
Abstract
BACKGROUND:
Hamstring flexibility plays a significant role in physiotherapy. Various stretching studies have been conducted to increase hamstring flexibility, but the effects of the Fascial Distortion Model (FDM) on hamstring flexibility have not yet been investigated. Moreover, no studies have compared the effects of FDM and static stretching.
OBJECTIVES:
To investigate the effects of the FDM on hamstring flexibility compared with static stretching.
METHODS:
Thirthy healthy adults were divided into two groups: static stretching and FDM groups. Static stretching was performed to hamstring in the supine position. The FDM was performed using trigger band techniques that followed the hamstring in a longitudinal direction. Hamstring flexibility was measured using the active knee extension angle (KEA), passive straight leg raising (SLR), sit-and-reach (SR), and finger-floor distance (FFD) tests. A paired
RESULTS:
Both groups showed significant differences (
CONCLUSIONS:
There was no difference in the effects of FDM and static stretching on hamstring flexibility.
Introduction
Flexibility is the ability to move a single joint or a series of joints smoothly and easily and can have a significant role in muscle function [1]. Flexibility can improve the results of various types of activities such as stretching, hot shower bathing, massages, and heating modalities [1, 2].
Stretching is a form of physical exercise in which a specific muscle or tendon is deliberately flexed or stretched [3]. It is commonly used in the general population and sport and clinical contexts to improve muscle control flexibility and range of motion (ROM) [3, 4] or reduce injury and improve the performance in sports and overall physical fitness [5]. Various types of stretching exercises include static and dynamic, ballistic, and proprioceptive neuromuscular facilitation stretching [1, 6]. Static stretching in particular is the best and highly preferred stretching method [6] because it is believed to be the safest and has the least associated injury risk [5].
The new techniques of manipulative diagnosis and treatment used in the fascial distortion model (FDM) have become increasingly popular among manual and physical therapists [7]. This model was developed and established by the American osteopath Stephen Typaldos, D.O. (1957–2006) [8, 9]. The model is based on an anatomical model on the concept of the fascia as sensitive and pain permitting organs [8, 9]. The FDM is rooted in the hypothesis that all musculoskeletal complaints can be traced back to three-dimensional deformation or distortion of a specific connective-tissue structure [7]. The main principle of the FDM is to reflect the main focus being on the body language with which patients communicate their complaints and medical history to be of central importance [7, 8]. In particular, the patient’s body language is observed to make a diagnosis, choosing one from the six classes that the FDM comprises: trigger bands, herniated trigger points, tectonic fixations, and continuum, folding, and cylinder distortions [7, 9]. The diagnosis describes the concept of how the fascia is twisted at a particular body part where they cause specific problems [9]. Therefore, the patients participate in the supervision of their own treatment [8]. Through the FDM, physicians can apply a manual technique to rapidly and effectively increase ROM and decrease pain [10].
The flexibility of the hamstring muscles plays a substantial role in the prevention of injury and muscular imbalance, maintenance of a full range of joint movement, optimal musculoskeletal function, and enhanced performance in sports [5]. The hamstrings are not used on a regular basis, so both athletes and non-athletes are not well noticed if they are short [5, 11]. Moreover, they are well known for their great tendency to shortening [2]. Insufficient hamstring flexibility is associated with adverse alterations in lower limb kinematics [11]. The lack of hamstring extensibility creates various musculoskeletal injuries such as a decrease in pelvic mobility and increase in biomechanical changes in the pressure distribution of the spine, leading to lower back pain [2, 11, 12]. Therefore, hamstring stretching is one of the useful clinical exercises for increasing the ROM and muscle flexibility, improving muscle balance, and preventing the muscle from injury [5, 13]. Moreover, hamstring flexibility becomes a significant matter in the context of physiotherapy [2].
Various stretching studies have been conducted to increase hamstring flexibility, but the effects of FDM on hamstring flexibility have not yet been investigated. Moreover, no studies have compared the effects of FDM and static stretching. Therefore, we aimed to investigate the effects of FDM on hamstring flexibility compared with static stretching.
Materials and methods
A total of 30 healthy adults participated in this study and were divided into two groups: static stretching group (SG) and FDM group (FG). The age range of subjects was 21–24 years because all voluntary participants were university students; the mean age of 22.17
The required sample size was calculated using an 80% statistical power to detect a 30% difference in the two groups. N
The inclusion criteria of the study were willingness to participate in the trial, bilateral normal (120
All subjects were informed about and understood the details of the research procedure and provided signed informed consent prior to participation. The present study was conducted in a single-blind fashion; thus, the subjects did not realize the purpose of the experiment. This study complied with the ethical standards of the Declaration of Helsinki and was conducted after approval from the Institutional Review Board from Kyungnam University was obtained (approval number 1040460-A-2019-012).
Before the procedures, each subject was asked to be present in the laboratory to inform them about the experiment. In static stretching exercise for the hamstrings, the subjects lay supine on the floor, and their hip was flexed with the knee in an extended position by placing the leg of the subject on the therapist’s shoulder as in the SLR test and the ankle in a neutral position [1, 4, 5]. For an effective stretch, the pelvis and opposite leg remained on the floor with the knee extended. Static stretching was performed three times with no pain, with a range of discomfort of mild discomfort, and keeping for 30 s and resting for 15 s between stretching repetitions. The session lasted for approximately 10 min. For the application of the FDM, the subjects were asked to indicate the location of pain using the FDM according to Typaldos during the SLR test [9]. The FDM was initiated using trigger band techniques that followed the hamstring in a longitudinal direction from the medial knee joint or lateral hollow of the knee to the ischial tuberosity [14]. Mainly, strong local pressure was applied on the painful points using the thumb and reduced when the patient reported [9]. These procedures were repeated until pain was no longer reported. The number of repetitions varied according to the subjects’ condition, and the average was three to four times. The session lasted for approximately 3–4 min. No other form of treatment was performed.
Hamstring flexibility was measured using the active KEA, passive SLR, sit and reach (SR) and finger floor distance (FFD) tests. To measure KEA, the subjects were instructed to lie in a supine position with their hip and knee flexed to 90
All measurements were repeated three times before and after static stretching and FDM, and the average score was calculated. No warm-up or stretching was performed before the measurements. SPSS software was used to examine the hamstring flexibility. The normal distribution of data before analysis was checked using the Shapiro-Wilk test, and the collected data met the normality assumption (
Results
The table presents the mean values and SDs (Standard Deviations) for the hamstring flexibility measurements before and after static stretching and FDM. Both groups showed significant differences (
Comparison of hamstring flexibility measurements before and after static stretching and fascial distortion model in each group
Comparison of hamstring flexibility measurements before and after static stretching and fascial distortion model in each group
Comparison of hamstring flexibility measurements between the two groups
Values are presented as means
Comparison of hamstring flexibility measurements. SG, static stretching group; FG, FDM group; KEA, knee extension angle; SLR, straight leg raising; SR, sit and reach; FFD, finger floor distance.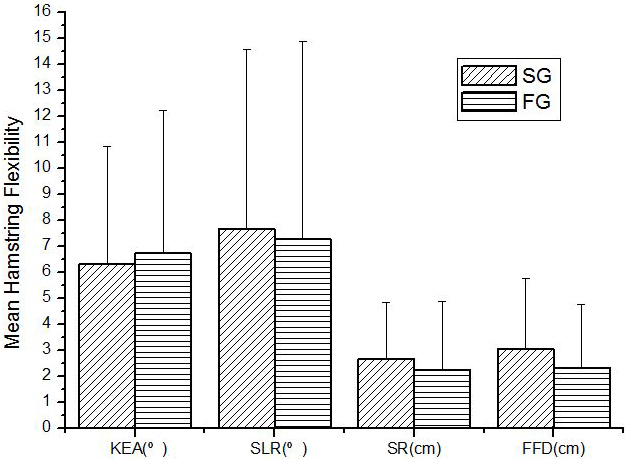
However, no significant difference(
To dtae, no study has demonstrated the change in hamstring flexibility using the FDM. To the best of our knowledge, this is the first to compare the effects of static stretching and FDM. In our study, hamstring flexibility showed significant differences; all values increased after static stretching and FDM compared with those prior to the procedures (
Several studies showed that static stretching is very effective in increasing muscle flexibility and hamstring length [12, 17]. Manickam et al. [5] showed that there was a significant reduction in hamstring tightness of followed by active self-stretching using the 90–90 test. Moreover, Marques et al. [16] showed that static stretching was effective in reducing hamstring stiffness and suggested that stretching three times a week is sufficient to improve flexibility compared with stretching at a higher frequency. In the study by Bandy and Irion [18], they reported increased knee extension ROM with static stretching and Page [19] showed the greatest change in ROM with a static stretch. Moreover, Weijer et al. [20] suggested that a significant increase in hamstring length can be maintained for up to 24 h when performing static stretching. These results are consistent with our findings. Regarding these results, it is well known that gains in flexibility involve biomechanical, neurological and molecular mechanisms [16]. Sundaram and Arun [1] suggested that the short time of increased hamstring flexibility is due to the viscoelasticity, thixotropicity, and neural properties of the muscle-tendon unit. Marques et al. and Demoulin et al. [4, 16] suggested that it can be associated with increased tolerance to pain and decreased neural input to the motor neuron pool. Moreover, Medeiros et al. [2] and Savelberg and Meijer [21] proposed that there is a great possibility of increasing the number of sarcomeres in series and blood supply in the joints and muscles that enhances muscular extensibility and flexibility may produce autogenic inhibition of the stretched muscle.
Several studies showed that the FDM treatment is very effective in ROM and pain management [9, 22, 23, 24]. Boucher and Figueroa [22] reported that the shoulder was restored to full abduction and internal rotation without pain, and Schulze et al. [9] showed that the FDM was an effective method for the acute treatment of medial tibial stress syndrome. Park and Kim [24] reported an increase in the range of motion of ankle dorsiflexion compared to foam rolling and self-stretching.
However, the evidence about the FDM remains unclear. According to Dr. Typaldos, who developed the FDM, shortening caused by fascial distortion causes a movement restriction of the affected area. As a result, most patients complain of pulling discomfort, called trigger bands, and the therapist follows the exact same line with one’s thumb [14]. During the FDM, patients could experience a significant discomfort and pain, but a powerful counter stimulation activates the gate-control mechanisms [8]. Schulze et al. [9] suggested that after FDM treatment, pain sensation could be quickly achieved and substantial relief afterward, improved regarding function. The extracellular matrix composed of 70% water is a major component of fascia, which can causes thixotropy [25]. Richter et al. [8] assumed that the strong pressure through FDM affected on the fibroblast activity consequently and alterations of the extracellular connective-tissue matrix. We assumed that the immediate increase in the range of motion was the result of changing the viscosity of fascia from solid to liquid. In comparison with conventional physiotherapy, the FDM method seems to be clearly superior and is potentially effective for acute treatment [9]. Maśliński and Woldańska Okońska [23] suggested that the techniques of the FDM are an interesting complement workshop therapy that is treating limits in the ROM and pain in the joints. Although there is not enough evidence compared with static stretching, our results also support the previous suggestions. Despite the short application time of the FDM compared with static stretching, no difference in the effect on flexibility was noted (
This study examined the effects of FDM on hamstring flexibility compared with static stretching. The finding showed that FDM provided in a shorter period of time than static stretching induced similar changes in flexibility as static stretching. It appears that FDM application can increase the patients’ motivation by restoring function within a short period of time.
There were some limitations in this study. First, the most notable limitation was the small sample size, which could negatively impact statistical conclusions. Second, as the sample was collected from only 30 participants, a larger study with a full sample size calculated through a power analysis should follow this study to ensure the consistency. Third, since the age range of the participants was narrow and they were not clinical patients, the findings of this study are not conclusive in generalizing until a clinical trial is conducted.
Footnotes
Conflict of interest
None to report.