
Abstract
BACKGROUND:
The screw-home mechanism (SHM) plays an important role in the stability of the knee. Accordingly, the analysis of tibial rotation patterns can be used to elucidate the effect of SHM-related factors.
OBJECTIVE:
The purpose of this study was to compare the magnitude of the angle and the pattern of SHM between passive and active movements.
METHODS:
We studied twenty healthy males, of which the angle of knee flexion-extension and tibial longitudinal rotation (TLR) during active and passive movements were measured using the inertial measurement unit. Student’s
RESULTS:
Significant differences were found in the TLR between the active and passive movements (
CONCLUSION:
The SHM increased abruptly during the last 20
Keywords
Introduction
Biomechanical instability of the knee joint leads to tissue damage and severe pain that can be prevented via appropriate coordination of knee-related factors [1, 2]. In other words, the joint is injured by moving beyond the threshold of stability. Although the knee joint is a structurally modified hinge joint, it is accompanied by rotational motion owing to the biomechanical coordination among knee-related factors. This kinematic phenomenon is referred to as the screw-home mechanism (SHM), and plays an important role in the stability of the knee [3, 4, 5, 6, 7, 8].
Two different arguments were proposed to explain the SHM mechanism [3, 9]. The first involved knee movements along a consistent path, and the second considered various movements in an envelope. The controversy was attributed to the tibial longitudinal rotation (TLR) across a range of magnitudes and periods during the knee flexion-extension direction, although the external rotation was accompanied by extension [3]. A previous study reported that there was no difference in the absolute value of rotation, abduction/adduction, and articular movement during passive flexion of the knee compared with passive extension using unloaded postmortem human knee specimens [9]. This result suggests that the coupled movements involving knee flexion and extension follow a consistent path. However, the path and coupled movements are affected by gravity, force of muscle activation, weight-bearing, and loaded conditions [5, 9, 10, 11, 12, 13]. In particular, SHM has been defined as the tibial rotation involving the last angle of knee extension. In contrast, several published studies indicated that the TLR occurred continually over a wider range during passive knee movements [3, 9, 13, 14]. It was insufficient to interpret the influence of SHM-related factors because the results of tibial rotation of the knee joint varied according to the condition.
An initial study of the SHM was conducted using autopsy specimens [4]. Subsequently, the TLR was investigated with the actuator to reproduce muscle contraction around the knee [11]. The SHM affected the muscle action in the knee kinematics of autopsy specimens. The SHM was measured with the use of three-dimensional magnetic resonance imaging (MRI) at specific angles in live subjects that provided high-resolution outcomes that facilitated the analysis of structural elements related to SHM [15]. In particular, Heller et al. reported longitudinal rotation at the flexion angles of 0
Analysis of patterns of changes combined with tibial rotation can be used to elucidate the effect of SHM-related factors. In the current study, we compared the absolute displacement and the pattern of SHM between passive and active movements in non-weighted bearing conditions with the use of MEMS IMU. The working hypothesis is that the magnitude and timing of TLR may vary between passive and active movements.
Methods
Subjects
This study was performed according to the protocol approved by the Institutional Review Board at the Sun Moon University (SM-201703-011-1). Twenty healthy young adults (20 males; age, 22.43
Test procedure
Each subject sat on a chair and performed active and passive knee flexion-extension-flexion motions without bearing any weight on the tested knee. In the active movement trial, subjects were asked to extend knees from the flexed to the fully extended positions for 2 s and repositioned them to the flexed position for 2 s with the assistance of a metronome. The passive movement trial was also conducted in the same procedure as the active trial, but the knee movement was attributed to the manual force applied by the physical therapist. After confirming that the subject’s muscles were relaxed, the therapist hung the sling on the heel (calcaneus) pulled it to a fully extended position, and then allowed gravity to return it to the flexed position.
Data acquisition and analysis
Data acquisition and analysis were performed based on procedures reported earlier [21]. Angles of knee flexion-extension and TLR during active and passive movements were measured using the MEMS IMU (EBIMU24GV3, E2BOX, Seoul, Republic of Korea) at 40 Hz. The MEMS IMU consisted of a three-axis accelerometer (
Attachment of MEMS IMU sensors and test procedure (A: flexion and B: full extension position) during the movement trial of the knee joint.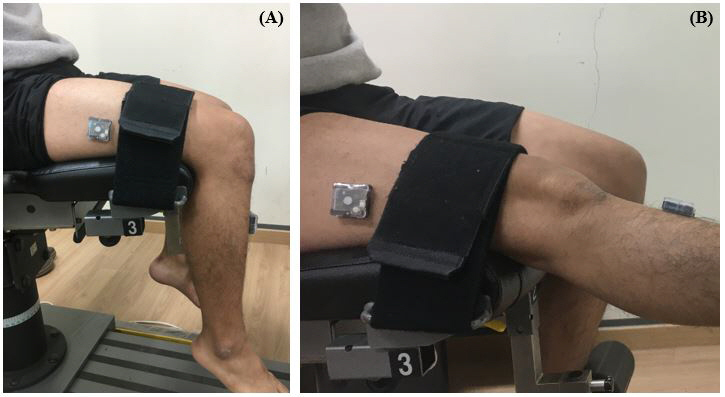
The kneejoint angle was estimated as the relative angle between the thigh and shank segments using SMULeg software (SMULeg, XENART, Daejeon, Republic of Korea). Before performing trials of knee movement, the subject was asked to perform flexion-extension motion to determine the physically meaningful axes of the knee joint in the local coordinate system of the sensors [22, 23]. The fully extended knee (achieved manually by the examiner) was considered as the zero position. The longitudinal rotation of the tibia was shifted to a zero angle during knee flexion, which was the starting position in the examination. Positive angles indicate flexion and external rotation, respectively. Both passive and active movements (flexionextensionflexion) were time normalized to the range of %100% with a visual three-dimensional (3D) software (C Motion Inc., Germantown, MD, USA).
Each angle of the knee flexionextension and TLR were calculated by subtracting the angle in the flexed position from the angle in a fully extended position. The timing of the peak angle (TPA) was defined as the instant at which the maximum knee extension and tibial external rotation angles were achieved. The coefficient of multiple correlation (CMC) was used to assess the waveform similarity in both movements [18]. The equation for obtaining CMC is as follows:
where
where
where
The independent
Comparison of the angle and TPA of knee flexion-extension and TLR according to active and passive movements of the knee
Comparison of the angle and TPA of knee flexion-extension and TLR according to active and passive movements of the knee
All results are expressed as mean
Comparison of knee flexion-extension angles according to active and passive movements of knee flexion-extension-flexion. Dashed and solid lines represent active and passive movements, respectively. The positive values represent knee flexion. Waveform similarity (coefficient of maximum correlation (CMC) 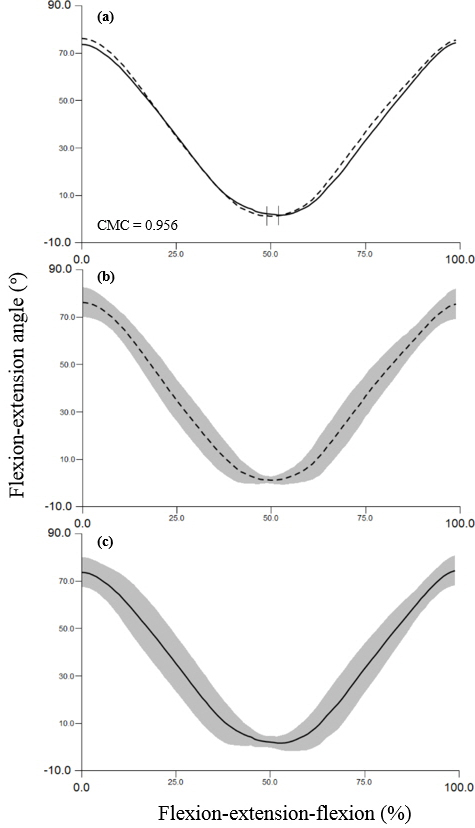
Comparison of tibial longitudinal rotation (TLR) angles between active and passive movements (knee flexion-extension-flexion motion). Dashed and solid lines represent active and passive movements, respectively. The positive values represent tibial external rotation. Waveform similarity (CMC 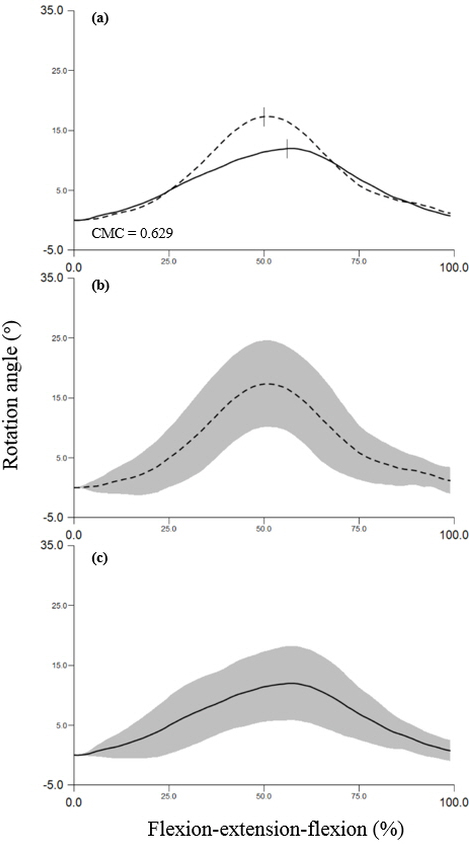
Movement path of TLR angle according to the knee flexion-extension angle during flexion-extension-flexion motion. Dashed and solid lines represent active and passive movements, respectively. The positive values represent knee flexion and external rotation of the tibia.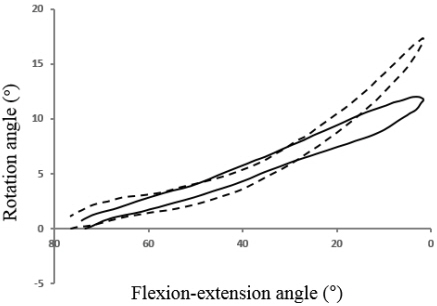
The angles and the TPA according to active and passive movements are shown in Table 1. The magnitude of TLR was 18.98
Figures 2 and 3 present the CMC results, and the mean and standard deviation of flexion-extension and TLR angle for the two movements, respectively. The knee flexionextension waveform similarity was excellent (CMC
Discussion
The present study was conducted using MEMS IMU to demonstrate the changes in TLR by active and passive movements. Recently, the nine-axis inertial sensors with a microcontroller were miniaturized and the increased reliability of the biomechanical data acquisition was confirmed [19, 25]. To analyze the SHM mechanism, we focused on the relative comparison and pattern rather than on the absolute displacement, because the angle of TLR showed a large variation in each of the studies reported previously depending on the equipment and experimental conditions [3, 5, 9, 10, 11, 12, 13, 14, 26]. Furthermore, the tibial rotation values varied for each subject in a rig design study that used postmortem specimens [9]. In this study, the similarity of the flexionextension waveforms demonstrated excellent CMC values between active and passive movements and confirmed the overall similarity of joint angle waveforms acquired at different experimental conditions [24]. Therefore, it appears that the flexionextension angle was synchronized between active and passive conditions. In contrast, the CMC value of longitudinal rotation showed poor correlation between the two conditions. The longitudinal rotation of the active motion (18.98
In this study, the TLR of the passive movement was increased gradually in both flexion and extension and ranged between 0
In the current study, the TLR of the active movement showed a statistically significant difference from the passive movement. The magnitude of TLR increased, and the timing of TPA was rapid during active knee extension. The dominant muscle in our experiment was the quadriceps during the knee movement because of the force and direction of gravity in the sitting position. In the two previous studies, the force related to knee muscles was reproduced with the use of an actuator on the knee specimens from postmortem humans, and the TLR was reduced relative to the loading of the knee [11, 29]. The load of anterior cruciate ligament (ACL) was increased in the active trial [16] because the force of quadriceps muscle pulled the tibia forward and ensured that the angular orientation ranged between 0
Two previous studies reported that the in situ force in the ACL decreased at 0
In conclusion, we demonstrated the changes in magnitude and pattern of SHM between passive and active movements in unconstrained knees in vivo using MEMS IMU. The TLR rapidly increased from the last 20
The following study limitations should be considered during the interpretation of the results. First, this study investigated biomechanical data based on in vivo IMU. Although biomechanical data using skin markers were affected by inaccuracies of skin movement, this study minimized the effect of bias by changing only the conditions of movement. Second, to minimize the diversity of dependent variables, we measured the range within 90
Footnotes
Acknowledgments
This work was supported by the Sun Moon University Research Grant of 2019.
Conflict of interest
The authors have no conflict of interest to report.