
Abstract
BACKGROUND:
Total knee arthroplasty (TKA) is one of the most common orthopaedic surgical procedures in the advanced stages of knee arthritis.
OBJECTIVE:
The purpose of this study was to define the sex differences in the Turkish population’s morphological measurements of the distal femoral and proximal tibial surfaces that form the knee joint and to compare their compatibility with conventional prosthetic implants commonly used in TKA for advanced-stage knee arthritis.
METHODS:
Anthropometric data for a total of 240 knees from 240 patients were measured using 3-dimensional computed tomography (3D CT). All morphological data were compared with the dimensions of four conventional knee prostheses commonly used in Turkey.
RESULTS:
A comparison of the four tibial components revealed that the majority of female proximal tibias matched with smaller-sized tibial components, whereas those of males matched the larger sizes. Comparing the morphological data with similar values for the four femoral components currently used in Turkey, we found that all the prostheses had similar values.
CONCLUSION:
The four conventional prosthetic brands included in this study matched the distal femoral dimensions of both sexes. On the other hand, we need smaller size tibial components for our female population.
Keywords
Introduction
The knee joint is one of the most complex joints of the human body and requires high functional capability. It is quite common that as the mean age of society increases, knee joint arthritis increases. A number of medical and non-invasive conventional treatment modalities have been used for the treatment of joint aging which is called arthritis. Total knee arthroplasty (TKA) is one of the most common orthopaedic surgical procedures in the advanced stages of knee arthritis. In TKA, proper sizing of femoral and tibial implants is essential to bring bone composition and load transfer to the most appropriate level, which is also of vital importance for the stability and life span of the implant [1, 2, 3].
In TKA, the use of components smaller than actual size during surgery causes subsidence whereas the use of component larger than actual size leads the overhanging part to cause soft tissue damage and pain. In addition, not only the incompatibility of the size of the implant involved, but also its shape can also cause problems in terms of postoperative range of motion and function. In an optimal implant placement, components must match properly to the bone wall [3, 4].
A clinical study has reported that the anatomical profiles of Asian knees were smaller than those of the Caucasian, and suggested that the Asian population requires a smaller range of component size for knee replacements [5]. We believe that there are differences not only between genders in Turkish society but also between Turkish society and other societies. The implants used in our clinic are mostly those designed for American and European societies and different views have been put forward so far regarding proper implant selection based on racial and gender differences. Morphological measurements revealed that female knee joints have anterior condyles that are less prominent and more diamond-shaped. Furthermore, women with the same anteroposterior (AP) length have been reported to have a narrower mediolateral (ML) width than men [6]. Therefore, the implants used in TKA should be designed specifically according to different sizes, genders and races. In this study, we aimed to identify morphotype parameter differences of the knee joint between Turkish males and females and to evaluate the appropriateness of the current protheses we have been using in our practices.
Materials and methods
This research was approved by the institutional ethical review board of the University of Health Sciences, Taksim Education and Research Hospital (#2015/87). The study took place from March 2015 to December 2019. We studied the morphology of 240 normal knees (120 male knees, 120 female knees, left or right, as chosen randomly). During computed tomography of the limb, CT scans were selected using a 64-slice CT scanner (Brilliance 64, Philips Electronics Japan Ltd., Tokyo, Japan). Of the individuals who visited our institution with complaints of multi-trauma, those undergoing computed tomography (CT) of the knee joint for diagnosis were considered for enrollment, and of these, 240 patients were randomly selected. Patients with primary knee osteoarthritis, secondary knee osteoarthritis as a result of connective tissue disease (e.g., rheumatoid arthritis), knees with any implants and knee trauma were excluded. Our exclusion criteria was knee injury thus we chose the patients who had multitrauma without knee injury. The cohort included 120 men and 120 women with an average age of 35.3 years (20 to 45 years) and 37.2 years (20 to 45 years), respectively. The average height was 171.8 cm (165.9–180.4 cm) for males, and 158.7 cm (150.7–171.9 cm) for females. The scanning procedure was performed to acquire 1.2 mm computer tomographic (CT) slices from the hip joint to the ankle joint. All images were retrieved on the CT workstation. The region of interest of the tibia and femur were reformatted with 3D reconstruction. The 3D models of the tibia and femur can be rotated, cut, clipped, and measured. Two orthopedic surgeons measured the entire data to secure objectivity against interobserver bias. Each parameter was also measured twice in a randomly selected knee.
Tibial cuts and measurements
We defined the tibial mechanical axis as the line connecting the center of the knee and the center of the ankle [7]. The proximal tibia was cut perpendicular to tibial mechanical axis, 6 mm below the medial aspect of the tibial plateau with a 7
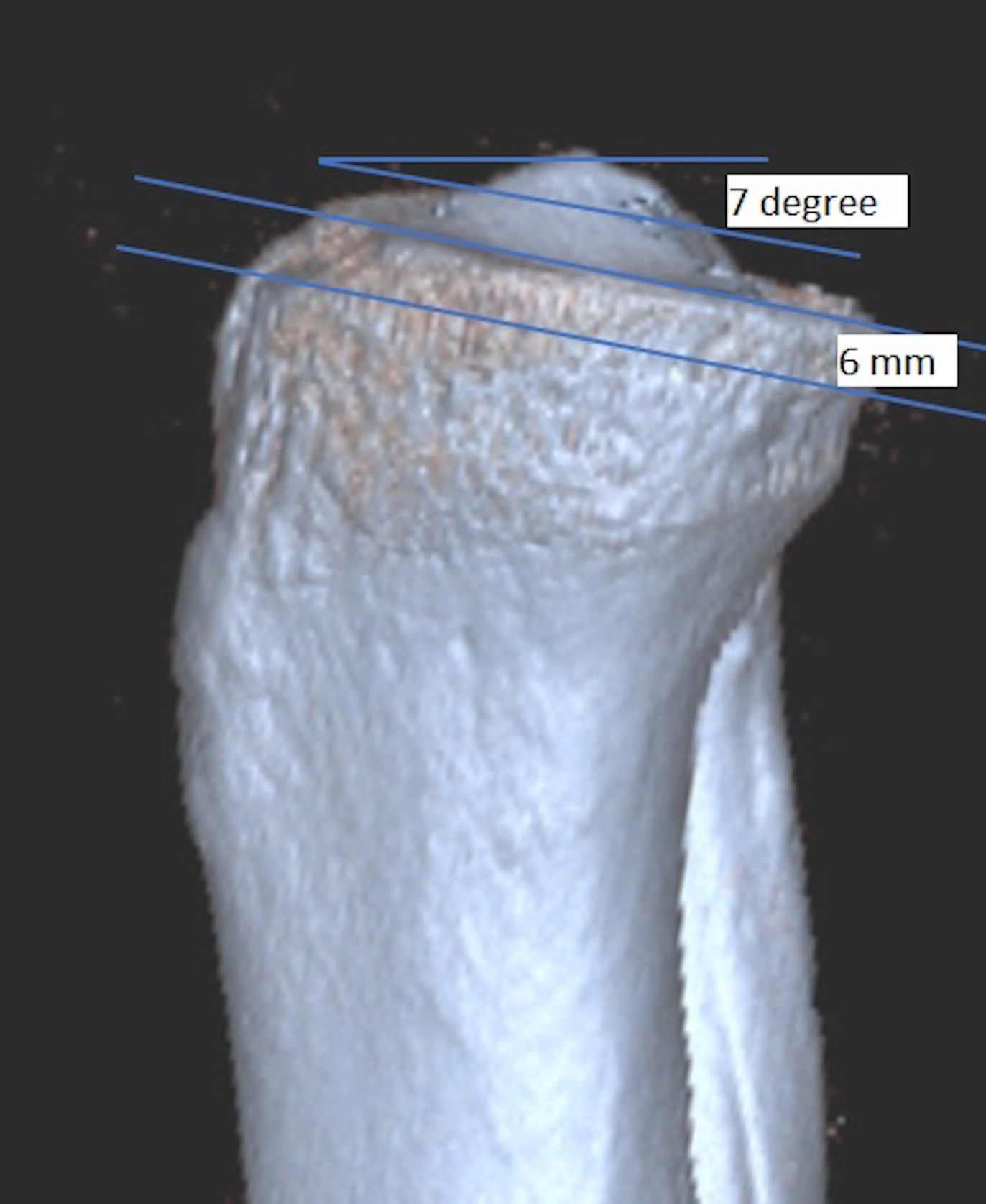
a: The proximal tibia was cut perpendicular to the tibial mechanical axis, 6 mm below the medial aspect of the tibial plateau with a 7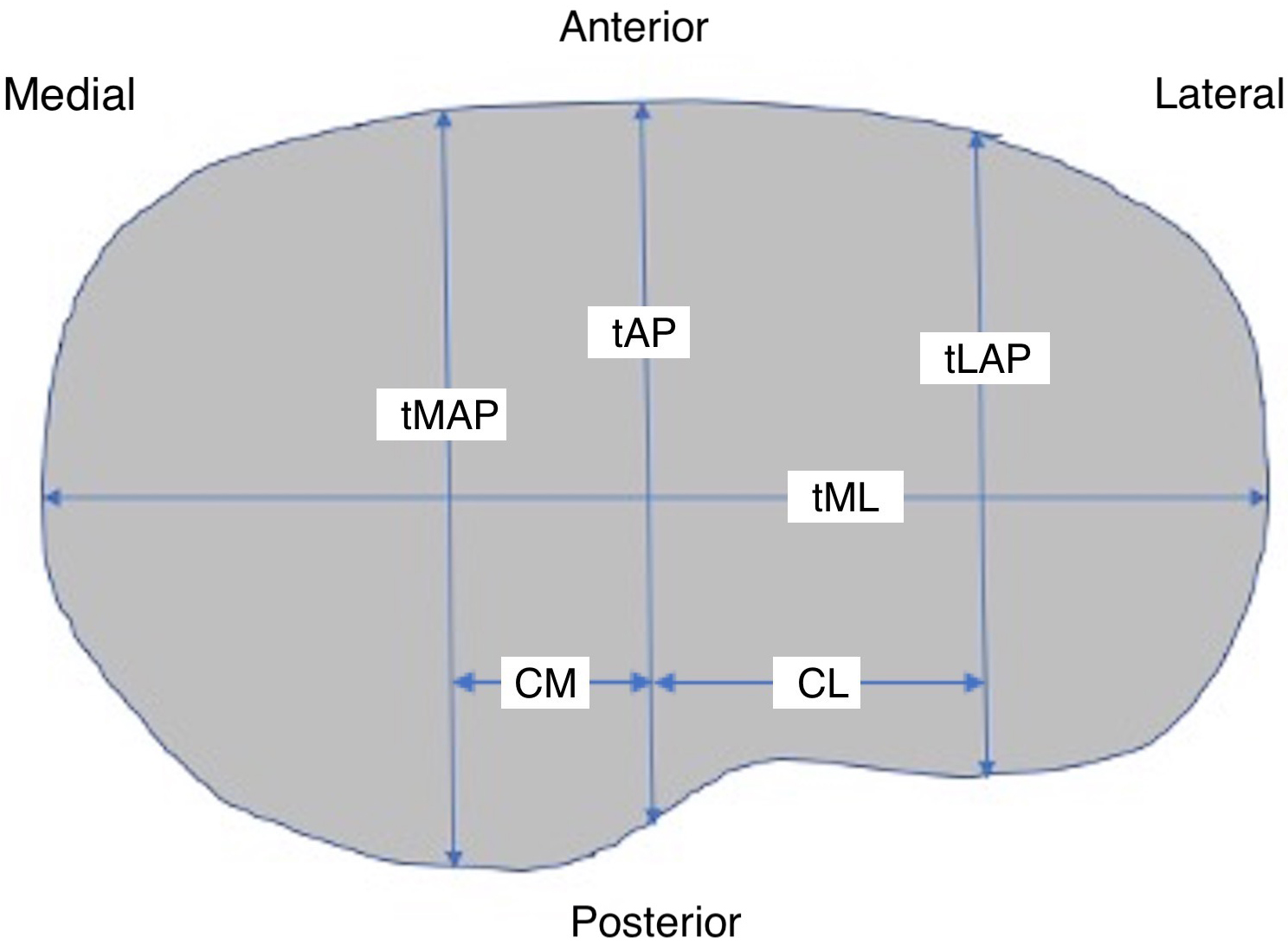
The measurement was made in the axial CT image of the distal femur which was cut 9 mm above the lowest point of the medial condyle with 6
Axial CT image of the distal femur showing the femoral anteroposterior length (fAP), the mediolateral length of the distal femur (fML), the medial anteroposterior length (fMAP), and the lateral anteroposterior length (fLAP).
All measurements were recorded in millimeters using the DICOM imaging software. The anthropometric parameters thus obtained from the tibia and femur were analysed with similar values of prostheses commonly used in Turkey. Four implant types which we used mostly in Turkey, namely Triathlon PS (Stryker, Kalamazoo, MI, USA); Vanguard (Biomet, Warsaw, IN, USA); Anthem (Smith & Nephew Inc., Memphis, TN, USA) and Multigen Plus PS (Limacorporate, Udine, Italy) implants were studied to adjust their ML and AP lengths (MAP and LAP), and ML to AP ratios were calculated. The dimensions of these components were obtained from the manufacturers, and all the available sizes of each component design were used in the analysis.
Average values of the tibia morphology measurements (mm)
A sample size of 240 subjects was determined for this study. This sample size was larger than the table value of 200 (anticipated population proportion – 30%; confidence level
Results
Measurement of proximal tibial morphology
The measurements of proximal tibial dimensions are summarized in Table 1. The average tibial mediolateral (tML) and tibial anteroposterior (tAP) measurements for Turkish knees were 70.6
Tibial medialolateral (tML; mm) and tibial anteroposterior (tAP; mm) dimensions compared with those of four femoral knee prostheses currently used in Turkey (M; male, F; female).
To examine whether the tibial component of the total knee prostheses is suitable for the Turkish population, we analyzed the aspect ratio of the tibia (tAP/tML %). The average aspect ratio of the tibia was 60.6 (Table 1). The aspect ratio showed a definitely positive correlation with tAP. From the relationship between the aspect ratio (tAP/tML %) and tAP, we found that there were large values in the aspect ratio with the larger tAP, and that males had significantly larger values in the aspect ratio than females having the same values for anteroposterior dimension (Fig. 4). The comparison of four tibial components revealed that the majority of female proximal tibias were found to match with the smaller-size tibial components, while the males matched with the larger sizes. A statistically significant number of female knees (
The aspect ratio (tAP/tML %) and tibial anterioroposterior (tAP; mm) dimensions compared with those of four femoral knee prostheses currently used in Turkey (M; male, F; female).
Average values of the femur morphology measurements (mm)
Femoral mediolateral (fML; mm) and femoral anteroposterior (fAP; mm) dimensions compared with those of four femoral knee prostheses currently used in Turkey (M; male, F; female).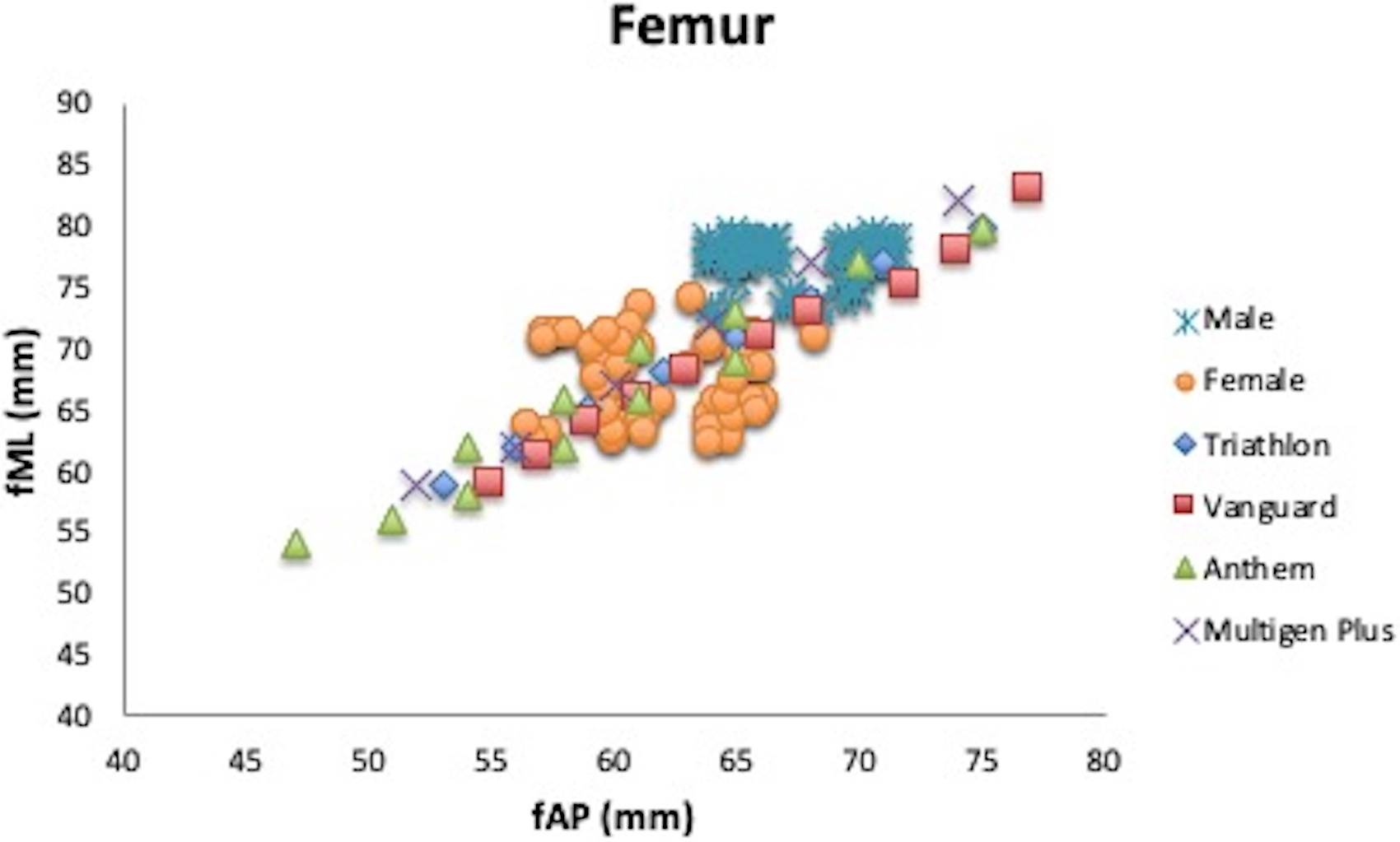
The aspect ratio (fAP/fML %) and femoral anterioroposterior (fAP; mm) dimensions compared with those of four femoral knee prostheses currently used in Turkey (M; male, F; female).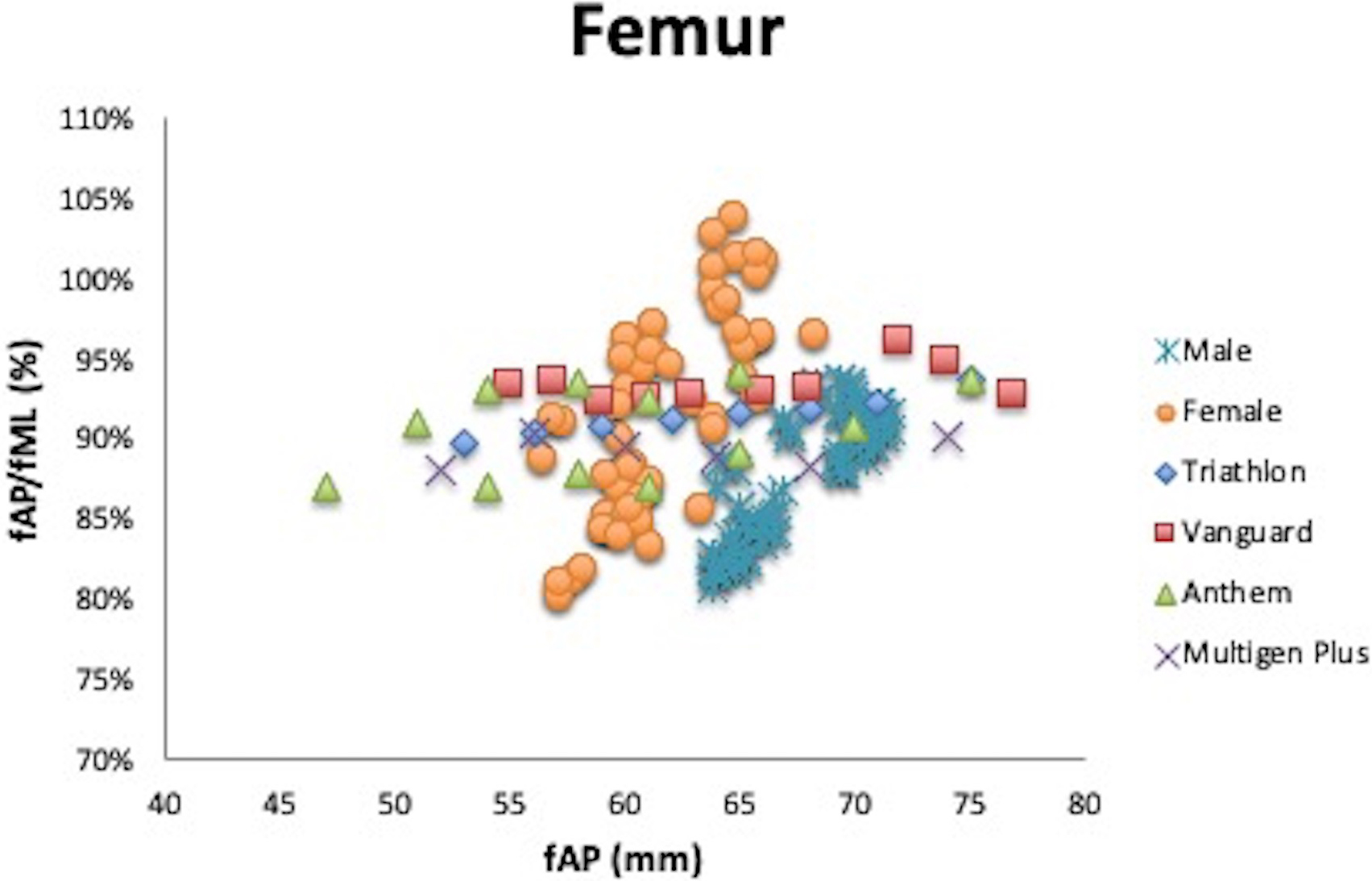
The measurements of distal femur dimensions are summarized in Table 2. The men were found to have large values (
Discussion
Total knee replacement surgery is usually resorted in the end stage of arthritis and its success depends mostly on the technique used, the experience of the surgeon and the compatibility of the implant used with the patient’s knee [14].
In this study, we analyzed morphologic gender differences in Turkish society using 3D CT knee images of 240 patients and the compatibility of the most commonly used four knee protheses with patient knees. Several studies reported differences regarding knee morphology among races [15, 16, 17]. Although not many studies showed the anthropometric differences between Turkish and Western societies, it was demonstrated that they were similar but there were differences between genders [18]. The reason we used 3D CT in this study is that it provides a clear distinction between bone and soft tissue, offers high quality measurement and enables the use of several measurement techniques.
CT analyses showed that females had significantly lower values in both proximal tibial and distal femoral dimensions than males. In our study, as also shown by Kwak et al. [8], the tML length of the female proximal tibial surface was smaller than the male. In addition, males had higher average values than females in distal femoral dimensions. In this study, the evaluation of the parameters in both genders measured showed smaller values than Western societies [19] but similar values to Asian societies [8, 9].
Similar to other reports, we also found that tMAP has larger values than tLAP [8, 10, 19]. Since the medial tibial plateau was larger than the lateral tibial plateau in all our measurements, regardless of any gender differences, the use of asymmetric proximal tibial baseplate appears to be more reasonable. There are several studies which support our views [8, 9], whereas there are several others which do not [4]. On the other hand, a recent study showed no differences in asymmetric and symmetric tibial component design regarding compatibility to the bone [20]. Designing individual and gender specific anatomic prostheses seems to be the most effective solution.
Some studies demonstrated that the morphology of the knee varies between races. For example, Korean and Chinese knees were found to be smaller than Caucasian knees [21, 22, 10, 19]. Besides, several studies suggest that since there are differences between female and male anatomies, standard prostheses are not appropriate to be used for both genders [23, 8, 24]. We believe that tML and fAP measurements should be taken into consideration by the manufacturers while designing patient specific prostheses.
The measurements of the four knee prostheses compared in this study matched morphological data of male knees and distal femoral data of females in Turkish society whereas there were small female tibial datas that did not match even the smallest tibial baseplates in females. Tibial tAP/tML aspect ratios of female patients indicate the need for smaller measurements for tibial prostheses. The fAP/fML aspect ratio matched due to wide size range of the four prosthetic brands as presented in the graphics above. On the other hand, the comparison of male and female data showed that smallest prosthesis lengths matched better for all brands.
This study has several limitations. First, the cohort was relatively young with normal knees, and thus, our results might not be applicable to TKA candidates with degenerative osteoarthritis. Second, the study does not provide post-operative clinical patterns, because it did not target patients who had undergone TKA. Since patients with arthritis in the surgery group present some deformations and subtle shape changes in bones, sizes and coverage of components would be affected, which, however, can be compensated if prosthetic brands have a wide range of sizes. During surgery, since the depth of bone cut may sometimes depend on the severity of bone loss, the level of resection may change. Nonetheless, we believe that the findings of this study provide basic information for the development of knee joint prostheses that match the Turkish morphotype and pre-operative guidelines regarding prosthesis selection. Therefore, prospective studies that record post- resection measurements of patients during surgery could yield more effective results. A strength of our study is that, while most studies were conducted using MRI, we used 3D CT in this study, which enabled us to have a computer program with capabilities of easy identification of bone boundaries, measurement, incision and rotation.
Conclusion
This antropometric study of the knee joint of male and females of Turkish society showed that proximal tibial and distal femoral data of females were much smaller. The four contemporary prosthetic brands included in this study are of appropriate sizes to meet distal femoral measurements of both genders. However, smaller size tibial components are required for female population. We believe that prosthetic technology should be improved so that patient specific prostheses for different societies are designed and thus, size variability is increased and prosthetic match is achieved even in small size joints.
Footnotes
Conflict of interest
The authors declare no potential conflicts of interest with respect to the research, authorship and/or publication of this article.