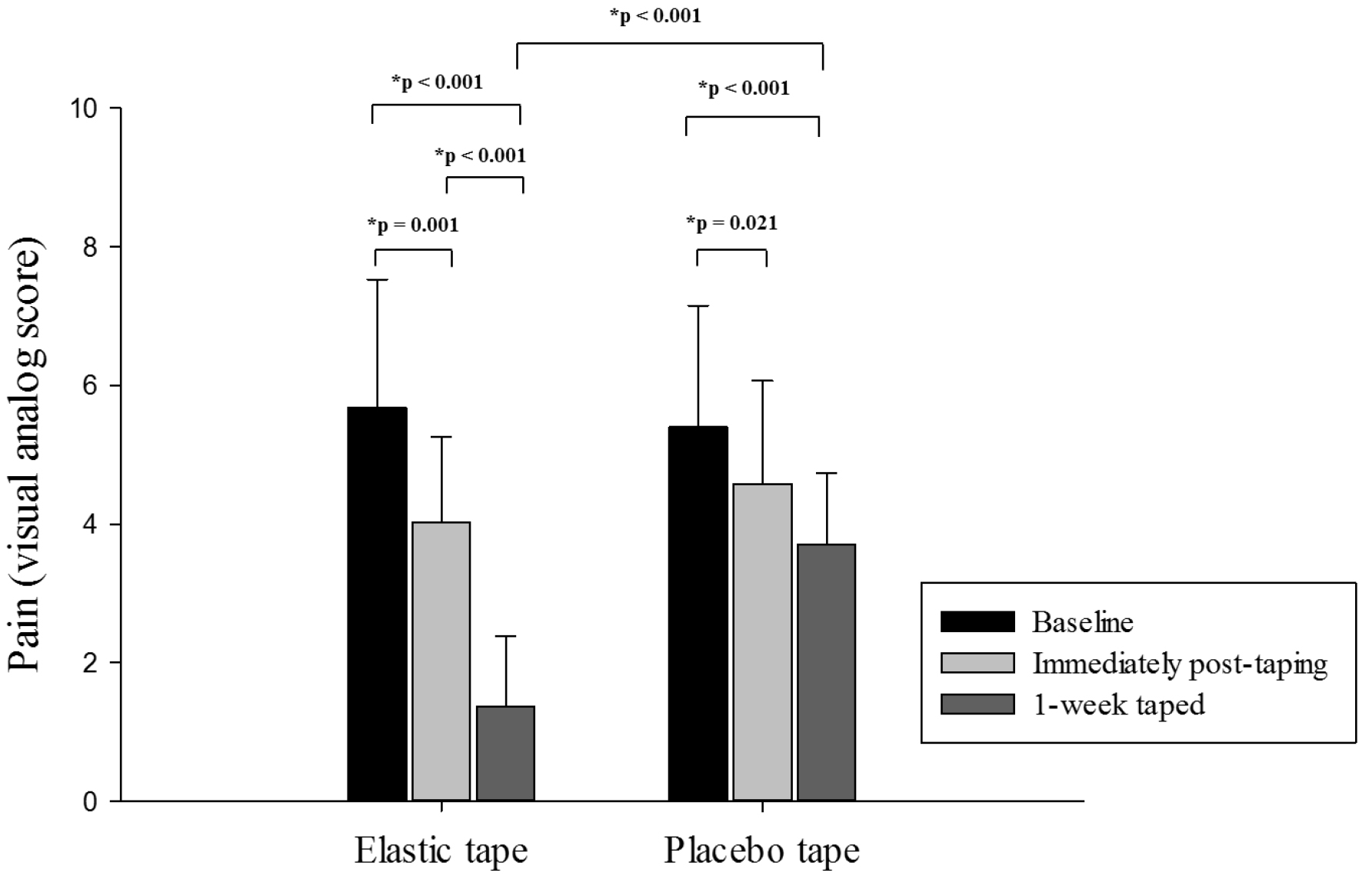
The effect of elastic tape and placebo tape on functional ability (RMDQ, Roland-Morris Disability Questionnaire) at baseline, immediately post-taping and one week taped. 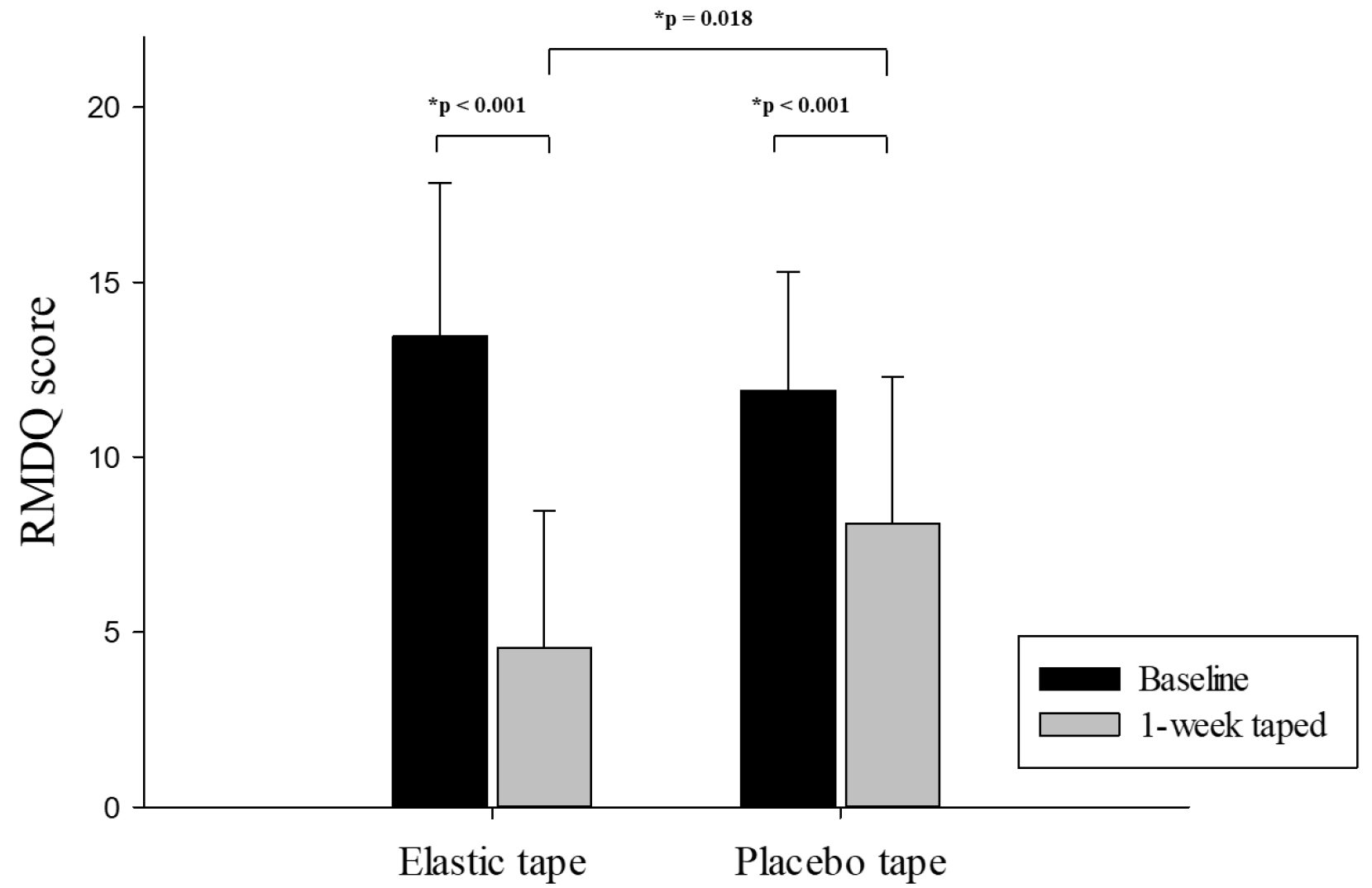
The effect of elastic tape and placebo tape on walking speed at baseline, immediately post-taping and one week taped. 
The characteristics of the participants of the elastic and placebo tape are presented in Table 1. At baseline there were no significant differences between the groups for the measures taken. In addition, no adverse effects of taping such as allergies or skin irritations were observed.
Immediately after applying the stretched Kinesio tape to the participants in the elastic group their subjective back pain score (as measured by the VAS) significantly decreased by approximately 29.4% (dropped from 5.7 to 4.0,
One week after applying the tape, the elastic group had significantly reduced their disability score from 13.5 to 4.6 (
Immediately after applying the stretched elastic tape, the elastic group had significantly increased their walking speed, which remained improved through to one week after wearing the tape. Similarly, applying the non-elasticized tape to the placebo group, immediately improved their walking speed which was maintained through to the following week (Fig. 5). There was no significant difference in walking speed change between groups.
Taping the lower back with stretched elastic (elastic group) or non-stretched elastic (placebo group) tape for one week did not significantly alter posture as measured by the PostureScreen Mobile application.
Discussion
In this study, both Kinesio and placebo taping improved back pain, walking speed and reduced perception of disability (RMDQ score) compared to baseline. However, Kinesio tape had a significantly greater effect on the reduction of back pain and perceived disability than the placebo tape after one week of wearing the tape. This study did not find any postural changes from the midline in either the horizontal or sagittal view as a result of wearing Kinesio or placebo tape.
Previous research has revealed both beneficial and non-beneficial effects of Kinesio tape on non-specific chronic low back pain. A meta-analysis recently concluded that Kinesio tape had no positive effect compared to placebo taping in pain reduction, but it significantly improved disability scores [6]. However, only a few studies examined the effects of such taping on final trimester pregnant women. Our study showed that elastic Kinesio tape reduced low back pain from distressing pain to mild or annoying pain and improved physical functioning in final trimester pregnant women compared to placebo taping.
While this is not the first study that investigates the effects of elastic taping on the reduction of lower back pain and disability in pregnant women [7, 8], previous studies either lacked control groups [7] or did not control for gestational age and thus size and weight of the growing fetus [7, 8]. Our study indicated that elastic taping has a greater effect than non-elastic taping on reducing lower back pain in pregnant women with a similar gestational age.
Mechanisms behind the positive effects of elastic taping include improved lower back stability [14] and increased proprioception [15] resulting in an improvement of postural control. It is also thought that elastic taping may help to widen the interstitial space between the skin and the fascia resulting in increased blood circulation [16] which may help to remove pain-causing substances [17].
Kinesio tape may also improve back muscle activity and posture change. Kang et al. showed that application of postural taping on the lower back area in chronic low back sufferers decreased the back extensor muscle electromyographic activity and rate of perceived exertion while also improving the kinematics of the lumbo-pelvic-hip complex assessed by a 3D motion capture system [18]. The current study did not find any difference in postural correction after taping in pregnant women as assessed by a mobile phone application (PostureScreen Mobile). The mobile phone application may not be sensitive enough to detect small sectional back postural changes from taping. In addition, the participants wore a loose dress (Fig. 3) during the posture screening which may have reduced the accuracy of finding the postural landmarks for the phone application.
The limitations of this study include the fact that it would have been ideal to measure the extent to which the effects of taping lasted and we recommend future studies to continue to measure the effects of taping into the weeks after the tape has been removed. In addition, previous research suggested that the duration of taping should be two weeks [9], therefore our results may not reflect the full extent of adaptation that may occur if the taping period was extended. Also, we recognize that while we initially blinded patients to the intervention, some patients over time may have correctly guessed which intervention group they were in. Finally, a more sensitive measure of postural change would be required in future research to confirm whether postural change caused any improvement in pain reduction.
Conclusion
Elastic tape has a positive effect on reducing lower back pain and improves physical function in pregnant women in their third trimester compared to placebo tape. However, taping had no effect on walking speed or postural changes in heavily pregnant women.
Footnotes
Acknowledgments
The authors would like to acknowledge Dr. Jitjira Chaiyarit, Clinical Epidemiology Unit, Faculty of Medicine, Khon Kaen University for statistical advice and analysis and furthermore thank the participants who were involved in this study.
Conflict of interest
None to report.