
Abstract
BACKGROUND:
Most studies use platelet-rich plasma (PRP) requiring multiple intraarticular injections for knee osteoarthritis (OA).
OBJECTIVE:
To investigate the efficacy of a single intraarticular PRP injection for patients with early knee OA and consider subgroup analyses of radiographic severity and age, respectively.
METHODS:
Forty-one patients with knee OA (Kellgren-Lawrence grade 1–2) received a single PRP injection into the target knee and were assessed at baseline and 1, 3, and 6 months postinjection. The primary outcome was the mean change from baseline in the visual analog scale (VAS) pain (0–100 mm) at 6 months postinjection. Secondary outcomes included the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Lequesne index, single leg stance test (SLS), use of rescue analgesics and patients’ satisfaction.
RESULTS:
Thirty-eight patients completed the study. The mean pain VAS decreased significantly from 45.6
CONCLUSIONS:
One injection of PRP improved pain and function for 6 months for patients with early knee OA. This study supports putting the one-injection regimen into clinical practice. Further research is needed for more definite conclusions.
Introduction
Knee osteoarthritis (OA) is a common condition that causes pain and disability. The treatment for knee OA aim to reduce pain, stiffness, and physical disability. Current treatment options include the use of simple analgesics or nonsteroidal anti-inflammatory drugs (NSAIDs), glucosamine and chondroitine sulphate, intra-articular injection of corticosteroid, hyaluronic acid and platelet-rich plasma (PRP), physical therapy, weight reduction, orthotics and surgical treatment ranging from arthroscopy to total knee replacement [1]. Due to the chronicity and incurable nature of knee OA, therapies targeting knee OA should be safe and effective for its long term management. In recent years, treatment options such as biological and regenerative methods have come into vogue.
PRP is an autologous blood product that mainly contains concentrated platelets and growth factors. The growth factors serve to promote local angiogenesis, modulate inflammation, inhibit catabolic enzymes and cytokines, recruit local stem cells and fibroblasts to sites of damage, and induce healthy nearby cells to manufacture greater numbers of growth factors [2]. Local use of PRP directly at the site of cartilage injury is thought to stimulate a natural healing cascade and accelerate cartilage repair [3, 4, 5, 6].
PRP had been reported to be an effective and safe orthobiologic in the treatment of knee OA [7, 8, 9, 10]. However, there is no clarity in reference to the number and frequency of PRP injections. A range of single to multiple injections with weekly to every 3- or 4-week schedule had been reported [11, 12]. To date, there were only few studies reporting the efficacy of a single PRP injection for the treatment of knee OA [12, 13, 14, 15, 16]. Patel et al. reported that a single PRP injection is as effective as two injections in early knee OA [12]. The single injection regimen may represent an attractive alternative, as it may decrease patient time expenditure and discomfort associated with the injection process and offer potential safety benefits to patients. Besides, the one injection regimen may possibly represent a cost-saving therapy compared with multiple injections.
Intraarticular PRP has been reported to have better results in younger patients, low body mass index patients and those with less degree of cartilage degeneration [8, 17]. However, the predictors of good response for one injection of PRP have seldom been reported [12, 13, 14]. It is important to determine the type of patients who will benefit from the therapy in order to guide its clinical use and avoid an indiscriminate clinical application. The purpose of this study was to investigate the efficacy and safety of a single injection of PRP for the treatment of early knee OA. Subgroup analyses would be done to determine whether radiographic severity or age would influence the treatment effects.
Materials and methods
Ethical approval
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board for Human Investigation of Kaohsiung Veterans General Hospital. The trial was registered at ClinicalTrials.gov (Registry number NCT04027738). All subjects provided written informed consent prior to enrollment in the study.
Study design and participants
This was a prospective study with a 6-month follow-up period done in the setting of an outpatient rehabilitation department in a tertiary care medical center between January 2017 and December 2017.
The inclusion criteria were: patients aged 20–70 years, symptomatic knee OA with pain for at least 6 months despite conservative treatment such as analgesics, NSAIDs and/or physical therapy, average knee pain of at least 30 mm on a 100-mm visual analog (VAS) scale, grade 1 or 2 knee OA according to the Kellgren-Lawrence grading system based on standing anterior-posterior and lateral knee radiographs taken within the previous 6 months [18]. Radiological evidence of bilateral knee OA was accepted if global pain VAS in the contralateral knee was less than 30 mm.
Exclusion criteria were: previous orthopedic surgery on the spine or lower limbs; disabling OA of either hip or foot; knee instability or marked valgus/varus deformity; history of severe knee trauma; intraarticular injections into the knee in the past 6 months; infections or skin diseases around the target knee; women ascertained or suspected pregnancy or lactating; presence of malignancy, hematological disease, collagen vascular diseases, or autoimmune diseases; therapy with anticoagulants or anti-aggregating agent; or serious medical conditions that would interfere with assessments during the study.
Major protocol violations included surgery, initiation of physical therapy, and use of proscribed medications. Patients were said to be noncompliant when they missed any patient visit.
Study process
The study consisted of a screen visit, a baseline visit during which intraarticular injection was done and follow-up visits at 1, 3 and 6 months after the injection. Potential study participants returned for a baseline visit after a 1-week washout period for NSAIDs and analgesics. Before injection, demographic data and baseline assessments were collected.
Intervention
The patients received a single 3-ml injection of PRP. Approximately 10-mL of venous blood was drawn from each patient and centrifuged using an Arthrex autologous conditioned plasma (ACP) kit (a low-leukocyte ACP system), spun at a speed of 1500 rpm for 5 minutes. The platelet concentration obtained was approximately 2–3 times greater than the baseline platelet concentration.
All the injections were done by the same experienced physician using aseptic procedures. All injection procedures were carried out using 23 gauge needles based on anatomic landmarks. With the patient in a sitting position and the knee flexed to 90
None of the patients received physical therapy after the injection. No regular analgesics, glucosamine or chondroitin, NSAIDs or physical therapy for knee were permitted during the study. Acetaminophen (500 mg; maximum daily dose, 4 g) was the only rescue medication allowed for knee pain. Acetaminophen was not permitted during the 24-hour period prior to each study visit. Use of rescue medication during the study period was recorded in a patient diary.
Outcome measures
The primary outcome was the change from baseline in the VAS pain score at 6 months. The patient rated the average severity of knee pain on knee movement over the previous week on a 0–100 mm VAS (0
Secondary outcome measures included the following:
The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC, Likert Scale) is a 24-item questionnaire with 3 subscales measuring pain, stiffness, and physical function [20]. The patient answers the questions and then receives a cumulative score in each of the 3 areas (pain, 0–20; stiffness, 0–8; physical function, 0–68). Total score is 96 and higher scores indicate worse outcomes.
Lequesne index was used to assess severity of knee symptoms during the last week [21]. It includes the measurement of pain, walking distance, and activities of daily living. Maximal score is 24 and higher scores represent worse function.
Single-leg stance test (SLS) is done by raising one foot up without touching it to the supported lower extremity with target knee and maintain balance for as long as possible. Each participant performed 3 trials, and the best result of the 3 trials was recorded [22].
These variables were measured at baseline (before intervention), 1, 3 and 6 months after injections by a physician not involved in PRP injection. Patients were asked to rate their treatment satisfaction compared to the preinjection condition, using a 100 mm VAS (0
The occurrence of adverse events was recorded, including duration, action taken and outcome.
Statistical analysis
Based on the G*Power 3.0 and the statistical method used for the study purpose, Wilcoxon signed-rank test, the required sample size was 35 participants (power
We used the Statistical Package for the Social Sciences (version 20.0; SPSS Inc, Chicago, IL, USA) for all analyses. Changes in outcome measures among baseline, 1, 3, and 6-month postinjection were assessed using Friedman tests and Wilcoxon signed-rank tests as post hoc analyses with Bonferroni’s corrections. A
Subgroup analysis
After data collection was complete, we divided patients by radiographic severity and age and subgroup analyses were done to compare the outcome scores at various time points to determine whether radiographic severity or age would influence the treatment response. Between-subgroup differences were assessed using Mann-Whitney U tests for satisfaction and for improvement (i.e. each follow-up comparing with baseline) of other outcome measures. Within-subgroup differences were assessed using Friedman tests and Wilcoxon signed-rank tests as post hoc analyses with Bonferroni’s corrections. A
Results
Patient characteristics
Forty-six participants were assessed for eligibility, of whom 5 were excluded, and 41 participants were enrolled for intervention (Fig. 1). Three patients withdrew during the study period, leaving 38 patients available for the analysis at 6-month follow-up. The demographic and clinical characteristics of the study participants are shown in Table 1. Patients were predominantly female (65.8%), the mean age was approximately 57.9 years (range 31–70 years), the mean body mass index was 24.5 kg/m
Demographic and baseline characteristics of the participants
Demographic and baseline characteristics of the participants
The values are given as mean
Flow diagram of participants through the trial.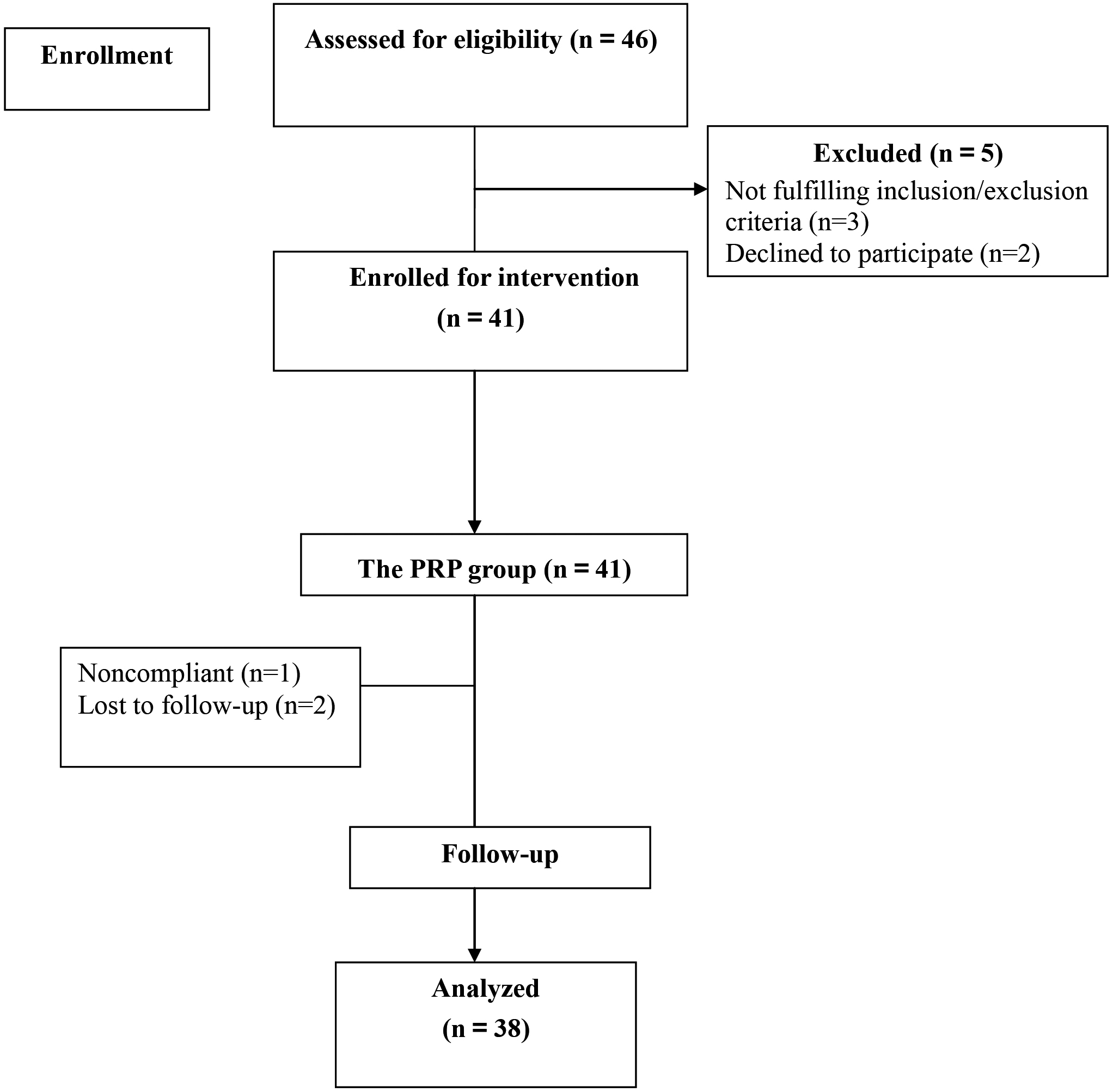
Patients showed significant VAS pain change among four time points from baseline to three follow-ups after a single PRP injection using a Friedman test (
The outcome measures before and after treatment
The outcome measures before and after treatment
The values are given as mean
WOMAC (including 3 subscale scores and total scores) changed significantly among four time points from baseline to 1, 3, and 6 months after injections (
Patients improved significantly in Lequesne index and SLS scores from baseline to each follow-up visit, respectively (all
In this study, there were 15 patients with Kellgren-Lawrence grade 1 OA and 23 patients with grade 2 OA. At baseline, the grade 2 group showed greater WOMAC function subscale scores and total scores, and Lequesne index scores (
Comparison between different OA Kellgren-Lawrence grade
Comparison between different OA Kellgren-Lawrence grade
The values are given as mean
Comparison between different age populations
The values are given as mean
When patients were divided by age, some interesting findings emerged. Using 60 years of age as the cutting point, patients were classified into the younger age-group (age
No infections, allergic reactions, or other serious adverse events occurred during the study. Five (13.2%) patients developed minor adverse events after PRP injections. These adverse events were mild and transient, and self-resolved in 2 days without any therapeutic intervention. No patients withdrew from the study because of any adverse event.
Discussion
This study demonstrated that one injection of PRP was safe and effective for 6 months in the treatment of Kellgren-Lawrence grade 1 or 2 knee OA. The one injection regimen of PRP reduced pain, improved function and resulted in high patient satisfaction. Patients with grade 1 OA showed significantly greater improvement in VAS pain at 3 and 6 months than patients with grade 2 OA. Patients aged over 60 years showed significantly greater reduction in VAS pain, WOMAC function subscale and total scores at 6 month postinjection compared with patients aged 60 years or younger. Patients aged 60 years or younger reported greater satisfaction at 1 and 3 months than patients aged over 60 years.
Pain reduction is the primary indication for the use of intra-articular knee injection. In clinical trials of chronic pain treatments, reduction in chronic pain intensity of at least 30% appeared to reflect at least moderate clinically important differences [23]. In our study, the mean VAS pain score reduced by 28.7 mm (62.9%), 31.6 mm (69.3%), and 30.1 mm (66.0%) at 1, 3, and 6-months postinjection, respectively. It appeared that pain reduction was documented in our study and the magnitude of pain reductions were far beyond clinical meaningful significance. Li et al. investigated the efficacy of single injection of PRP for Kellgren-Lawrence grade 1 or 2 knee OA. The median VAS score improved from 64.2 mm at baseline to 42.8 mm at 6-months follow-up, corresponding to a median reduction of 33.3% from baseline [13]. Interestingly, greater VAS pain reduction (66.0%) at 6-months postinjection was noted in our study population.
The patients experienced significant improvements in all WOMAC subscale and total scores through the 6-month follow-up, supporting the efficacy of PRP injections in relieving pain and stiffness for patients with knee OA. The minimum clinically important differences (MCID) for changes in WOMAC pain and function scores was set at 20% [24]. Patients in our study experienced a 51.4% improvement in WOMAC-pain and a 48.8% improvement in WOMAC-function from baseline at 6-month postinjection, much exceeded the MCID. Patel et al. reported a mean WOMAC-pain reduction of 50.9% from baseline at 6 months after a single injection of PRP in grade 1 or 2 knee OA, which was very similar to our results [12]. Sánchez et al. compared PRP and hyaluronic acid in patients with knee OA, and they also reported that treatment with PRP reduced the WOMAC index by 50% [25].
Lequesne defined effective treatment forms as those leading to a score improvement of 30–40% at the time of follow-up [26]. In our study, the mean Lequesne index scores improved by 3.7 points from baseline at 6-month post PRP injection, representing an improvement of 48.7%, which was beyond the values used to define treatment effectiveness.
There is limited evidence supporting the use of a single PRP injection for the treatment of early stage knee OA [12, 13, 14, 15, 16]. Patel et al. reported that a single intraarticular PRP in concentrations of 10 times the normal amount is as effective as 2 injections to alleviate symptoms in early knee OA [12]. Similar to our results, they reported that patients with grade 1 OA showed better results than those with grade 2 [12]. Different from their study, the PRP concentration in our present study was approximately 2–3 times greater than baseline platelet concentration. Interestingly, we found that patients aged over 60 years showed significantly greater reduction in VAS pain at 6-month postinjection compared with those aged 60 years or younger, as at baseline patients in the older-age group were more painful than those in the younger-age group. Li et al. reported a case series with 21 patients and they concluded that one injection of PRP seems to be effective in patients with low-grade knee OA [13]. Compared with their case series, we had larger sample size and we used more subjective and objective outcome measures. Buendía-López et al. reported that a single intraarticular PRP resulted in pain reduction and function improvement in patients with early knee OA at the 52-week follow-up, superior to a single injection of hyaluronic acid and the use of oral NSAID [14]. Kesiktas et al. recently reported that a single intraarticular PRP, hyaluronic acid, or peptide injection provided satisfactory results in terms of pain and function in knee OA at 3 months [27]. Although various studies reported the efficacy of one injection of PRP for knee OA, direct comparison among these studies was not possible because of different study population, different PRP preparation method and different outcome measures.
This study utilized the low-leukocyte ACP system (Arthre, Germany) based on increasing evidence that it is the ratio of platelets to leukocytes and not only the number of platelets that determines the biological activity of a PRP-type product [28].
Evaluation of the efficacy for one-injection regimen of PRP in the Asian population was also a major concern of this study, as most previous studies with a single injection regimen were conducted with Caucasian or mixed populations [12, 13, 14, 15, 16]. The findings are not necessarily applicable to the Asia population, as recent studies have claimed that platelet function differs with ethnicity [29, 30]. We choose to use a single injection regimen because there is evidence of no significant differences between a single dose and multiple doses, suggesting the possibility to avoid multiple injections protocols, and consequently reducing the health expenses in terms of cost-efficacy.
Patient satisfaction is a fundamental goal in the treatment of OA patients and it reflects the summation of all factors relating to successful clinical treatment. Results of patients’ global satisfaction showed that most patients were satisfied with the treatment. Interestingly, we found that patients aged 60 years or younger reported greater satisfaction at 1 and 3 months postinjection than patients aged over 60 years. No patients reported dissatisfaction or aggravations of the symptoms throughout the study period.
In this study, all adverse events were mild and self-limiting. The absence of serious adverse events, noted in previous studies and in the present trial, suggests that PRP represents a safe treatment option for patients with knee OA.
There were several limitations in this study. First, this was a single center study and we recruited patients with Kellgren-Lawrence grade 1 and 2 tibiofemoral OA only. The result can not be generalized to all the OA populations with different radiographic severity. Second, the sample size was small and the follow-up time was short. Additional studies with larger sample size and longer follow-up period would be needed to confirm the long-term efficacy. Third, because of budget limit, we did not have a control group. There is a strong placebo effect from joint injections, which may cause a nearly 30% pain reduction during the first few weeks [31]. Thus, we may possibly miss the placebo effects and overestimate the real effects of PRP. However, because the placebo effect would mostly be seen in the early periods, the late findings of this study at 3 and 6 months may reflect reliable results for PRP injections. Further research including a sham control, corticosteroid injection, or hyaluronic acid injection is of great interest. The optimal number and frequency of injections, the potential use in joints other than the knees, as well as the role for repeated series of injections must be clarified in the future.
Conclusions
This study showed that a single injection of PRP was effective and safe for patients with Kellgren-Lawrence grade 1 or 2 knee OA. Subgroup analyses revealed that patients with grade 1 OA showed significantly greater VAS pain reduction at 3 and 6 months than patients with grade 2 OA. The older-age group (age
Author contributions
SFS was the principal investigator of the study and responsible for the trial operation, study design, knee injections and completion of the manuscript. IHL was responsible for the study design, evaluations, and writing-up the manuscript. YCC, SYW and HYH contributed to the conception and study design, project administration, data interpretation and writing up the manuscript. CWH and HSL were responsible for sample size calculation, statistical analysis and data interpretation. All authors have read and agreed to the published version of the manuscript.
Funding
SFS received an academic research fund for Kaohsiung Veterans General Hospital (no. VGHKS106-131).
Footnotes
Acknowledgments
We wish to express our sincere gratitude to all the investigators and patients who participated in the trial.
Conflict of interest
The authors report no conflicts of interest.