
Abstract
BACKGROUND:
Patients with chronic low back pain (LBP) have an impaired dynamic spinal stability, which may lead to arm injuries.
OBJECTIVES:
To examine the latissimus dorsi and gluteus maximus muscles activation pattern and the upward scapular rotation in patients with chronic LBP.
METHODS:
Sixty-one right-handed males were divided into two groups: chronic LBP group (
RESULTS:
The LBP group has a bilateral significant increased EMG of latissimus dorsi (
CONCLUSION:
Chronic LBP increased the latissimus dorsi muscle activities and decreased the gluteus maximus activities. It furthermore increased the upward scapular rotation in different shoulder abduction positions.
Introduction
Nonspecific chronic low back pain (LBP) is one of the most prevalent musculoskeletal problems affecting most ages and genders. Most patients have chronic pain that lasts more than three months, limiting their activities and forcing them to miss work [1]. Chronic LBP is expressed as LBP not related to an exact disease such as inflammatory disorder, osteoporosis, fracture, structural deformity, radicular syndrome, cauda equina syndrome, or a tumor [2].
One of the common causes of chronic LBP is the trunk and hip muscles strength and length imbalance [3]. Various factors associated with chronic LBP, such as changes in motor control and muscular recruitment have been the primary concern of chronic LBP treatments within the past decade [4, 5]. Patients with chronic LBP experienced irregular adaptations that resulted in movement and control impairments, leading to either excessive or impaired dynamic spinal stabilization and loading, which causes pain [6]. The muscles and joints of the lumbopelvic region provide proximal stability to allow optimum force production and transmission for distal mobility of extremities through a kinetic chain. Thus, insufficient support of the trunk and lower extremities may affect arm injuries through breakage in the kinetic chain [7, 8].
The muscle chains are connected through myofascial slings, which maintain trunk stability and force transmission from the lower to the upper limbs during movement [9]. Muscle imbalance and pain produced due to sling muscle injury will irritate the trigger points. The posterior oblique myofascial sling, composed of the erector spinae latissimus dorsi, gluteus maximus, and hamstring muscles plays a critical role in trunk extension [9, 10, 11]. Moreover, the latissimus dorsi muscle acts as a synergist to the gluteus maximus muscle through the thoracolumbar fascia [12].
During the prone hip extension (PHE) test patients with chronic LBP had greater muscular activation of latissimus dorsi muscle [9]. When the control gluteus maximus to the lumbopelvic area is decreased, the contralateral latissimus dorsi muscle may be activated to compensate for gluteus maximus insufficiency and spinal instability [9, 12]. Furthermore, there is more significant pelvic motion and less lumbar motion during forward bending. Moreover, there is bilateral reduction in the gluteus maximus muscle and a significant association between ipsilateral erector spinae muscle function and lumbar activity in patients with chronic LBP [13].
Scapular dyskinesia is related to the increased latissimus dorsi stiffness. The latissimus dorsi stiffness increases the upward scapular rotation and posterior tilt; however, scapular internal scapular rotation decreased during humeral elevation [14]. Since the latissimus dorsi is attached to the inferior border of the scapula, its stiffness affects scapular motion [9]. Moreover, Taghizadeh et al. [15] found an increasing scapular rotation in a patient with chronic LBP at the neutral position and shoulder at 40–45
The relationship between scapular position and electromyography (EMG) of lumbopelvic muscles, especially the latissimus dorsi and gluteus maximus, must be identified. Therefore, this study was set to examine the latissimus dorsi and gluteus maximus muscles activation pattern and upward scapular rotation in male patients with chronic LBP. It has been hypothesized that there was no effect of chronic LBP on scapular positions and EMG of latissimus dorsi and gluteus maximus muscles of the right and left side.
Materials and methods
Participants
A total of 61 right-handed male participants (mean age 22.47
The participants were divided into two groups: those with chronic LBP (LBP group,
The participants’ flowchart.
The study followed the principles of the Declaration of Helsinki and each participant signed an informed consent form. The ethical committee of the Faculty of Physical Therapy, Cairo University approved the current research work (No. P.T. REC/012/002035).
Before baseline measurements, the subjects were given a full explanation of the study protocol, scapular movement, and contraction of latissimus dorsi and gluteus maximus muscles. Then, the subjects were asked to perform each movement.
Electromyography recording
The EMG surface device (MyoTrac Infiniti, model SA9800, Canada) was a modular EMG data collection system. The system offers dual channels to assess the ipsilateral gluteus maximus and contralateral latissimus dorsi muscles EMG during the PHE test for both sides [19].
The PHE test is a widely used and recognized method of determining lumbopelvic stability and the muscle recruitment pattern of the posterior oblique sling muscles in chronic LBP patients. Muscle activity pattern during PHE test has been theorized to be similar to those muscles activated during gait and changes in this pattern may decrease lumbopelvic stability during walking [6, 9, 16, 22].
Before placement of the electrodes, the skin was cleaned with isopropyl alcohol 70% to remove excess oils and debris, and shaved (if required). The active and reference electrodes were stuck in the muscle belly parallel to muscle fibers and away from the tendon and muscle edges. The ground electrode was placed on any bony prominence distal to the other electrodes [19].
For the latissimus dorsi muscle, the active electrode was stuck 4 cm below the inferior angle of the scapula, mid the distance between the vertebral column and the lateral edge of the torso. The reference electrode was mounted next to the active electrode, parallel to the muscle fibers, and at a distance equal to the electrode scale. The ground electrode was placed distally on the acromion process (Fig. 2A) [9].
A. Electrodes placement for EMG of latissimus dorsi muscle. B. Electrodes placement for EMG of gluteus maximus muscle.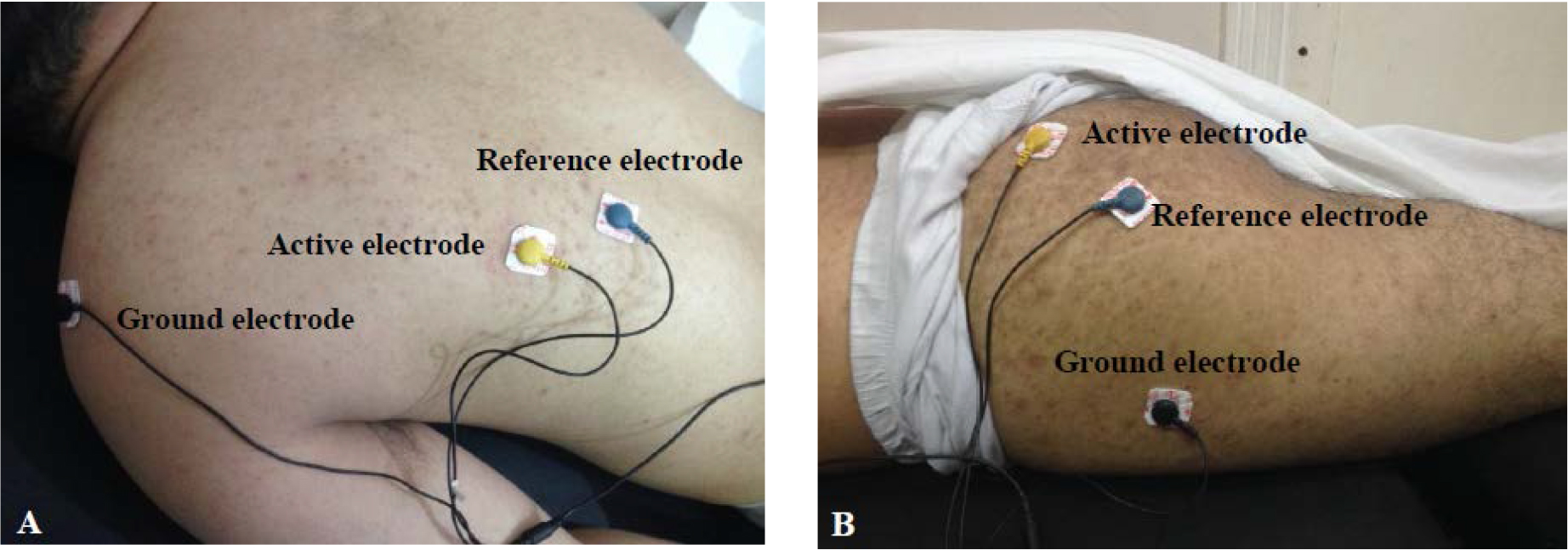
For the gluteus maximus muscle, the active electrode was stuck in mid-distance between the greater trochanter and 2
All participants were informed about the PHE test procedure before testing. The EMG measurements were conducted while the participants lay prone on a plinth with a firm mattress. The participants lay prone with their arms beside their trunk, and maintained their pelvis and hip joint in neutral positions. A universal goniometer was used to set the degree of hip extension at 10
Prone hip extension test.
The participants were instructed to keep the knee extended and extend their hip from the neutral to 10
The maximum voluntary isometric contraction (MVIC) method was used to normalize the RMS value of the latissimus dorsi muscle. The participants lay in a prone position with the upper extremity suspended on the plinth side and were asked to flex their elbow to 90
A. Normalization of the RMS values of latissimus dorsi muscle. B. Normalization of the RMS values of gluteus maximus muscle.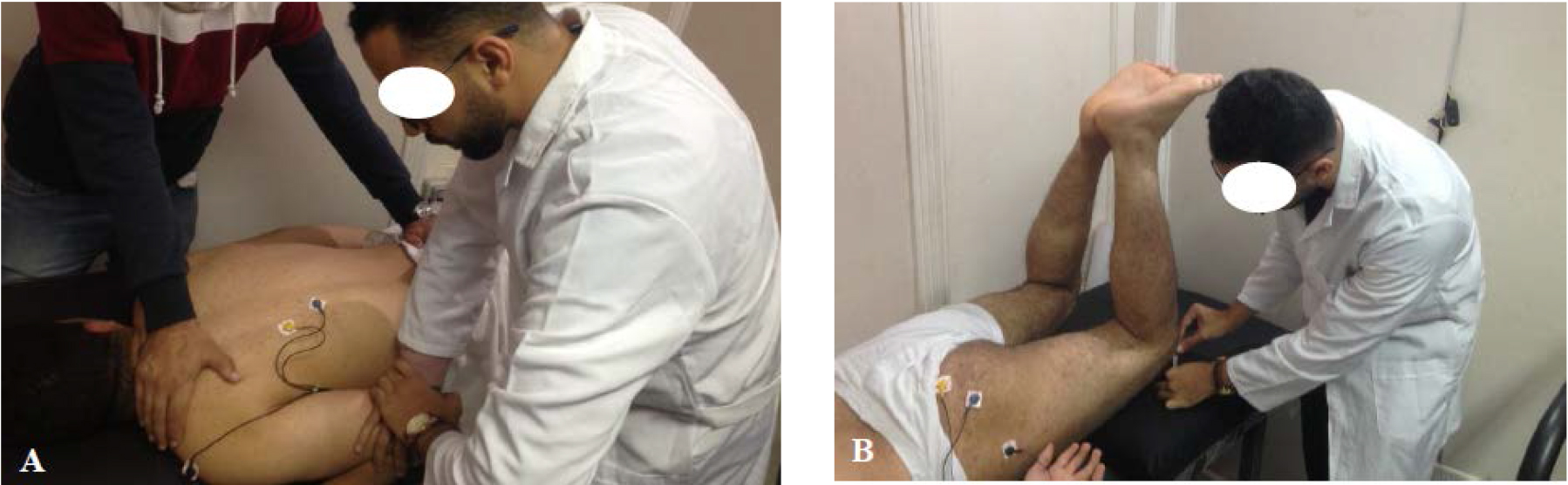
The submaximal isometric contraction method was used to normalize the RMS value of the gluteus maximus muscle. The participants were asked to lift both knees 5 cm above the plinth and keep this position for five seconds while lying down with their knees flexed at 90
The Plurimeter-V gravity Inclinometer (Baseline 12-1056 bubble inclinometer, USA) was used as an effective and reliable tool for measuring the upward scapular rotation in all shoulder abduction ranges in the frontal plane [25].
The degree of upward scapular rotation was measured by using two inclinometers. The first inclinometer was taped vertically to the arm, just above the humerus’s lateral epicondyle. The participants were asked to abduct their shoulder with complete elbow extension and neutral wrist position while the examiner registered the humeral resting position. The participants were instructed to stop the movement at 45
Measurement of upward rotation of the scapula.
Statistical analysis was carried out using the Statistical Package for the Social Sciences (SPSS; IBM Corp., Armonk, NY, USA) version 24 for Windows. The data were normally distributed as indicated by non-significant values of the Shapiro-Wilk normality test (
Results
As shown in Table 1, the difference in mean age, weight, height, or BMI between the two groups was non-significant (
The RMS values of the latissimus dorsi muscle of the LBP group were significantly higher than those of the control group on both sides (
Demographic characteristics of the participants
Demographic characteristics of the participants
Data are presented as mean
RMS of latissimus dorsi and gluteus maximus muscles
Data are presented as mean
Scapular upward rotation values from different shoulder abduction positions
Data are presented as mean
The upward scapular rotation of the right and left sides of the chronic LBP group were significantly lower than those of the control group in different shoulder abduction positions: neutral position, 45
The present study revealed that the subjects with chronic LBP have bilateral increased EMG activities of latissimus dorsi muscle and decreased EMG activities of gluteus maximus muscle compared to healthy subjects without difference between the right and left sides. Moreover, there is an increased scapular upward rotation ROM of subjects with chronic LBP compared to healthy subjects with the left side scapular upward rotation ROM of both groups was more significant than the right side.
Changes in motor control due to chronic LBP may cause abnormality in muscle activation pattern, timing and rate of force development [6]. The muscles and joints of the lumbopelvic region provide proximal stability to allow optimum force production and transmission for extremity distal mobility through a kinetic chain. Insufficient support of the trunk may affect arm injuries through breaks in the kinetic chain [7].
In patients with chronic LBP, Taghizadeh et al. [15] observed an increased upward rotation of the scapula at neutral position and shoulder abduction of 40
These findings are in line with those of the previous study that demonstrated a significant increase in latissimus dorsi muscle activation in women with chronic LBP, compared to healthy women during the PHE task [9]. This can be attributed to the ability of healthy women to stabilize the lumbopelvic region more efficiently than women with chronic LBP. Increased latissimus dorsi muscle activation is required to complete the task. As the gluteus maximus muscle on one side fails to control the pelvis during PHE, the thoracolumbar spine rotates to the opposite side. As a compensatory mechanism for that faulty movement, the contralateral latissimus dorsi muscle’s over-activation may execute during the PHE task [28, 29].
Furthermore, the increased EMG activity of the latissimus dorsi muscle is coincident with the findings of Masaki et al. [30], who reported that the activity of latissimus dorsi muscle increased in patients with LBP, enhancing the compressive and shear stress on the intervertebral disks and leading to a recurrence of LBP symptoms. Moreover, the increased latissimus dorsi muscle activation attached to the lower tip of the scapula affects the scapula’s upward rotation position. It pulls the inferior tip of the scapula superiorly and laterally during arm elevation (increased upward rotation), which inserts into the humerus [15].
However, the findings of the current study do not support the previous research, which demonstrated no major differences in latissimus dorsi muscle EMG activity while lifting bags in several different conditions in female students with chronic LBP [27]. This may be due to the use of a different task to measure the latissimus dorsi muscle’s activity level. On the other hand, the present findings are in keeping with this previous study, which shown no differences in latissmus dorsi muscles EMG activity during lifting bags in many different conditions in female students with chronic LBP [27]. This may be attributed to use another task to assess the activity level of the latissimus dorsi muscle. This finding is contrary to previous studies, showing significantly lower endurance in back extensors in collegiate male athletes with LBP than healthy male athletes [31].
The decreased EMG activity of the gluteus maximus muscle may follow the pain adaptation model, predicting a reduction in the activity of the motor neuron output of agonist’s muscle due to pain (shorter muscle) and increased activity antagonist muscles (elongated muscle). This can, in turn, lead to a reduction in the MVC and range and velocity of movement. All these adaptations aim to protect the injured part against more injury [32, 33]. Furthermore, this finding supports a study that revealed a substantial reduction in concentric torque of hip extensor muscles in females with LBP compared to healthy subjects [20].
The results of Leinonen et al. [21], who observed the same result during forward bending in patients with chronic LBP, may explain the substantial reduction in gluteus maximus muscle function. They clarified that the pain caused the patients to stop using their back muscles during everyday activities, leading the back muscles, particularly the multifidus muscle, to atrophy. As a result, the gluteus maximus muscle, which functions in conjunction with the lumbar paraspinal muscles, is affected by this deconditioning state. Moreover, some research works found a significantly delayed onset of gluteus maximus muscle activity while performing PHE tests in patients with LBP compared to healthy individuals [18, 34, 35, 36].
These findings are also consistent with those Tateuchi et al. [37], who discovered a significant decrease in gluteus maximus muscle activation with the semitendinosus muscle during PHE caused by increased hip flexor activation, resulting in increased anterior pelvic tilting in healthy subjects. Their findings indicated an agonist and antagonist imbalance of the hip muscles. Moreover, there is an increased lumbopelvic motion due to the delayed trunk muscle onset [37]. Wattananon et al. [13] observed a similar result to the current study despite their limited sample size (8 subjects). They reported that chronic LBP leads to less bilaterally activation of the gluteus maximus muscle, associated with greater pelvic and less lumbar spine contribution to the forward bending task.
However, Himmelreich et al. [38] showed that the LBP is associated with changes in the amount and duration of gluteus maximus activation under different gait conditions (level ambulation, incline walking, and stair ascent). The alterations may be compensated to increase the lumbopelvic stabilization. There is an average increase in the gluteus maximus muscle activity of about 35% in incline walking and stair climbing in men with chronic LBP. Furthermore, Kim et al. [29] found that females with chronic LBP had significantly higher EMG activity of the gluteus maximus than healthy subjects during PHE, contradicting the current findings. The increased activity of the gluteus maximus muscle is needed to support the pelvic and thoracolumbar regions during the PHE task. There is a laxity in the ligaments supporting the pelvic in women with chronic LBP, explaining their results [29, 30, 39]. Their sample consisted of females, causing this contradiction, whereas in the current study only males were enrolled.
It was found that the left side (non-dominant) upward scapular rotation in different shoulder abduction positions, i.e. neutral position, 45
This study is not without limitations. First, the assessment included only the latissimus dorsi and gluteus maximus muscles of the posterior oblique sling. Second, the position of the scapula could be altered by the erector spinae or hamstring muscles. Third, only adult male subjects with chronic LBP were recruited for the current study. Accordingly, the interpretation of the findings is limited to this specific population and cannot be generalized to other types of LBP, females, or elderly subjects. Future research is required to investigate the effect of lumbopelvic muscle activation patterns on lumbar and pelvic kinematics and the relationship between EMG activity pattern and the trunk extensors and trunk muscles strength endurance in patients with chronic LBP.
Conclusion
Chronic LBP leads to a bilateral increased EMG activity pattern of latissimus dorsi muscle and decreased EMG activities of gluteus maximus muscle than healthy males, without difference between the right and left sides. Moreover, males with chronic LBP had a bilateral increased scapular upward rotation compared to healthy subjects in different shoulder abduction positions. The left side rotation was more significant than the right side of both groups. These results should be taken into account in patients with chronic LBP and scapular dyskinesia when assessing and treating the lumbopelvic region. Moreover, clinicians should focus not only on the proximal cause of the lesion but also on the distal vital points that may affect the LBP prognosis.
Footnotes
Acknowledgments
The authors would like to acknowledge the participants of the study.
Conflict of interest
There are no conflicts of interest.
Funding
The authors received no financial support for this research.