
Abstract
BACKGROUND:
Myofascial trigger points (MTrPs) in neck muscles seem to be related to the main symptoms of patients with chronic neck pain.
OBJECTIVE:
The objective was to investigate the effects of dry needling (DN) on pain, disability, kinesiophobia, pain catastrophizing and psychological distress in patients with chronic neck pain.
METHODS:
A double blind randomized controlled pilot trial was designed. Twenty-one patients with chronic neck pain were randomly allocated to the DN group (
RESULTS:
The DN group showed a greater decrease in pain intensity, disability and pain catastrophizing compared to the Sham-DN group (
CONCLUSION:
Adding two sessions of DN in active MTrPs in upper trapezius, levator scapulae and sternocleidomastoid muscles to a TENS/US protocol with patient education decreased pain intensity, disability and pain catastrophizing in patients with chronic neck pain.
Introduction
Neck pain is one of the most common disorders in the general population [1]. In most cases it develops into a chronic condition affecting the physical, social and psychological status of the patients [2]. The global prevalence of chronic neck pain has been established in the general population in 2.2% [3].
Chronic neck pain [4] has been closely linked to disability and psychological distress [2, 5]. A central sensitization has been proposed as one of the significant mechanisms that could be related to the psychological distress. Thus, it is important to assess not only the physical function but also the mental state of the patient, which can also play a role [6].
The etiology of chronic neck pain remains unclear and could be caused by the disfunction of various structures in the neck region [7]. Currently, several authors have shown a relationship between chronic neck pain and myofascial trigger points (MTrPs) [7, 8, 9]. In addition, recent systematic reviews have shown the presence of MTrPs in patients with chronic neck pain [10, 11, 12], especially in the upper trapezius muscle [11].
MTrPs are defined as hyperirritable spots in a palpable taut band of skeletal muscle fibers. Active MTrPs provoke local and referred spontaneous pain [13]. The referred pain areas described by Travell and Simons [8] for the MTrPs in upper trapezius, levator scapulae and sternocleidomastoid muscles are similar to the pain described by patients with chronic neck pain. These active MTrPS lead to the development of neck pain and the described physical and psychological dysfunctions suffered by patients with chronic neck pain.
Dry needling (DN) is one of the most common treatments for active MTrPs. The aim of DN is to eliminate or inactivate the MTrP eliciting local twitch responses [14]. A local twitch response is a brisk contraction of a taut band of the skeletal muscle fibers that confirms the presence of MTrPs. Previous studies have shown that the DN treatment of the MTrPs in the upper trapezius muscle [15, 16, 17] or trapezius and levator scapulae muscles [18, 19, 20, 21] is effective to decrease pain intensity and disability in patients with chronic neck pain [15, 16, 17]. However, there is a lack of evidence about the effects of DN in the MTrPs in upper trapezius, levator scapulae and sternocleidomastoid muscles on pain, disability, kinesiophobia, pain catastrophizing and psychological distress in patients with chronic neck pain.
The aim of this pilot randomized controlled trial (RCT) was to evaluate the short-term effects of the DN treatment in active MTrPs in the upper trapezius, levator scapulae and sternocleidomastoid in patients with chronic neck pain compared to a sham DN procedure and a control procedure on pain intensity, disability, kinesiophobia, pain catastrophizing and psychological distress.
Materials and methods
Study design and ethical approval
A double blind (patient and evaluator) randomized controlled pilot trial was conducted. The study was approved by the Clinical Research Ethics Committee of Aragón (PI 20-1773) and was registered at www.clinicaltrials.gov under number NCT04060004. All patients understood the procedures and signed a written informed consent. The study was carried out according to the CONSORT guidelines [22].
Participants
Between September 2019 and February 2020, thirty-seven patients with chronic neck pain were referred by medical doctors to the physiotherapy primary care service in Soria (Spain).
The inclusion criteria were: neck pain for
The exclusion criteria were: history of neck trauma; cervical radiculopathy; acute neck pain; previous surgery in the neck or shoulder area; history of diagnosed primary headache, deformity, infection or malignancy; previous physiotherapy treatment in the last three months; previous experience of the DN technique; DN contraindications such as local infection, bleeding disorders, immune suppression, or significant fear to needles; and inability to understand the instructions.
Randomization and blinding
All participants were randomly assigned to one of the three intervention groups: the DN group, the Sham-DN group or the Control group. An external assistant randomized the participants to the groups using the Research Randomizer (version 4.0) computer software. The randomization list was accessible only to the therapist that applied the intervention. The patients included in the DN and Sham-DN groups and the examiners were blinded to the assigned group.
Outcomes
The primary outcome measure, pain intensity, was recorded at baseline and after the intervention. A 10-cm Visual Analogic Scale (VAS) was used to measure pain intensity, in which 0 represented “no symptoms” and 10 “the most intense pain imaginable”. This scale has shown to be valid and reliable to measure pain intensity [25]. The Minimally Clinical Important Change (MCID) has been stated in 0.8 cm in patients with chronic neck pain [26].
Secondary outcome measures were disability, kinesiophobia, pain catastrophizing and psychological distress. These variables were recorded using the validated Spanish version of the Neck Disability Index (NDI) [27], Tampa Scale for Kinesiophobia (TSK) [28], Pain Catastrophizing Scale (PCS) [29], and Hospital Anxiety and Depression Scale (HADS) [30]. All secondary outcomes were recorded at baseline and after the intervention. After the last treatment session, the self-reported improvement, measured with the Global Rate of Change (GROC) scale, and the success of blinding were assessed.
The NDI assesses neck pain and disability and is composed of a first section related to the intensity of pain, and a second section related to neck disability in daily living activities. Each item rates from 0 to 5 and the total score ranges from 0 (no disability) to 50 (maximum disability). This scale has shown an Intraclass Correlation Coefficient (ICC) of 0.98 [27]. The MCID has been stated between 3.5 to 9.5 points in patients with chronic neck pain [31].
The TSK evaluates fear of movement in patients with musculoskeletal pain. This scale is composed of 11 items. Each item rates from 1 (strongly disagree) to 4 (strongly agree). The total score ranges from 11 to 44, and higher scores indicate a worse health status. This scale has shown an ICC of 0.95 [32]. The MCID has been stated in 5.6 points in patients with chronic pain [33].
The PCS assesses different thoughts and feelings that patients may experience such as rumination, magnification and helplessness. This scale is composed of 13 items. Each item rates from 0 (no negative thoughts or feelings) to 4 (maximum negative thoughts or feelings). The total score ranges from 0 to 52 and higher scores reflect worse patients’ levels of catastrophizing thinking. This scale has shown an ICC of 0.84 [29]. The MCID has been stated in 6.8 points for patients with chronic pain [34].
The HADS measures anxiety and depressive symptoms. This scale is composed of 14 items. Each item rates from 0 (no distress) to 3 (maximum distress). The total score ranges from 0 to 42 and higher scores indicate more severe psychological distress. The cut-off score for the presence of anxiety and depressive symptoms is
The GROC scale assesses the self-reported improvement after the intervention. This scale consists of a 15-points scale ranging from
To test the blinding of the patients included in the DN and Sham-DN groups, a short 3-items questionnaire was used after the intervention. The patients included in the DN and Sham-DN groups were asked about the intervention received. Patients selected one of the three options (DN intervention, Sham-DN intervention or No answer).
Interventions
All interventions were carried out by the same experienced therapist, who was blinded to the measurements and had more than 5 years of clinical experience in the use of DN.
Participants allocated to the Control group received a Transcutaneous Electrical Nerve Stimulation and Therapeutic Ultrasound (TENS/US) protocol [37] with therapeutic patient education in daily sessions from Monday to Friday for two weeks. TENS was applied with an Enraf-Nonius device TENS 911. One electrode was placed on the lateral part of the upper trapezius muscle and the other was placed 5 cm proximal. The frequency was 80 Hz and 150
Flowchart diagram.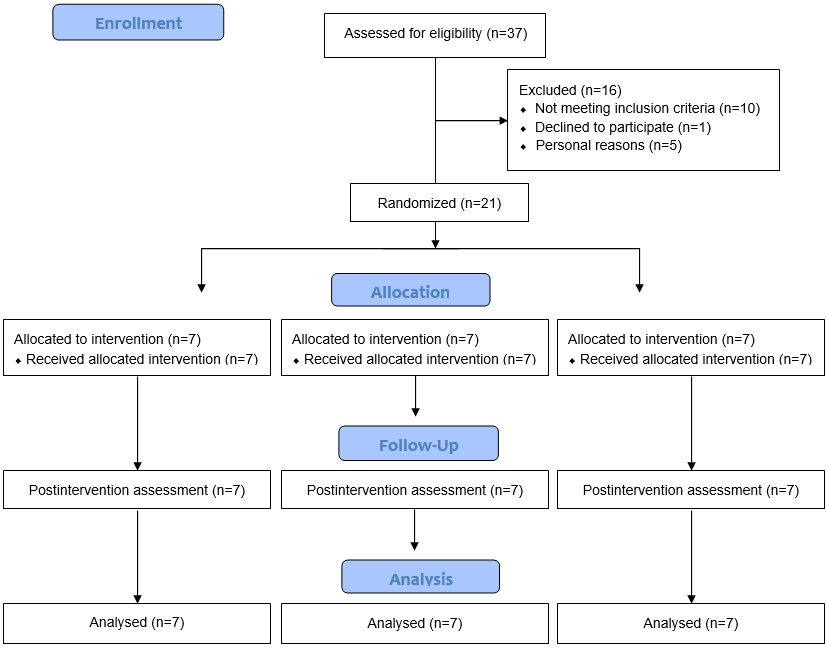
Participants assigned to the DN group received the same treatment protocol as the Control group with the same dose. In addition, two sessions of DN into active MTrPs were added. DN sessions were performed once per week (the second and the seventh days of treatment) according to the findings described by Domingo et al. [40]. At most, three active MTrPs that reproduced the symptoms of the patients were treated in each session, following the protocol described by Ceballos-Laita et al. [41]. The DN technique was performed with single-use stainless needles (0.25 mm
Participants assigned to the Sham-DN group received the same treatment protocol as the Control group with the same dose. In addition, two sessions of sham DN, one per week, were also added in the same regions and with the same procedure as the DN group. The sham DN technique was performed according to the procedure described by Tough et al. [44]. A blunted needle was placed on the MTrP and was pressed up and down against the skin without penetrating, causing a pricking sensation.
Statistical analysis was performed using SPSS version 20.0. Descriptive analysis was presented with means and standards deviations for quantitative variables, and frequencies and percentages for qualitative variables. Normal distribution of the variables was analyzed using the Shapiro-Wilk test. The demographic and clinical variables were compared between groups at baseline using one-way analysis of variance (ANOVA) or Kruskal-Wallis analysis for continuous data according to the normally distributed data or non-normally distributed data respectively, and Chi-square test (X
Results
Thirty-seven consecutive patients with chronic neck pain were screened for eligibility. Sixteen patients were excluded. Twenty-one patients met all the eligibility criteria, agreed to participate, were randomly assigned to one of the three groups, and completed the study. The study flowchart is shown in Fig. 1. Table 1 shows the demographic and clinical details of participants at baseline. There were no statistical differences between groups in any variable at baseline (
Sociodemographic and clinical variables of each group at baseline
Sociodemographic and clinical variables of each group at baseline
Data are mean
Active MTrPs at baseline
Data are
The total number of active MTrPs in the muscles evaluated at baseline are shown in Table 2. According to these clinical findings, there were no statistical differences between groups in the number of active MTrPs located in each muscle. The MTrP1 and MTrP2 of the upper trapezius muscle and the lower MTrP of the levator scapulae were the main muscles treated in the DN and Sham-DN groups.
After the intervention, a two-way ANOVA showed a significant Group by Time interaction for pain intensity, disability and pain catastrophizing (
Primary and secondary outcomes at baseline and after intervention
Abbreviations: DN: Dry Needling; SD: Standard Deviation; CI: Confidence Interval; VAS: Visual Analogic Scale; NDI: Neck Disability Index; TSK: Kinesiophobia scale; PCS: Pain Catastrophizing Scale; HADS: Hospital Anxiety and Depression Scale.
GROC scale.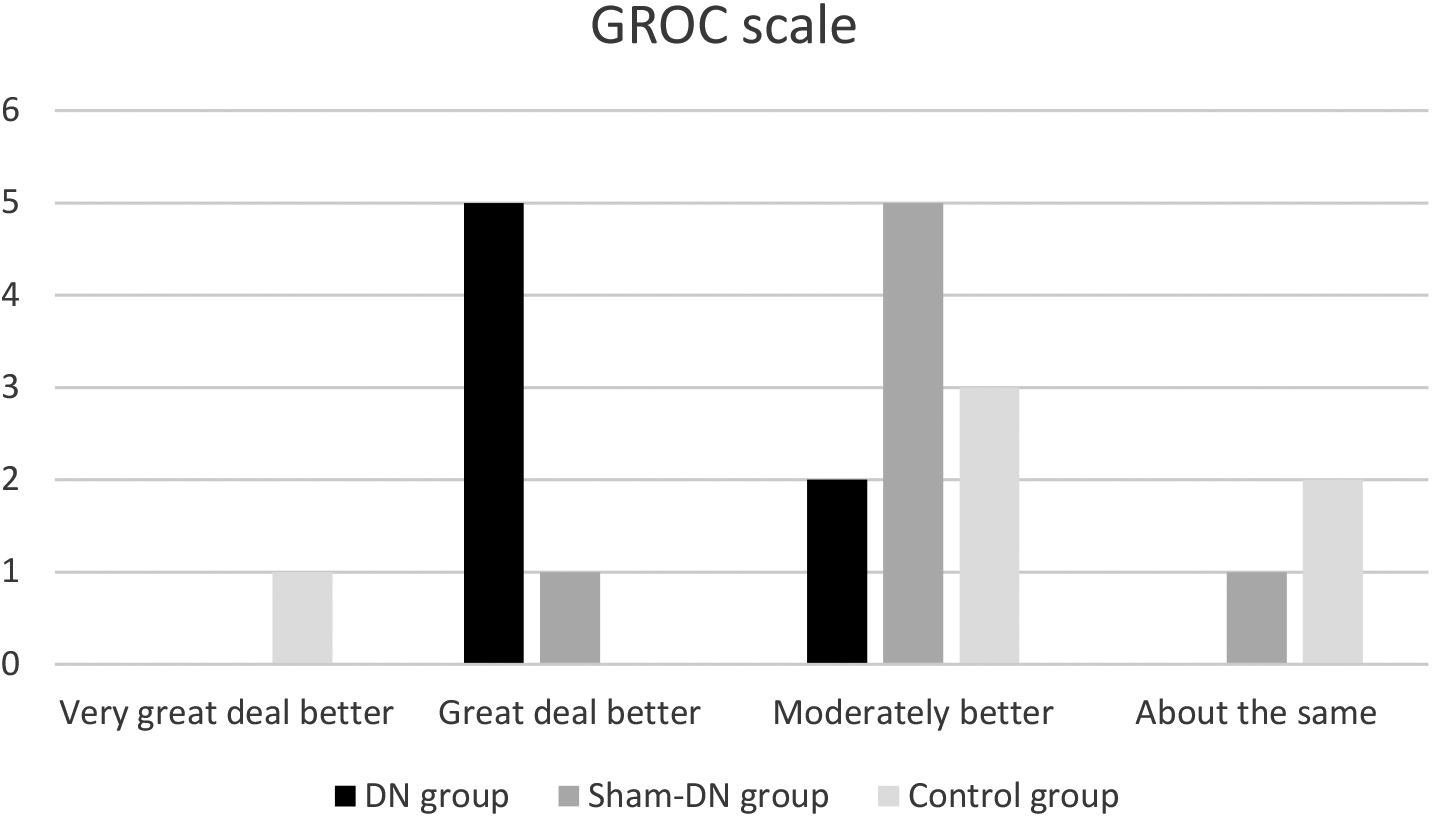
The self-reported improvement, measured by the GROC scale, was categorized as a “great deal better” (
Concerning the blinding, there were no statistically significant differences between the DN and Sham-DN groups (
The sample size was calculated for all dependent variables estimating a two-tailed test, according to the standard deviation and the minimal change between groups obtained in this pilot study. With 80% power, a
Discussion
This pilot study showed that DN in active MTrPs in upper trapezius, levator scapulae and sternocleidomastoid muscles reduced pain intensity, disability and pain catastrophizing statistically significantly compared to sham-DN or control intervention in patients with chronic neck pain.
The change achieved on pain intensity in the DN group was higher than the MCID stated for patients with chronic neck pain [26]. These results are in agreement with previous studies that showed that DN intervention reduces pain intensity in patients with chronic neck pain in the short-term [15, 16, 17, 18, 19, 20, 21]. The higher frequency of MTrPs in upper trapezius and levator scapulae muscles reported in our results agrees with previous studies [45]. Also, the active MTrPs found in the sternocleidomastoid muscle of the included patients evoked referred pain patterns contributing to the neck pain suffered by the patients included in this study. This fact has been reported in a recent study that showed that these three muscles presented a higher stiffness in patients with chronic neck pain compared to asymptomatic subjects [46]. However, this is the first study that has clinically evaluated and treated the MTrPs in the three neck muscles in patients with chronic neck pain. Therefore, the MTrPs in the sternocleidomastoid muscle should be considered in patients with chronic neck pain.
The short-term analgesic effects could be attributed to DN because the implementation of the control group protocol in isolation showed no statistically significant benefits in pain intensity. Previous studies have shown that a single session of DN in MTrPs increases the levels of endogenous opioids, such as
According to our findings, the treatment of the active MTrPs in upper trapezius, levator scapulae and sternocleidomastoid muscles also improved disability, kinesiophobia and pain catastrophizing. The results achieved on disability and pain catastrophizing were higher than the MCID stated for patients with chronic neck pain [31, 34]. Our results are similar to other studies that reported that two [18, 19] to four [15, 20, 21] sessions of DN improved disability in patients with neck pain [15, 18, 19, 20, 21, 48]. However, to the best of our knowledge, this is the first study that has investigated the effects of two DN sessions on kinesiophobia, pain catastrophizing and psychological distress in patients with chronic neck pain.
The changes showed on disability, kinesiophobia and pain catastrophizing could be related to the outcomes achieved on pain intensity. These variables have shown to be strongly correlated to the pain levels in patients with chronic pain [49].
The patients included in the DN group showed the highest self-reported improvement, which was higher than the MCID values. The 71.4% of the patients included in this group achieved large changes, and the 28.6% showed moderate changes. The Sham-DN and Control groups mainly reported small to moderate changes. The GROC scale is an important tool because statistically significant differences could be not directly linked to the perception of improvement of the patient.
Concerning the blinding, most of the patients included in the DN and Sham-DN groups reported having received the DN technique. The outcomes of this study have shown that the non-penetrating technique blinded successfully DN technique in patients with chronic neck pain. Furthermore, the Sham-DN and Control groups showed no statistically significant differences within or between groups in any variable. These results are in accordance with previous studies that showed that sham DN technique did not produce significant changes [50].
This study is not without limitations. The small sample reduced its internal validity, however, the data provided could be used to design future related studies; medium- and long-term follow-ups were not evaluated; the placebo and the DN group only included men, which could be a limitation in the generalization of the results; the Control group could not be blinded to treatment allocation, potentially influencing subjects expectations; patients with MTrPs were included and the outcomes achieved in this study cannot be generalized to other samples of patients with chronic neck pain. Future studies should investigate the medium and long-term effects of DN, as well as its combination with other non-pharmacological conservative treatments in patients with chronic neck pain.
Conclusion
This pilot randomized controlled trial showed that the addition of two sessions of DN in active MTrPs in upper trapezius, levator scapulae and sternocleidomastoid muscles to a TENS/US protocol with therapeutic patient education decreased pain intensity, disability and pain catastrophizing in patients with chronic neck pain.
Author contributions
Conceptualization, LC, MTM, SJ; methodology, LC, MTM, SJ; software, EE, LC, SJ; formal analysis, LC, EE, SJ; investigation, RM, IH, LC, MTM, SJ; resources, RM, IH, LC, MTM, SJ; data curation, RM, IH; writing – original draft preparation, LC, SJ; writing – review and editing, EE, LC, MTM, RM, IH, SJ; visualization, RM, IH, LC, MTM, SJ; supervision, RM, IH, LC, MTM, SJ; project administration, RM; funding acquisition, RM, IH, EE, LC, MTM, SJ. All authors have read and agreed to the published version of the manuscript.
Funding
The study was funded by the Cátedra de Conocimiento e Innovación de Caja Rural de Soria. The funders played no role in the study design, data collection or analysis, the decision to publish or preparation of the manuscript.
Footnotes
Conflict of interest
The authors declare no conflict of interest.