
Abstract
BACKGROUND:
First discussed by Dr. Robert Maigne in the late 1980s, Maigne Syndrome is an often unrecognized and treatable cause of low back pain. It can be separated into two distinct entities. The central variant is a result of nerve afferent input secondary to changes of facet joint arthropathy at the thoracolumbar junction. The peripheral variant is a result of impingement of the medial branch of the superior cluneal nerve, which arises from the posterior rami of the lower thoracic and upper lumbar nerve roots, and results in similar clinical symptoms and signs.
OBJECTIVE:
To review the current literature for a comprehensive description of Maigne Syndrome, its diagnosis and management.
METHODS:
Evidence was gathered using two main medical databases, namely PubMed and Google Scholar. Search terms included ‘Maigne’s Syndrome’, ‘Maigne facet’, ‘thoracolumbar junction syndrome’, ‘cluneal nerve entrapment’, ‘posterior iliac crest trigger point’, ‘pseudosciatica’, as well as various permutations of these terms.
RESULTS:
The initial search generated 52 articles. These were screened, and duplicate and irrelevant articles were removed. Using the remaining articles, and with evaluation of their cited references, we selected 28 articles for review. Most of these consisted of case reports, many of which were published in rehabilitation, chiropractic and medical journals. The papers explored topics such as anatomy, cluneal nerve imaging, and treatment of nerve entrapment and facet related back pain syndromes, and have been included in this review, which is, to the best our knowledge, the most comprehensive description of Maigne Syndrome to date.
CONCLUSION:
The keys to the diagnosis of Maigne Syndrome include an awareness of the mechanical causes of back dominant pain, an understanding of the relevant anatomy, a specific clinical examination, and focused radiological guided anesthetic blocks. Treatment is available, and as in all back-pain etiologies, is most effective in the early stages of the disease.
Keywords
Introduction
Low back pain is a common problem with approximately 85% of people experiencing it at some point [1, 2]. Considering the extensive list of causes, prompt and accurate diagnosis of low back pain can be a major challenge.
Maigne Syndrome is an underappreciated etiology of low back pain with unique biomechanical causes separated into two distinct entities: the “Thoracolumbar Junction Syndrome” or the “central variant” and the “Cluneal Nerve Entrapment Syndrome” or the “peripheral variant”. The former is due to spinal nerve irritation secondary to possible referred pain from peri-articular structures including facet joint degeneration at the transitional vertebra (usually T12-L1), and the latter involves impingement of the medial superior or middle cluneal nerve branches peripherally [3] (Figs 1 and 2).
Our aim is to raise awareness of Maigne Syndrome in patients who present with primarily low back pain and discuss the importance of history and physical examination, relevant diagnostic techniques, and available treatment options. Maigne Syndrome is modifiable with timely diagnosis and appropriate management [4].
Causes of low back pain by prevalence
Causes of low back pain by prevalence
Due to the relative lack of distinguishing demographic and clinical features, and the plethora of common causes of low back pain, Maigne Syndrome is an often-under appreciated diagnosis for lower back pain. (Table 1) [4, 5, 6, 7, 8, 9, 10]. The first description was made by Strong and Davila in 1957, who attempted deafferentation of the superior cluneal nerve in 30 patients [11]. They reported that 9.8% of their 122 patients admitted to hospital because of LBP had a superior cluneal nerve disorder. The actual prevalence and incidence is difficult to be accurate about. According to Kuniya et al. in a prospective study of 834 consecutive patients in a surgical spine centre clinic the incidence was 14% [12].
Maigne Syndrome was further elucidated by Dr. Robert Maigne, with a reported incidence of 40% in 350 patients that presented with low back pain [4]. In Maigne’s 2 year follow up study on 19 patients operated on for entrapment of the cluneal nerve at the iliac crest, excellent results were found in 13 of 19 patients. This study looked at 1800 patients with low back pain without sciatica, seen in their spine clinic with an incidence of 1.6% [13].
Low back pain due to peripheral cluneal nerve impingement shows a prevalence of 1.6%–14% [14]. The majority of the literature are case reports and case series as outlined in a review by Isu and colleagues [14].
Axial depiction at T12 level showing the dorsal root ganglion (DRG), dorsal and ventral ramus, articular branches of the dorsal ramus, and the origin of the medial branch of the superior cluneal nerve.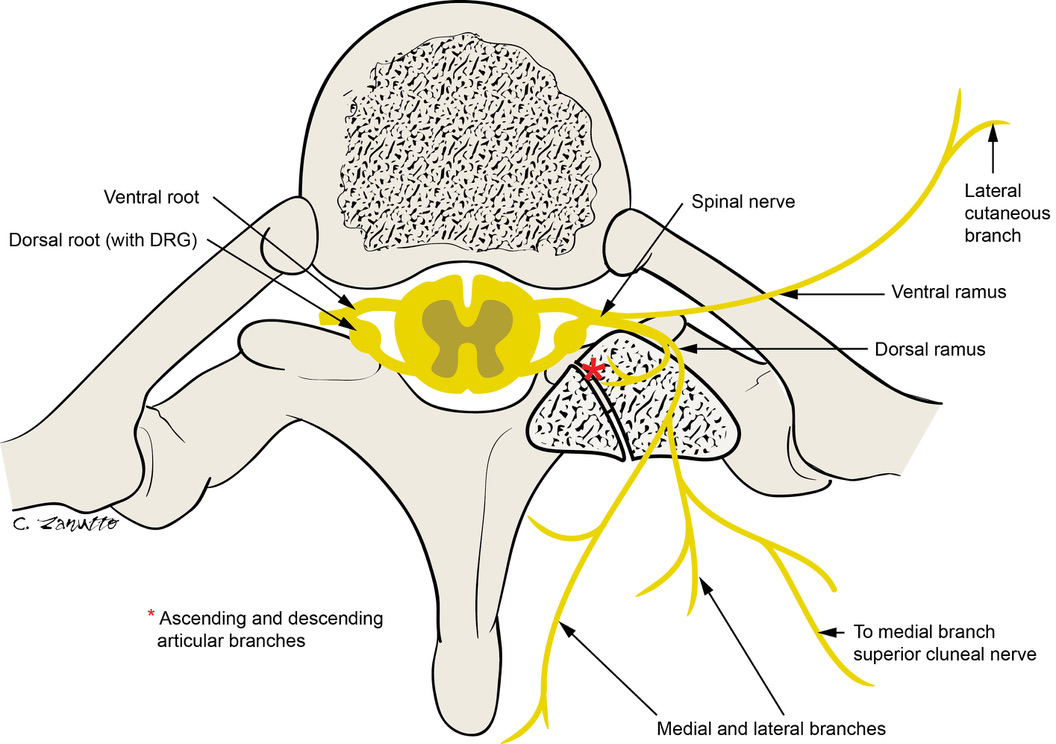
Maigne Syndrome can be divided into two distinct entities, the “central variant” also referred to as “Thoracolumbar Junction Syndrome” and the “peripheral variant” also referred to as “Cluneal Nerve Entrapment Syndromes”.
The central variant or Thoracolumbar Junction Syndrome (also known as spinal dorsal ramus mediated back pain) involves pathology at the thoracolumbar junction. The pathology is a result of spinal nerve irritation (afferent input) secondary to ligamentous, capsule, and or facet (zygapophyseal) joint degeneration [15, 16].
The thoracolumbar junction endures unique rotational and flexion/extension forces. This is due to the facet orientation and morphology of thoracic and lumbar vertebrae [4]. The facets of the thoracic spine are oriented primarily in the coronal plane with a joint inclination of approximately 60–70 degrees (Fig. 3). This orientation permits more rotation. In contrast, the lumbar facets are oriented primarily in a sagittal plane with a joint inclination angle of approximately 90 degrees, permitting less rotation but more flexion/extension (Fig. 3) [17]. The facet morphology at T12-L1 level is transitional with a structure that combines elements of both the thoracic and lumbar facet orientation, and therefore allows for both rotation and flexion/extension. This increased mobility is also a result of the lack of restraint of the 11
Diagram of the medial branch of the superior cluneal nerve taking origin at T12-L1 level (bold black arrow). The nerve penetrates the dorso-lumbar fascia at the level of the iliac crest via an osteoaponeurotic channel (black star), approximately 7 cm from midline.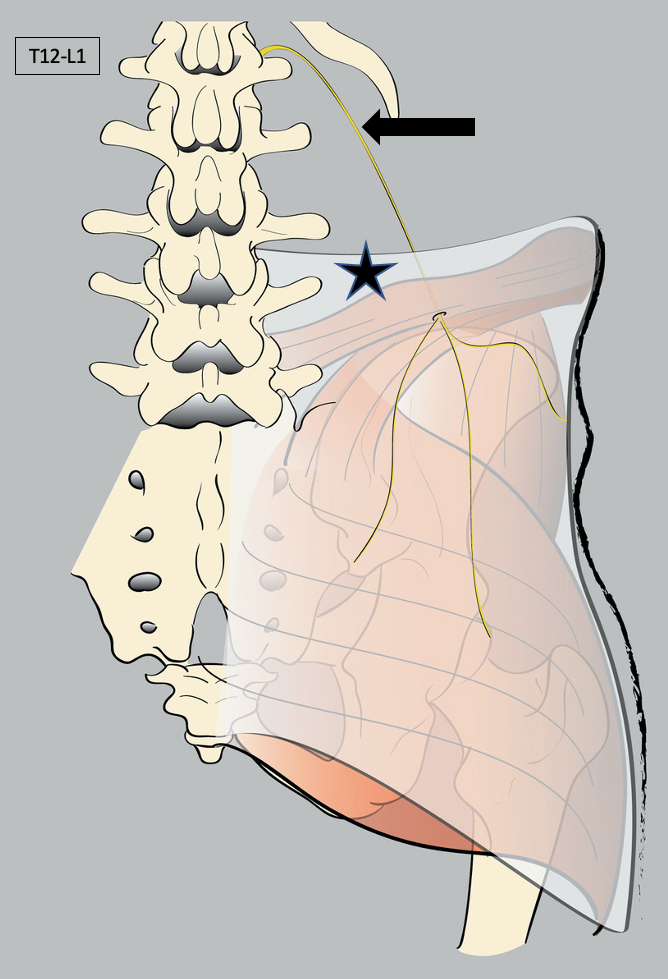
A) Sagittal MRI showing inclination angle of 70 degrees for the thoracic facets (arrow) and 85 degrees for the lumbar facets (star). B) Coronal orientation of the thoracic facets; and C) sagittal orientation of the lumbar facets, in the axial plane.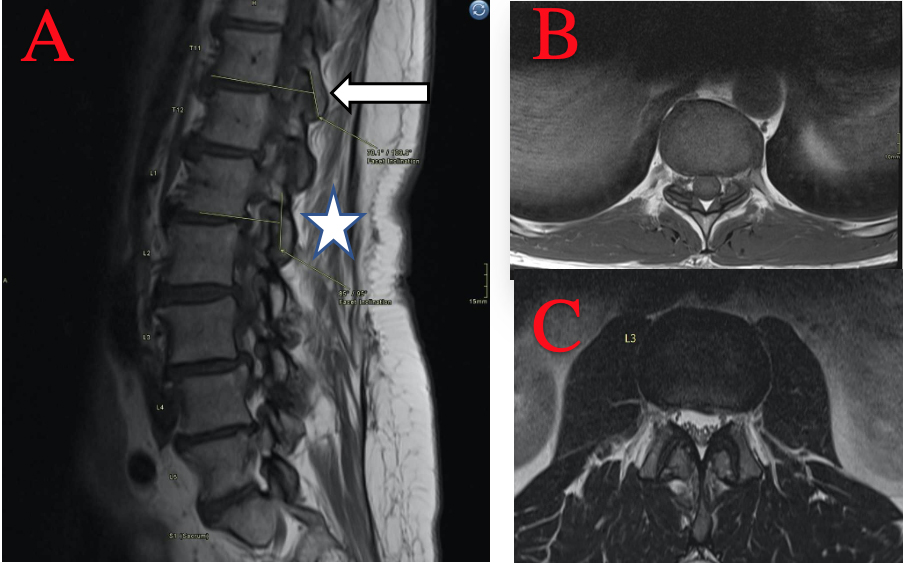
At the thoracolumbar junction, the T12 and L1 spinal nerves with their anterior and posterior rami are the main neural elements involved in Maigne Syndrome and have a distinct innervation pattern [4, 19] (Fig. 1). The ventral (anterior) ramus innervates the inferior abdomen, groin, and pubic area. A perforating lateral cutaneous branch also innervates the trochanteric region. The dorsal (posterior) ramus innervates the subcutaneous tissues of superior gluteal and inferior lumbar regions. The lateral branches of the dorsal ramus innervate the longissimus and costo-lumbar muscles, and skin of the back lateral to the line traced along the facet joints. The medial branches of the dorsal ramus innervate facet joints, paraspinal muscles, and skin of the back medial to the line traced along the facet joints. This pattern of innervation explains the possible diffuse nature of symptoms associated with the referred phenomena and nerve “irritation” and the potential abnormal afferent input to the central nervous system in pain syndromes such as Maigne Syndrome, including low back pain, pseudo-sciatica, hip pain and pseudovisceral pain.
Approximately 60% of the Maigne Syndrome patients exhibit pathology at T12- L1 level [20]. Less frequently, abnormalities occur at T11-12 or L1-2 levels [21]. A subset of military and athletes, particularly those involved with excessive extensional and rotational movements of the spine can be predisposed to Maigne Syndrome. Examples include military personnel [22] weightlifters, equestrian riders, hockey players and football players [23].
In the peripheral variant, the medial branch of the superior cluneal nerve becomes impinged within an osteoaponeurotic tunnel as it pierces the thoracolumbar fascia [24, 25] (Fig. 2). The superior cluneal nerve takes its origin from the terminal lateral branches of dorsal rami of the T11 to L4 spinal nerves and has three branches: medial, intermediate, and lateral [19, 26] (Fig. 1). The medial branch of the superior cluneal nerve passes through an osteoaponeurotic tunnel bounded by the iliac crest inferiorly and the dorso-lumbar fascia superiorly. This osteo-aponeurotic tunnel is located approximately 7 cm from midline, at the level of the posterior superior iliac spine [24]. Nerve impingement within this tunnel can result in the spectrum of symptoms described as Maigne Syndrome and the Cluneal Nerve Entrapment disorders [12, 13, 14].
A variety of predisposing conditions have also been described for this variant including postural deformities in Parkinsonism resulting in stiffening of the thoracolumbar fascia [27], iatrogenic injury to the superior cluneal nerve following bone harvesting procedures at the posterior iliac crest [28], failed back surgery [29], and nerve irritation secondary to intragluteal injections [30]. In six patients who underwent neurectomy of the superior cluneal nerve, the resected nerve showed abnormal pathology including decreased fibre density, perineurial thickening, and loss of myelinated fibres suggesting pathological evidence of nerve entrapment can elicit LBP [31].
Clinical findings
The most common symptom is pain referred to structures innervated by the dorsal rami of the T11, T12 and L1 spinal nerves [3, 10, 15, 32]. Both the central and peripheral variants of Maigne Syndrome may produce pain referred to the lower back, gluteal, symphysis pubis, groin, and thigh regions. Aggravating factors include bending and rotation of the spine. Patients often attribute the pain to an episode of spinal extension and/or rotation. The two variants are often indistinguishable with respect to the patient’s presentation [4, 23, 24]. Other symptomatology is varied and is experienced in the areas supplied by the ventral ramus of the involved spinal nerves. This is summarized in Table 2.
Symptoms and signs of Maigne Syndrome
Symptoms and signs of Maigne Syndrome
Segmental examination often elicits focal tenderness in the back at the T12-L1 level but can sometimes occur at the T11-T12 level or the L1-L2 level [4]. With the patient in the prone position, tenderness by direct pressure can be elicited at various other points enumerated in Table 2.
Cutaneous changes are manifested as alteration in the skin texture, increased sensitivity of the soft tissues, and intramuscular taut bands in regions innervated by the posterior and anterior rami of the involved spinal nerves. Maigne called these “dermocellulagic changes” and described a “pinch and roll” maneuver in the affected regions and comparison with the unaffected side to help with detection (Table 2). Findings range from normal skin texture to thickened, edematous skin, associated skin discoloration, hypoesthesia, and rash [21]. The involved areas include the posterior inferior lumbar, superior gluteal, superomedial thigh, greater trochanteric regions, and bilateral inferior abdominal quadrants.
Imaging diagnosis
Diagnosing Maigne Syndrome requires clinical skill as the imaging findings associated with Maigne Syndrome have not been well documented, and are rarely diagnostic and or clinically helpful. Radiography is often the first modality employed to assess low back pain, which may show facet joint degenerative change at the thoracolumbar junction. CT may be employed to assess the bony anatomy if radiographs are equivocal. MRI is useful to assess disc degenerative disease, central canal or neural foraminal narrowing, and cord or nerve impingement from disc or facet abnormalities. Unfortunately, the majority of people who experience back pain and are investigated with imaging show considerable degenerative changes, especially in the lumbar spine, and the difficulty lies in correlating structural problems with patient’s symptomatology [32, 33]. Often, a mismatch between radiological findings and symptom distribution exist in terms of location as well as severity of radiological abnormality [34, 35].
Recent developments in ultrasonography have aided in imaging of the cutaneous sensory cluneal nerves using high-resolution US probes to determine sites of nerve impingement that could result in the peripheral variant of Maigne Syndrome [22, 35]. In our opinion, promising diagnostic techniques involve targeted nerve blocks. Several techniques have been described, with the most accurate involving double-blind placebo controlled targeted nerve blocks, which can be used to confirm and localize pain-producing pathology to the T11-12 or T12-L1 facet joints, or posterior iliac crest locations. This technique, known as a ‘triple block’, described by Lord et al involves three fluoroscopy-guided nerve blocks at the suspected culprit locations [36]. For the first injection, one of two local anesthetics (2% lidocaine or 0.5% bupivicaine) are randomly chosen to ensure that pain producing pathology stems from the injected site (evidenced by profound or complete pain resolution for the duration of the action of the local anesthetic). Sometime later, a second injection is done, where normal saline or the other local anesthetic is chosen randomly. For the third injection, the agent which was not used in the first or second injection is used. All injections must be under strict double-blind conditions (patient and physician unaware of the substance being injected), with 0.5 mL generally used for each injection. The location of pain producing pathology is considered confirmed only if the patient has complete relief of pain each time the local anesthetic is used and no relief when normal saline is used [36]. Ultrasound can be used to guide diagnostic block of the medial superior cluneal nerve if the peripheral variant is suspected [37].
Treatment
Effective diagnosis of Maigne Syndrome is critical for appropriate treatment as treatment targeted on non-culprit anatomy may lead to delay in effective treatment, failed low back surgery, significant cost to the medical system, and stress for both the patient and treating professional. Ideally, treatment of Maigne Syndrome should be directed at the involved thoracolumbar junction segment for the central variant or at the site of peripheral nerve entrapment for the peripheral variant. Differentiation between the central versus the peripheral variants can be achieved using the above-mentioned clinical examination and fluoroscopy or ultrasound- guided diagnostic block techniques. Unfortunately, these techniques are not often in widespread use, and therefore, most treatments mentioned in the literature currently are not targeted with respect to central variant versus peripheral variant of the disease.
Initial conservative treatment options include thoracolumbar exercise protocols, analgesic and/or anti-inflammatory medication, and targeted spinal manipulation therapy, with the latter exhibiting excellent therapeutic response [18, 33, 38]. Exercises that focus on strengthening of the segmental paravertebral (multifidus, and rotatores) back muscles can also be beneficial [39]. When spinal manipulative therapy is contraindicated (i.e. fractures or instability, advanced osteoporosis and osteogenesis imperfecta), interventional procedures such as facet joint corticosteroid injections [33], percutaneous rhizotomy, electrocoagulation and/or surgical denervation of the involved facet joint, and ultrasound-guided neural blocks can be considered [4]. Early studies also demonstrate that combined therapy, such as exercise and steroid injection, show significantly increased benefit when compared to single method treatment options [39].
Other potentially effective but understudied treatment options include monitoring of posture with avoidance of hyperlordosis of the lumbar spine while sitting and sleeping decubitus with flexion at the thoracolumbar junction. Both may be helpful to decompress either the thoracolumbar facet joints or the fibro-osseous tunnel. Several variations of pelvic tilt exercises which attempt to decompress the thoracolumbar facets by changing the distribution of muscle tone, may also prove beneficial. A number of studies have demonstrated positive benefit with surgical release of the superior cluneal nerve, in refractory cases non responsive to conservative rehabilitation strategies, who have a positive response to the diagnostic block at the iliac crest of the superior cluneal nerve [12, 13, 14, 27].
Conclusion
Maigne Syndrome is an under-recognized cause of low back pain. It can be mistaken for other causes of low back pain and misdiagnosis delays effective treatment and may lead to inappropriate management. Diagnosis requires a focused clinical history and physical examination. The role of medical imaging investigations in Maigne Syndrome is often limited. Ultrasound imaging may be helpful to determine if there is superior cluneal nerve impingement in the peripheral variant and imaging is used to guide diagnostic nerve blocks. Ideally, treatment should be both site-specific and multimodal, targeting either the central variant or peripheral variant while optimizing aerobic fitness, posture, core strength, muscle tone, and fascial tension. Surgical release is reserved for cases when conservative therapy is ineffective or constrained by pre-existing conditions. Fully understanding the varied symptomatology of Maigne Syndrome, knowledge of the complex thoracolumbar junction and the superior cluneal nerve anatomy that contributes to disease, and awareness of the many available treatment strategies are important for successful diagnosis and treatment [38, 40].
Footnotes
Conflict of interest
None to report.