
Abstract
BACKGROUND:
Teachers present with shoulder musculoskeletal disorders, which result in pain and poor shoulder function.
OBJECTIVE:
To determine the effect of an eight-week shoulder rehabilitation intervention on pain and function, range of motion and muscle strength among teachers.
METHODS:
Thirty teachers presenting with shoulder pain were recruited and divided into equal control and experimental groups. The intervention group participated in an eight-week rehabilitation programme. Pre- and post-intervention measurements included the scapular position test, range of motion, muscle strength measurements as well as a shoulder rating questionnaire.
RESULTS:
There was a significant improvement in the experimental group’s internal range of motion for the dominant (
CONCLUSION:
The implementation of a rehabilitation programme in schools should be considered to manage the prevalence of shoulder musculoskeletal disorders among teachers.
Introduction
The teaching profession requires prolonged standing and use of body movements that place a demand on the musculoskeletal system. Due to such demands, school teachers have a high prevalence of musculoskeletal disorders (MSDs) compared to other occupational groups [1]. These musculoskeletal disorders account for one of the most expensive occupational health problems in developing and developed countries [2]. Among school teachers, MSDs are reported as one of the leading causes of ill-health retirement [3]. The outcome for MSDs among teachers includes taking more sick leave days [4], retiring early [3], chronic pain and functional impairment [5]. Lower back, shoulder and neck pain are the three most commonly reported conditions among teachers presenting with MSDs [6, 7, 8, 9, 10]. The prevalence of shoulder MSDs, in particular, is reported to be within a range of 15–83.1% in various countries such as China, Sweden, Taiwan, Egypt, Saudi Arabia and Botswana, with the average prevalence reported at 58% [11]. A more recent study conducted in Nigeria reported the prevalence of shoulder pain as 11.7% among school teachers [12]. The highest prevalence of 83.1% was reported among South African primary school teachers [13].
Generally, there is an association between shoulder MSDs and reduced range of motion in patients [14]. Shoulder MSDs have also been associated with reduced muscle strength including shoulder abductors, internal and external rotators [15, 16]. When an injury exists, it is almost always associated with loss of range of motion, which may be due to pain, swelling, muscle guarding or spasm [17]. Musculoskeletal disorders result in impairment in muscular strength and endurance. This muscle weakness can result in abnormal movement and can impair normal functional movement [17]. .Rahman and Warikoo [18] have found that teachers who experienced shoulder pain, presented with an altered scapular position. Furthermore, the study concluded that scapular dyskinesia is the cause of shoulder pain among teachers.
In spite of the prevalence of shoulder MSDs and its implications [1, 2, 3, 4, 5], to the best of the authors’ knowledge, no study has addressed the management and prevention of such MSDs among teachers, specifically via an intervention.
Therefore this study aimed to determine the effect of an eight-week shoulder rehabilitation intervention on pain and function, range of motion and muscle strength among teachers. Shoulder function in this study is defined as the ability to perform work, daily activity tasks and recreational activities with the shoulder. The hypothesis of the study was that an eight-week rehabilitation intervention programme would reduce pain, improve shoulder range of motion, muscle strength as well as shoulder function among teachers.
Methods
Research design
This was a quasi-experimental study design with non-randomised, intact control and experimental groups.
Population and sample
Two public primary schools were purposively selected from a local district in Durban, South Africa. Participants from one school were the control group, and participants from the other school were the experimental group. A total of fifteen participants were recruited from each school. The experimental group was involved in the eight-week shoulder rehabilitation intervention programme, whereas the control was not involved.
Inclusion and exclusion criteria
Participants from both the control and the experimental groups were included in the study if they reported shoulder pain. Additionally, participants were included if they were involved in classroom teaching rather than being primarily office-based. Exclusion criteria consisted of teachers that had a macro-trauma to the shoulder; a dislocating shoulder; a history of shoulder surgery; swelling and inflammation to the shoulder; and undergoing treatment for shoulder pain during the intervention period, all of which were self-reported by the participants.
Arm positions for measuring scapular position using lateral scapular slide test. a: neutral; b: 40–45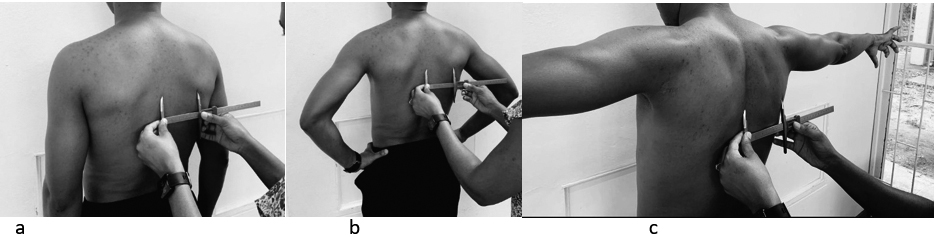
Range of motion measurements. a: flexion; b: abduction; c: internal rotation; d: external rotation.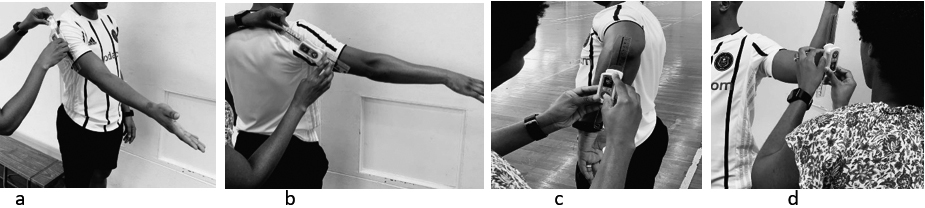
The study was approved by the University’s Biomedical Research Ethics Committee (BF 225/18) prior to commencement. Approval was further obtained from the provincial Department of Basic Education and school principals. The study was then presented to the teachers, and those who were willing to participate and met the inclusion criteria gave their written consent to participate in the study. The shoulder rating questionnaire (SRQ), scapular position tests, shoulder range of motion and shoulder strength tests were conducted pre- and post-intervention on all participants.
Shoulder rating questionnaire
The shoulder rating questionnaire (SRQ) was used to determine the symptoms and function of the shoulder; the severity of the pain and limitations to daily activities, work and recreational activities for the participants [19]. The questionnaire has been reported to be valid, reliable and responsive to change [20]. The questionnaire consists of five domains, including global assessment, pain, daily activities, recreational/athletic activities and work. An overall score is also calculated from these five domains. An additional section includes a question about the degree of satisfaction of the participants about the shoulder, as well as ranking the areas in which the participants wish to see most improvement. The answers to questions were converted to numerical values for analysis.
Scapular position
A lateral scapular slide test (LSST) was conducted using a sliding caliper (martin type) to measure the scapular position on the dominant and non-dominant sides of the participants. The measurements were taken in three different positions: shoulder in neutral; at 40–45 degrees of coronal plane abduction; and at 90 degrees abduction and internal rotation. The test measures the distance from the inferior angle of each scapula to the nearest spinous process in the three positions [21]. An asymmetry of 1.5 cm between the right and the left side is considered a threshold for abnormality [22]. An illustration for the scapular position measurements is presented in Fig. 1.
The participants were requested to wear minimal clothing during the measurements so that the markings could be accurately located.
Range of motion
An EasyAngle digital goniometer was used to measure shoulder range of motion [23]. The movements measured were shoulder flexion, abduction, and internal and external rotation, as illustrated in Fig. 2. The examiner ensured that each participant did not compensate by leaning forward or backwards and shrugging the shoulders during the measurements. The use of a goniometer for measuring active shoulder flexion, abduction, internal and external rotation has been reported to have excellent intrarater reliability with intraclass correlation coefficient (ICC) of
Muscle strength
Muscle strength was measured using the MicroFET 3 dynamometer which provides an objective measurement of the force applied against the machine. This device is reported to be more accurate than manual muscle testing, i.e. against the resistance of the examiner’s hand [26]. The measurements performed were flexion, abduction, internal and external rotation, as illustrated in Fig. 3.
Muscle testing measurements. a: flexion; b: abduction; c: internal rotation; d: external rotation.
Algorithm for developing the intervention programme.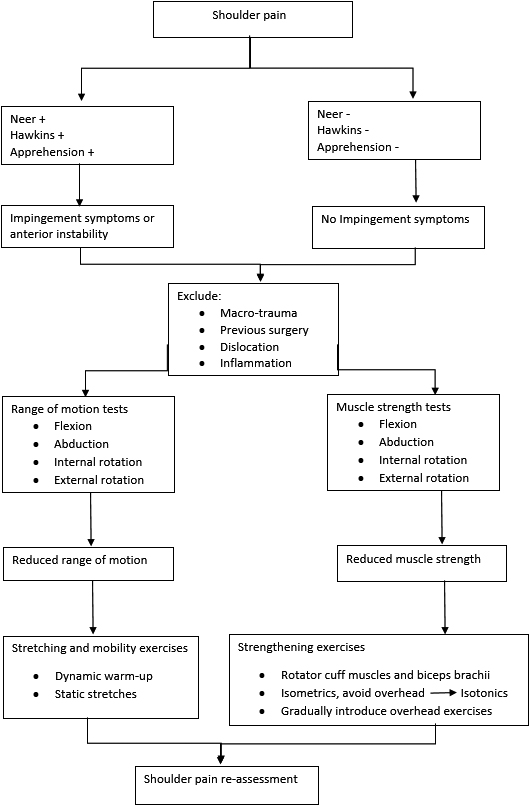
Measurements were evaluated by three trained individuals, each designated a station, i.e., one was taking measurements of scapular position, one measuring range of motion and one measuring muscle strength throughout the study pre- and post-intervention.
Summary of exercises performed in the intervention programme.
The experimental group followed a shoulder rehabilitation intervention programme twice a week for a period of eight weeks.
The intervention programme was designed based on the lack of range of motion and poor muscle strength that the participants presented with. The programme focused on improving range of motion and flexibility, as well as strengthening the stabilising muscles of the shoulder, focusing on rotator cuff muscles (supraspinatus, infraspinatus, teres minor, subscapularis) and biceps brachii (long head). The algorithm for designing the rehabilitation programme is presented in Fig. 4. The initial phase included isometric exercises and avoided overhead exercises to avoid aggravating shoulder pain. As the programme progressed, the overhead activites were introduced to prepare the shoulder for the daily activities involved in teaching such as writing on the chalkboard.
The intervention was conducted at the school in the afternoons, at the end of the school programme on Mondays and Thursdays. The duration for each session was 25–30 minutes. The programme included a dynamic warm-up, strengthening and neuromuscular control, as well as static stretching exercises, summarised in Fig. 5.
The dynamic arm warm-up included bodyweight arm circles; neck rotations; shoulder shrugs/rolls; horizontal adduction/abduction; internal/external rotation; adduction/abduction and shoulder flexion. These were performed 10 times each, before commencing with strengthening exercises.
The static stretches were performed at the end of the programme following strengthening exercises and included lateral neck flexion; forward flexion; chest stretches and shoulder stretches. Each stretch was performed twice, holding for 15 seconds.
The strengthening exercises were performed using resistance bands, progressing from light to heavier resistance as tolerated by each participant. No progression was allowed if a participant experienced pain or could not complete the required sets and repetitions.
Week one and week two consisted of isometric exercises, of which two sets of eight seconds-hold and three sets of ten seconds-hold were performed for week one and week two, respectively. The exercises for weeks one and two included shoulder flexion; abduction; scaption; external rotation and protraction.
Weeks three and four consisted of exercises from weeks one and two, progressed to isotonic exercises. Two sets of ten repetitions were performed in week three, while three sets of ten (same resistance) were performed in week four.
Additional exercises from previous weeks were added from week five to week eight, including horizontal abduction, shoulder press and wall push-ups plus. Two sets of ten repetitions were performed in week five, with heavier resistance from week four where applicable; three sets of ten repetitions for week six; and three sets of ten to twelve repetition for weeks seven and eight, with heavier resistance than week six, where applicable. Participants were re-assessed a week after completion of the eight-week intervention programme.
Muscle strength measurements post-intervention for the control and experimental groups. D 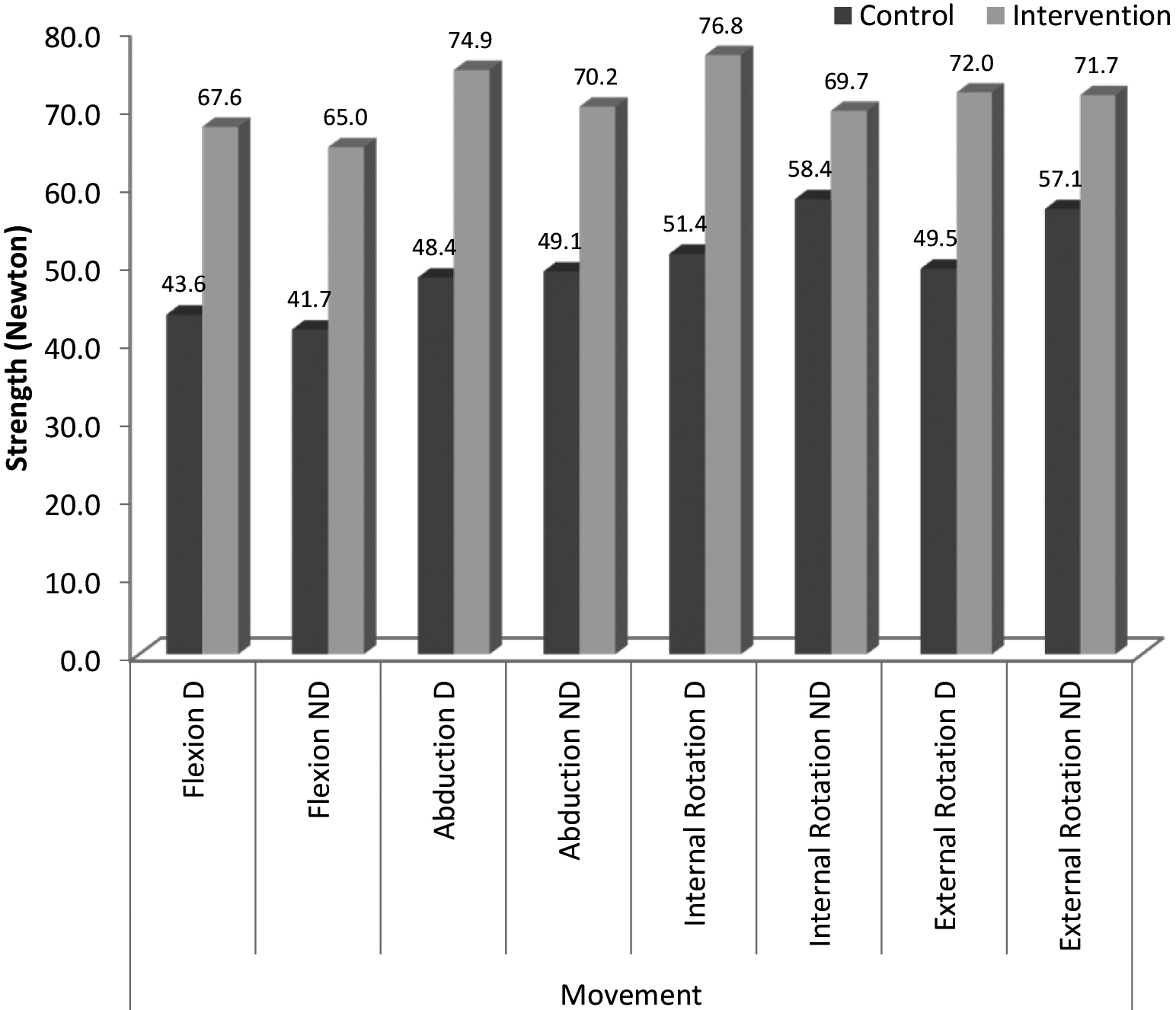
The difference in the scapular position between the right and left shoulder was calculated by subtracting the value for the non-dominant side from the value for the dominant side. This absolute value was used for analysis. The statistical package for social science (SPSS) was used to analyse data, using descriptive statistics including means and standard deviations where applicable. The analysis of covariance (ANCOVA) was applied to determine if the post-intervention measurements differ significantly between the control and experimental groups, after being corrected for by the pre-intervention measurements. Partial eta squared (
Results
Table 1 presents the characteristics of the participants in the control and experimental groups. The control group consisted of all females whereas the experimental group had 13 female and 2 male participants (86.7% and 13.3%, respectively). The control group had a mean age of 48.6 (
Characteristics of participants in the control and experimental groups
Characteristics of participants in the control and experimental groups
Scapular difference between the dominant and non-dominant side for the control and experimental groups
Post-intervention results for the shoulder rating questionnaire for the control and experimental group
There was no significant difference between the scapular position difference of the dominant and non-dominant sides for the control and experimental groups for all scapular positions measured (neutral, 40–45
Figure 6 shows the difference between post-intervention measurements of muscle strength for the control and experimental groups. There was a significant difference in muscle strength after the intervention between the control and experimental groups, including dominant flexion (
The shoulder rating questionnaire (SRQ) showed that there was a significant difference post-intervention between the control and experimental groups, with the experimental group showing improvement in global assessment; pain; ability to perform daily activities; the overall score and the overall satisfaction of participants with their shoulders. The results for the SRQ are presented in Table 3.
Participants were also required to rank the area in which they would most like to see an improvement (e.g. improvement in pain, work, daily activities or recreation activities). In the control group, 46.7% ranked pain as the most important area for improvement pre-intervention, and this increased to 53.3% ranking pain as the most important area for improvement, post-intervention although this was not a significant increase. In the experimental group, 66.7% ranked pain as the most important area for improvement, pre-intervention. Significantly, this dropped to 33.3% post-intervention (
This study aimed to determine if the eight-week shoulder rehabilitation intervention programme would be effective in improving shoulder pain and shoulder function, as well as shoulder range of motion and muscle strength among teachers. Findings showed that the intervention programme improved shoulder strength, reduced pain and improved function, resulting in the ability to better perform daily activities, as well as improved satisfaction with the shoulder.
The significant improvement in strength for all the movements tested (flexion, abduction, internal and external rotation) could be attributed to the shoulder rehabilitation intervention programme in the experimental group. Performing strengthening exercises two to three times a week is recommended to improve strength [29, 30]. This improved strength could potentially result in the ability of the joint to function better at work and daily activities that require use of the shoulder. There are no other known studies that have conducted a rehabilitation programme for shoulder pain among teachers for comparative purposes. However, there are studies reporting improved shoulder strength and function in various patients involved in eight-week rehabilitation or exercise programmes [31, 32, 33].
Shoulder internal range of motion improved significantly post-intervention in the experimental group for both the dominant and non-dominant sides. This could be attributed to the flexibility exercises which were included in the programme. Swain and Leutholtz [29] stated that lack of flexibility is associated with reduced ability to perform activities of daily living. .Prentice [17] also stated that incorporating flexibility exercises in the rehabilitation programme helps to improve the range of motion and joint functioning. However, no significant improvement was observed in shoulder flexion, abduction and external range of motion. This could indicate that the duration (eight weeks) and frequency (twice a week) of the intervention programme was not enough to elicit significant improvement. Regular stretching exercise improves range of motion, although not immediately [30]. Furthermore, stretching exercises need to be performed at least five times a week to promote range of motion improvements [34].
The shoulder rating questionnaire (SRQ) results showed no significant difference in the ability to perform work activities and recreational/athletic activities between the control and experimental groups, post-intervention. This could be because the demands involved in the teaching profession, such as prolonged standing and elevated arm position while writing on the chalkboard [7, 18, 35, 36], were not addressed; and the demands of recreational/athletic activities might have been more than the shoulder strength gains. Hence, the shoulder is still being overloaded at work and during such activities. Refraining from work activities that overloaded the shoulder, and gradually reintroducing such activities as the shoulder strength and function improve, could potentially yield more positive results in improving the ability to perform work activities. However, this is rather impractical as the teachers had to continue with their normal teaching routine.
The shoulder rating questionnaire showed an improvement in global assessment, improved ability to perform daily activities, and improved satisfaction with the shoulder in the experimental group following the intervention, with a large effect. This improvement could also be attributed to the intervention programme, due to improved strength and improved shoulder internal rotation. Furthermore, pre-intervention participants had been predominantly concerned with improving their pain. However, the number of participants concerned with decreasing their pain significantly decreased (
No significant difference in scapular position difference between the control and the experimental groups. Both the control and experimental groups presented with a scapular position difference of less than 1.5 cm. A 1.5 cm asymmetry between left and right is regarded as the threshold for abnormality in the scapular position [22], which means than if the scapular difference is 1.5 cm or more, there could be scapular dyskinesis, which Kibler and McMullen associate with shoulder pain [22]. The results of this current study could therefore indicate that there was no abnormality in the scapular positions for either the control or experimental groups. However, on the other hand, it was noted that a threshold of 1.5 cm for shoulder asymmetry may not be accurate in determining altered scapular position and requires further examination [21], which could also support the current study which shows no abnormality in spite of shoulder pain reported.
The overall intervention programme was effective in reducing pain, improving shoulder function, internal rotation range of motion and muscle strength among teachers. The algorithm for the development of the intervention programme (Fig. 4) was based on the assessments conducted with the teachers and also considering the limited amount of time the teachers had to participate in the study due to the busy school schedule. The concept was to design a simple yet scientific and effective programme that is not time consuming, in order for the teachers to be able to adhere to and benefit from. The assessment for impingement symptoms was conducted by performing Neer’s and Hawkin’s tests, which are the most widely used tests [37, 38], with Hawkin’s test being the most accurate [38, 39]. The apprehension test was used to measure anterior instability. Participants with history of shoulder surgery, macro-trauma to the shoulder, dislocation and signs of inflammation were excluded. The reason for that was to avoid aggravating the shoulder pain, while still accommodating a range of other shoulder conditions to the programme. The excluded conditions would require further thorough examination and more specific individualised rehabilitation. Participants presented with lack of range of motion of the shoulder and reduced muscle strength, of which range of motion and strength exercises were incorporated in the programme to address this. The rotator cuff muscles are most prone in overuse activities and yet serve an important function of stabilising the shoulder. Therefore strengthening this muscles was the area of focus although the programme was not entirely limited to it.
Conclusion
This study provides a rationale to implement such programmes for teachers, as they present with a high prevalence of shoulder musculoskeletal disorder. Schools should consider applying the programme where teachers can be trained to perform the exercises to do them at home, as they can be simple to complete following appropriate training. Future research should also focus on improving work activities, as well as educating teachers on the ergonomics to minimise shoulder musculoskeletal disorders.
Limitations
The sample size for the study was small. A larger sample size is required to reduce error risk and improve accuracy. There was no randomisation between the control and the experimental groups. The experimental group was selected from one school and the control group from another school. Therefore the study did not balance the groups for prognostic variables and selection bias was not eliminated. Furthermore, the control and experimental groups might not have been exposed to the same conditions outside of the study, which could also affect the results. It is worth noting that the shoulder pain was self-reported by the teachers rather than being diagnosed by a healthcare professional, which could result in results being bias. Furthermore, no follow-up was conducted after the intervention period to assess how long the positive effects of the intervention programme last after the eight-week intervention. The benefits of the programme could only be short-term.
Footnotes
Acknowledgments
The authors wish to thank the primary school teachers from the Kranskloof circuit for participating in this study. The authors also acknowledge the National Research Foundation (NRF) for funding the study.
Conflict of interest
None to report.