
Abstract
BACKGROUND:
Exercise training after lumbar fusion surgery (LFS) is important for regaining the strength in the spinal muscles, pain management, and minimizing dysfunction. It may be prudent to evaluate technologies such as web-based chat and social media apps for increasing the efficacy of post-surgery interventions in LFS patients.
OBJECTIVE:
To explore the effectiveness of a WeChat-based individualized post-discharge rehabilitation program in patients with LFS.
METHODS:
Seventy-two eligible discharged LFS patients were enrolled from October 2018 to February 2019. The experimental group (36 cases) received a 10-week WeChat-based individualized rehabilitation program, while the control group (36 cases) received routine follow-up guidance. The outcomes were measured using the Exercise Compliance Questionnaire, Numerical Rating Scale, Oswestry Disability Index and Chinese version of the self-efficacy for exercise scale.
RESULTS:
The analysis using generalized estimation equations method shows significant differences in the interaction effect of group*time in exercise compliance (Wald
CONCLUSIONS:
The WeChat-based rehabilitation intervention can improve exercise compliance and self-efficacy, and help achieve greater pain relief compared to the routine intervention. However, the WeChat-based intervention did not offer better improvement in the self-dysfunction in the post-discharge LFS patients.
Introduction
Lumbar fusion surgery (LFS) is a surgical procedure in which vertebrae in the lower back are surgically joined together, minimizing movement between them. The goal of the procedure is to relieve pain caused by the inter-vertebral movement and is one of the most commonly used procedures for the treatment of the degenerative disorders of the spine, such as lumbar disc herniation and lumbar spondylolisthesis [1].
During the last 20 years, the rates of LFS (procedures performed per 100,000 of the population) have increased considerably [2, 3]. However, the rehabilitation of patients after discharge has not been satisfactory and residual pain, and moderate impairment of mobility are wide spread in LFS patients [4, 5], which leads to restrictions in their day-to-day activities [5], and also prolong the time required to return to work [6].
Spinal surgery is an invasive procedure and requires a long healing time. It has been shown that LFS patients with pain and dysfunction may benefit from a postoperative rehabilitation program [7]. However, evidence-based rehabilitation guidelines for LFS patients are lacking, and the best layout for an effective postoperative rehabilitation program has still not been developed. Additionally, the rehabilitation service system in China is inadequate to meet the needs of LFS patients, and the hierarchical and staged rehabilitation service is difficult to be implemented [8]. Thus, most LFS patients have to choose a routine home-based rehabilitation program after surgery [9].
WeChat is a multi-purpose messaging and social media mobile application (app) that allows users to communicate in real-time using text and video messages and overcomes the limitations of time and space. WeChat was launched in January 2011, and within three years the number of users crossed 600 million, roughly the same number as mobile internet users in China. WeChat has become an essential app for smartphones [1] and offers the possibility of providing instructions to the discharged LFS patients during their home-based rehabilitation.
This study aimed to evaluate the formulation and implementation of an effective WeChat-based individualized post-discharge rehabilitation program for LFS patients with the participation of clinicians, rehabilitation therapists, and clinical nurses.
Methods
Study design and participants
A quasi-experimental design was used in this study. The patients discharged after LFS from the Spinal Surgery Department of the First People Hospital of Nantong, China (a Class III A hospital located in Nantong, China) were recruited by using the convenience sampling method from October 2018 to February 2019.
Inclusion and exclusion criteria
All patients included in the study met the following criteria: (1) underwent LFS with no prior history of spinal surgery; (2) received routine nursing care in the spinal surgery department of the hospital as per surgeon’s discharge instructions; (3) were able to use smart phones and the WeChat app; and (4) were over 18 years of age and willing to cooperate in the data collection.
The exclusion criteria were: (1) pregnancy; (2) serious organ diseases such as that of liver, lung, and brain; (3) inability to exercise due to musculoskeletal disorders or limb and joint deformities; and (4) readmission or reoperation due to disease progression or improper treatment.
Sample size
G*Power 3.1 was used to calculate an appropriate sample size for the study. We set the test family to ‘F test’, the statistical test to ‘ANOVA: repeated measures, between factors’, and the type of power analysis to ‘A priori: compute required sample size-given
Routine hospitalized patient exercise rehabilitation program
All participants went through a routine exercise rehabilitation program supervised by the spine surgeons and rehabilitation therapists during the hospital stay. The routine exercise rehabilitation program included: (1) 30 ankle pump exercise 3 times a day: the patients were asked to lie down supine with relaxed thighs and move the toes up and down slowly and forcefully, maintaining each posture for 5–10 s. (2) 30 straight leg rising training 3 times a day: one day after the surgery, the patients were instructed to lie down supine with straight legs, and the ankle joint extended outwards. The patients were then asked to raise the left and right leg alternately at an angle of 30–45
Procedures of the experimental group
Preparation phase
An intervention team was built, including the surgeons, nurses, rehabilitation therapists, and the researchers. A rehabilitation file was created for each participant in which the demographic data, disease-related data and the medications to be taken after the discharge were compiled.
Design of a post-discharge rehabilitation program for the LFS patients
A post-discharge rehabilitation program for the LFS patients was designed based on the literature survey, group meetings, discussions and experiments, which included exercise rehabilitation, posture correction education, daily activity education, correct instructions for lumbar brace wearing, and self-management of pain (Table 1). Based on this, we formulated the WeChat-based electronic education manual for the discharged patients.
Implementation phase
The day before discharge
On the day before discharge, the spine surgeons and the rehabilitation therapists assessed the patient’s recovery and exercise ability and formulated the individualized post-discharge rehabilitation program, including exercise types, number of sessions in a day, repetitions of each exercise in a session, duration of each session and precautions. The researchers recorded the elements of post-discharge rehabilitation program for each patient and stored them in the patient’s rehabilitation file.
The researchers educated the patients and their family members about LFS, the possibility of fluctuations in the pain and recurrence of the original disease, clinical manifestations of a worsening condition, and the corresponding countermeasures to be taken. The researcher also informed the patients about the importance of rehabilitation after LFS, and asked family members to help the patients to participate in the rehabilitation program, and maintain a positive lifestyle.
The patients in the experimental group were invited to join the WeChat group named as ‘Post-discharge Rehabilitation Management for Patients with Lumbar Fusion Surgery’.
Post-discharge stage
The rehabilitation of the experimental group was conducted via WeChat. Group meetings were held every fortnight, where the researcher informed the team of problems and issues raised by the patient during the intervention. Solutions were discussed and recorded during the meetings and these solutions were communicated to the patient through WeChat the next day.
Procedures of the control group
On the day before the discharge, the researchers communicated the routine discharge instructions to the patients and followed-up by telephone in the first, second and third months after the surgery. The instructions at the time of follow-up included those pertaining to exercise rehabilitation, medication schedule, and lumbar brace wearing/unloading. If participants had any problems, they could contact the researcher at any time by telephone.
Measurements
The data were collected using five different questionnaires: the general data questionnaire; the exercise compliance questionnaire, the numerical rating scale (NRS); the Oswestry Disability Index (ODI), and the Chinese version of the self-efficacy for exercise scale (SEE-C).
The self-designed general data questionnaire was aimed at gathering the demographic, disease, and discharge medication-related data of the participants.
The exercise compliance questionnaire was designed as per Qiong-Ya Cao [11] and aimed to evaluate the exercise compliance of the participants in terms of frequency, types, duration, and outcomes. Responses were scored on a 4-point Likert scale (1
NRS is one of the widely used tools for the assessment of pain in lower-back pain patients, with an acceptable retest reliability, constructive validity, and responsiveness [12]. The intra-class correlation coefficient (ICC) of the NRS is 0.95 [13].
ODI is the ‘gold standard’ method to evaluate the self-dysfunction of patients with low back pain in the field of spinal surgery [14]. The Cronbach alpha coefficient of ODI is 0.86, and inter-rater and intra-rater reliability yield ICC of 0.94 and 0.95, respectively [15].
SEE-C contains 18 items, and the score of each item is from 0 to 100; 100 points indicate full confidence,
The post-discharge rehabilitation program for LFS patients
The post-discharge rehabilitation program for LFS patients
50 points indicate half confidence, and 0 points indicate no confidence at all. The SEE-C score is calculated by adding the scores of each item and dividing it by the total number of items. The Cronbach’s alpha coefficient of SEE-C is 0.75 [16], lower than the corresponding value of 0.95 of the original English version [17]. However, the SEE-C was chosen over the original version as its NFI is 0.90, RMSEA is less than 0.10 and the confirmatory factor analysis of SEE-C suggested a fair model fit [16].
This study was approved and supported by the school of nursing of Nantong University and the Spinal Surgery Department of the First People Hospital of Nantong, China, and was registered under trial registration number CTR2000033947. The disease-related information of the patients was obtained by referring to the case files. The data was collected on the day before discharge, and in third first, second and third months after the surgery. The time of outcome measurements in the control group was the same, but the method of outcome measurements was by telephone.
Ethical considerations
Ethical approval for the study was obtained from the Ethics Committee of the First People Hospital of Nantong, China (no. 2019026). The patients were provided with information related to the research and their rights were explained. Informed consent was obtained from all patients before the start of the study, and the patients were informed about the policy of maintaining the confidentiality of their personal data. All subjects were anonymized and voluntarily participated in the study.
Data analysis
Data were analyzed by SPSS Version 23.0 (IBM Corp., Armonk, NY, USA). Continuous variables were presented as mean (standard deviation) or inter-quartile range, and categorical variables and ranked data as frequencies. The baseline data were compared between groups using
Results
Participant enrolment and withdrawal
Thirty-six eligible patients from the Spinal Surgery Department of the First People Hospital of Nantong were enrolled in the control group from October 2018 to November 2018, and thirty-six eligible patients were enrolled in the experimental group from December 2018 to February 2019. One participant from the experimental group dropped out during the study due to readmission. Five participants from the control group dropped out due to readmission (2 cases) and other reasons (3 cases) (Fig. 1).
Demographic and clinical characteristics
Before the intervention, there were no significant differences between the experimental and control group in demographic data, except for age and education level. The disease related information and the discharge medication of patients, and all outcome measures were also not statistically different (Table 2).
Comparison of demographic data, disease-related data and discharge medication between the experimental and control group
Comparison of demographic data, disease-related data and discharge medication between the experimental and control group
Note:
The study flowchart diagram (including the drop-outs during the research).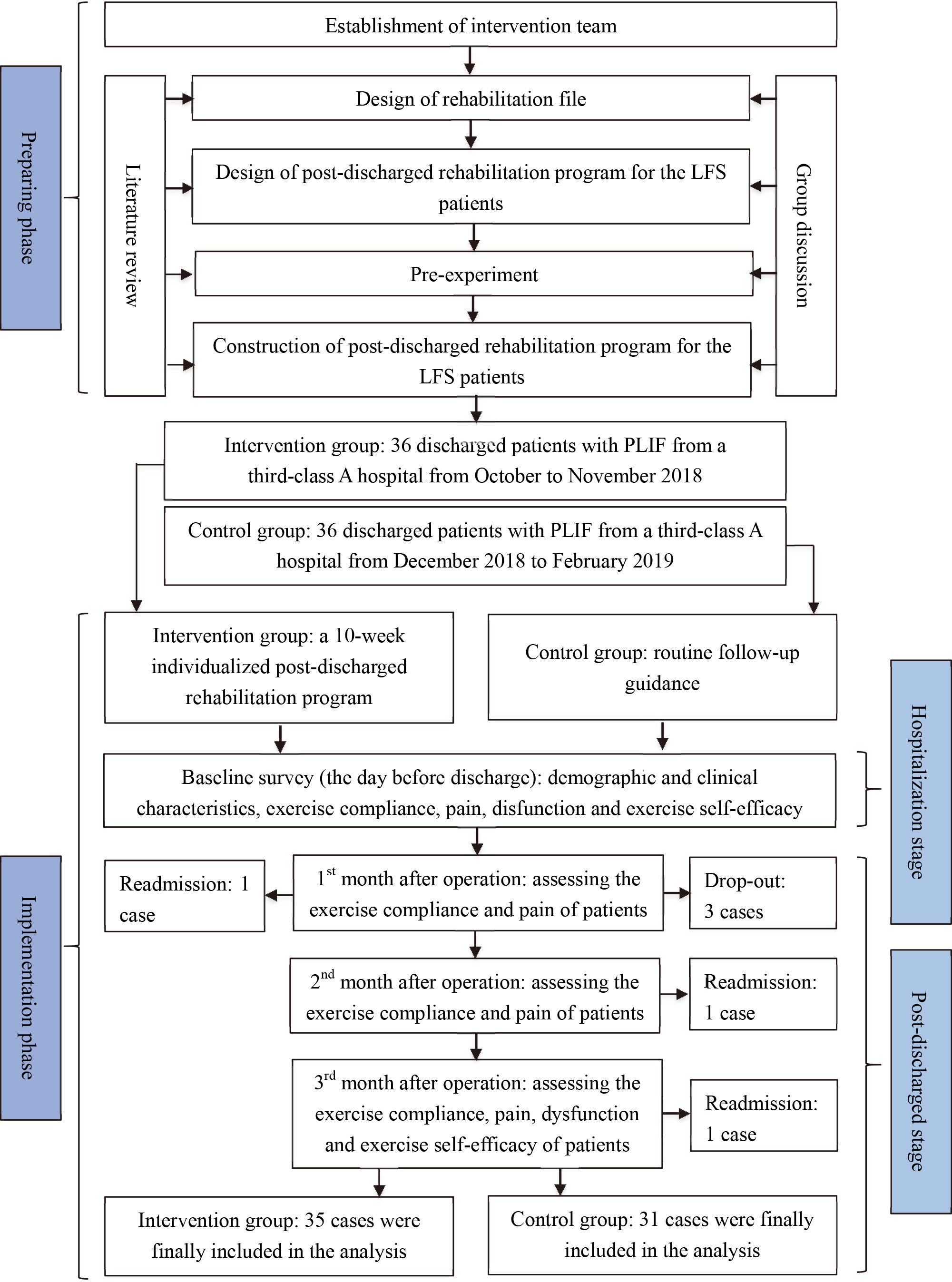
Comparison of the score of exercise compliance between the experimental and control group after the intervention
The GEE results showed a significant difference in group*time interaction effect on the score of exercise compliance (Wald
GEE results of outcome measurements after intervention
GEE results of outcome measurements after intervention
Note:
Marginal analysis results of the outcome measurements after intervention
Note:
The GEE results showed a significant difference in group effect (Wald
Secondary outcomes
Comparison of the score of dysfunction improvement between the experimental and control group after the intervention
The GEE results showed no significant difference in group effect in the score of dysfunctions improvement (Wald
Comparison of the score of exercise self-efficacy between the experimental and control group after the intervention
The GEE results showed a significant difference in group effect in the score of exercise self-efficacy (Wald
Discussion
The WeChat-based individualized post-discharge rehabilitation program can improve exercise compliance and relieve pain in LFS patients
Non-compliance is recognized as one of the most important factors affecting clinical therapeutic outcomes and result in a significant economic burden on the health care system [18, 19]. Studies have shown that an individualized intervention, designed according to preferences, exercise environment, physical fitness, and exercise experience of the LFS patients is more effective in improving exercise compliance than routine intervention [20]. The results of this study show that the WeChat-based intervention was more effective in improving exercise compliance in the patients compared with the routine intervention. The effective interaction between the medical staff and the patients and frequent monitoring and supervision by the medical staff may play a role in improving the exercise compliance of LFS patients [21]. The exercise self-efficacy of the experimental group was significantly higher than that of the control group, which may have a positive impact on the exercise compliance of LFS patients. However, the OR ratio of the pre-intervention exercise compliance score was as high as 1.508. This result indirectly shows that the participants’ exercise compliance before intervention has an important influence on exercise compliance after the intervention. We speculate that participants with higher exercise compliance before the intervention are more likely to follow the instructions provided during the intervention.
The co-administration of a number of medicines in the LFS patients makes the pain management difficult due to drug-drug interactions [22]. The medical staff has become increasingly aware of the problem of non-adherence of patients with the pain management guidelines [23, 24]. Despite stepped-up efforts by the researchers and the clinicians, ineffective post-operative pain management, is still a common problem [25, 26]. Self-management of pain is an important part of the intervention in this study. The results of this study show that the WeChat-based intervention is more effective in relieving the pain of patients with LFS compared with routine intervention. We speculate that two main factors associated with the WeChat-based intervention contribute to better pain management in the experimental group. First, patients accepted and applied the concept of preventive analgesia and took the important role of non-steroidal anti-inflammatory drugs in pain self-management seriously [27]. Taking analgesics before the occurrence of pain or taking them soon after the pain is felt prevents acute pain from developing into chronic pain. Second, the experimental group had better exercise compliance, which resulted in the reduction of pain. Chinese experts on pain self-management have suggested that patients with LFS should perform “nerve root sliding exercises” (such as straight leg raising training) to prevent and relieve nerve root pain [27]. Straight leg raising training is an important part of exercise rehabilitation in this intervention.
Although GEE analysis showed a significant improvement in the pain score, a higher value of OR of the pain score before intervention indicates that the results of the pain score after the intervention may be influenced to a certain extent by the pain level of the participants before the intervention. Further research should explore the best way to study the effectiveness of pain management strategies for low levels of pain.
Lack of sufficient evidence for the effectiveness of WeChat-based individualized post-discharge rehabilitation program on improvement of dysfunction in LFS patients
Studies have found that improvement in postoperative dysfunction in young LFS patients is not as good as that in middle-aged patient [28]. A high education level has a positive impact on the improvement of nerve root pain and dysfunction in patients with LFS [29]. The authors speculated that high education levels may equip the patients with better psychological mechanisms for coping with the surgery and also help them in interpreting the post-operative symptoms positively [30]. In this study, we did not find sufficient evidence to prove that a personalized WeChat-based post-surgery rehabilitation intervention is more effective in improving dysfunction of patients with LFS compared with the routine rehabilitation. We think the main reason for this result is the short duration of the study. The weakness of the back muscle and the formation of postoperative epidural fibrosis (EF) will result in dysfunction in patients with LFS [31, 32]. It needs a long recovery period for LFS patients to adapt to the physical limitations caused by low back pain/discomfort [33]. However, the duration of rehabilitation intervention in this study is only 10 weeks after the surgery. On the basis of the results of the exercise compliance of this study, we have sufficient reasons to speculate that given a longer intervention time, the improvement in dysfunction of the patients in the experimental group might be better than the control group. Also, the types of rehabilitation exercise implemented in this study were limited, and there was a lack of specific muscle training such as multifidus muscle training and standing spine muscle training. These specific muscle trainings play an important role in maintaining spinal stability. Studies have shown that core stability training [27] and breathing training can help in attaining effective improvements in the exercise ability of trunk muscles and dysfunction of LFS patients [34]. Another factor that may have contributed to no statistically significant improvement in the dysfunction of the LFS patients is the over-use of the lumbar-brace. In one study, patients reported that the lumbar brace made them feel stable and helped them to carry out daily activities better [35]. However, long-term use of a lumbar brace may lead to back muscle weakness and injury and decrease the effectiveness of postoperative rehabilitation for LFS patients [36, 37].
The individualized post-discharge rehabilitation program based on WeChat can improve exercise self-efficacy of LFS patients
Self-efficacy refers to the confidence or belief that an individual can successfully implement and complete a certain behavioral goal or cope with a certain difficult situation. In the field of exercise, exercise self-efficacy has a more substantial influence on exercise behaviors than general self-efficacy [38]. For LFS patients with low preoperative exercise level, improvements in exercise self-efficacy is an important factor that promotes greater engagement with postoperative exercise rehabilitation. The higher the patient’s exercise self-efficacy, the more likely the patient is to participate in exercise rehabilitation actively [39].
The study shows that the WeChat-based intervention is more effective in improving exercise self-efficacy of patients with LFS compared with routine rehabilitation. However, we also found that the odds ratio of the score of exercise self-efficacy was very high. The reasons for the high OR are as follows:
We found that the ‘quasi-likelihood under the independence model criterion’ was very high for the exercise self-efficacy data, implying that the GEE model may not be a fair model fit. Also, Cronbach’s alpha coefficient of SEE-C was 0.75, which might affect the accuracy of the data. Finally, a small sample size of 72 used in this study might also result in high OR. Undoubtedly, the high odds ratio exaggerates the effect of the intervention; however, the
Thus, the individualized WeChat-based rehabilitation intervention in post-operative LFS patient intervention encouraged and helped patients by providing professional guidance on exercise routine and social support, as observed in a similar study performed earlier [40]. Further research in the direction of improvements in the structure and the elements of this WeChat-based rehabilitation intervention is needed to increase its effectiveness in improving the outcomes of post-operative exercise rehabilitation of LFS patients.
Limitations
There were several limitations of this study. First, strict randomization was not achieved in selecting the patients, which resulted in inconsistent baselines. Although the variables (age and education level) which caused baseline imbalances were included in the GEE analysis as covariants, the possibility of results being affected by unmeasured baseline imbalance variables cannot be ruled out. Second, the intervention time in this study was short, and the outcomes were measured after 10 weeks. The short duration of the study may be a reason for an insignificant difference between the control and the experimental group in the score of dysfunction. Future studies should explore the effect of long-term personalized exercise rehabilitation (at least more than six months) on postoperative rehabilitation of LFS patients, to come up with the best postoperative rehabilitation programs for LFS patients. Last, the sample size of this study was small which decreased the true power of this study to 0.727. Future studies should try to enroll a sufficient number of patients to increase the confidence in the study outcomes.
Conclusion
Although no significant difference in the improvement in the dysfunction between the experimental and control groups was found in this study, the results indicate that the WeChat-based individualized post-discharge rehabilitation program is an effective and practical way of improving exercise compliance and self-efficacy and relieving pain in LFS patients.
Footnotes
Acknowledgments
This study was supported by the Natural Science Foundation of Jiangsu Province (BK20191447).
Conflict of interest
None to report.