
Abstract
BACKGROUND:
Worldwide, chronic low back pain (CLBP) is one of the most common causes of physical and psychological disabilities. The factors that affect low back pain (LBP) between Western and Eastern countries are different.
OBJECTIVE:
We assessed the factors associated with LBP and their impact in German and Thai CLBP participants.
METHODS:
This cross-sectional study was conducted in 100 Thai and 100 German CLBP participants. Data were collected before the participants received treatment in the outpatient rehabilitation clinic. We used standardized questionnaires to assess the demographic and socioeconomic data, clinical features of the pain, the impact of pain during daily activities, and psychological consequences.
RESULTS:
We found a statistically significant difference between the two groups for minimal pain intensity (NRS German
CONCLUSION:
German CLBP participants had significantly more depressive symptoms and pain-related impairments compared to the Thai participants. On the other hand, there were no differences in maximum and average pain severities.
Introduction
Low back pain (LBP) is one of the most common global health problems [1], and is a major cause of physical and psychological disabilities. The 2015 Global Burden of Disease study found that chronic low back pain (CLBP) was among the top five leading causes of disability in many countries. The worldwide prevalence of LBP was 18.3%; the rates of LBP were high in women, middle-aged individuals, and people from high-income countries [2]. In most cases, LBP is acute and self-limited. However, if the symptoms do not resolve and persist for more than three months, it is considered as CLBP [3].
The global number of CLBP patients is increasing, including in Thailand. The Ministry of Public Health data showed a threefold increase from 2011 to 2015 [4].
Meta-analyses of the last ten years showed a clear association between CLBP and psychological factors, socioeconomic status, and culture [1, 3, 5, 6]. The most striking differences are seen between Western and Eastern countries [7]. In 1990, Brena et al. found that Japanese LBP patients were significantly less impaired by psychological, social, and vocational factors compared to American patients [8].
To understand the impact of socioeconomic and cultural factors on CLBP, comparative studies are needed. A thorough understanding of the underlying factors that influence CLBP will be able to guide health care professionals to provide appropriate treatment to CLBP patients. In Western countries, the biopsychosocial concept of chronic pain is widely accepted [3, 6]. Therefore, multidisciplinary comprehensive pain programs are considered the gold standard of CLBP treatment. However, it is questionable if this concept translates easily into non-Western cultures because there are few studies that have compared CLBP in Western and Asian patients [7, 8].
In our study, we hypothesized that there are differences between German and Thai CLBP patients based on the cultural beliefs and socioeconomic background which can be measured in terms of pain, effect on daily living, and depression.
Materials and methods
Study participants
In this cross-sectional study, two teams of investigators collected data from Thailand and Germany. Thai patients were directly recruited from the Outpatient Rehabilitation Clinic, King Chulalongkorn Memorial Hospital, Bangkok, Thailand. German patients were recruited from the Interdisciplinary Pain Unit of Ludwig-Maximilians-University (LMU), Munich, Germany. This study was approved by institutional ethics committees from both Germany and Thailand. All participants provided written informed consent.
The inclusion criteria were: participants older than 18 years old and non-specific CLBP for more than six months. The exclusion criteria were: severe acute or chronic comorbid disease; systemic or inflammatory musculoskeletal disease; other identified pain generating disease; acute or chronic psychiatric disorder; severe degenerative spine disease with nerve root involvement; acute trauma, fractures, or require surgical treatment; and pregnancy.
One hundred Thai participants and 100 German participants were enrolled into the study. The Thai participants were interviewed, and the data were collected from June 2017 to January 2018. The data of the German participants were collected from their medical records which were self-reported from 2008 to 2016. Missing items in the German questionnaires were considered in the evaluation of our data and normalized with respect to their total score. Both sets of data were collected before the participants received medical service and treatment.
Outcome measurements
The data consisted of four domains of outcomes: 1) demographic and socioeconomic data, 2) clinical features of LBP, 3) impact on daily activity, and 4) psychological factors.
The following demographic and socioeconomic data were collected: age, BMI, sex, marital status, educational level, occupation, and health insurance. As for clinical features of LBP, we collected data related to clinical presentation and previous treatment of LBP. The participants were asked about the duration of pain and intensity of pain using a numerical rating scale (NRS). NRS was used to measure maximal, average, and minimal pain intensity in the last four weeks (10 points indicated severest pain and 0 point indicated no pain at all). Various consultations from several doctors were collected. Previous treatment was assessed using the World Health Organization (WHO)’s analgesic ladder [9]. Furthermore, the participants were asked if their back pain would persist after receiving proper medical care and their acceptable pain intensity following this treatment.
For the domain of impact on daily activity, this was assessed using Pain Disability Index (PDI) [10, 11]. PDI is a tool used to rate the impact of pain in seven aspects of life: family responsibilities, recreation, social activity, occupation, sexual activity, self-care, and life-support activities. Ten points indicated that the disability was the worst and 0 point indicated that there was no disability. The test had a test-retest reliability of 0.91 and Gronblad et al. stated that this test was a reliable assessment tool for disability in LBP patients [12]. The other domain, psychological factors were assessed using Center for Epidemiologic Studies Depression Scale (CES-D). The test included 20 items that screened for depression with a total score of 60. Patients with a higher score have a higher probability of being diagnosed with depression. The CES-D has a reliability of 0.92 [13]. The cut-off value for CES-D was 20 and 22 for Thai and German national treatment guidelines, respectively [13, 14].
Statistical analysis
Statistical analysis was performed using SPSS statistics version 22 (IBM Corp., Armonk, NY, USA). The
Results
The demographic data are presented in Table 1. The mean age of the German participants was 44.8
Baseline demographic data of German and Thai participants
Baseline demographic data of German and Thai participants
BMI, body mass index.
Socioeconomic status of German and Thai participants
The nature of LBP between German and Thai participants
WHO, World Health Organization.
Pain intensity between German and Thai participants
The data of the nature of LBP are shown in Table 3. Most of the participants from both countries had LBP for more than three years (55.51%). Both groups had no significant difference in maximum pain intensity (German
Majority of the participants from both groups believed that the cause of their back pain (Fig. 1) was the result of physical load (79% of German and 67% of Thai participants). The major aggravating factors (Fig. 2) resulted from body posture (
The attributed cause of LBP reported by the participants. 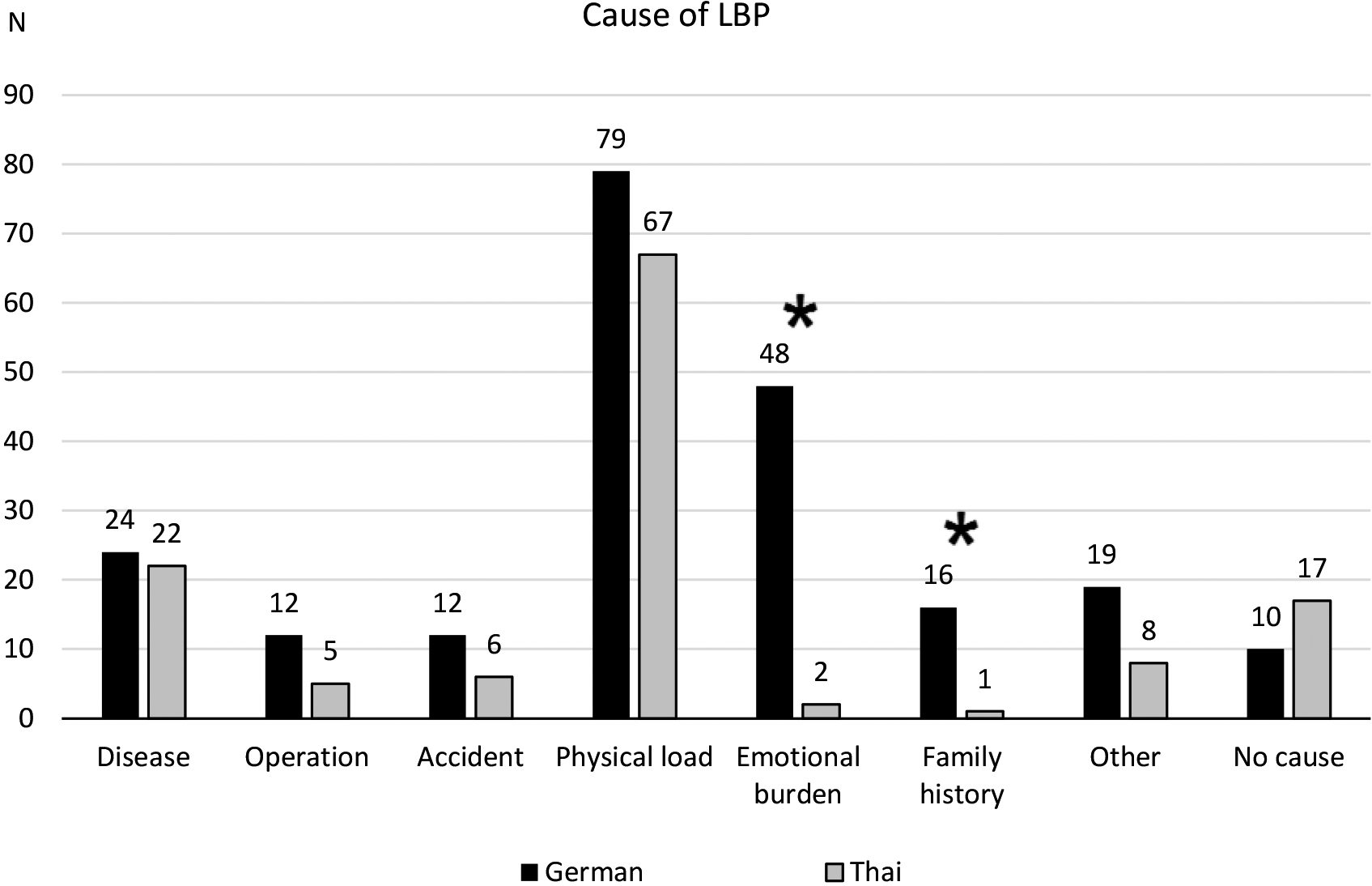
The aggravating factors of LBP. 
The CLBP of the German and Thai participants were different. The German participants had significantly more sick-leave days (13.8
Total score of PDI. 
The score of each item of PDI. 
The total score of CES-D. 
Number of participants at risk for clinical depression. 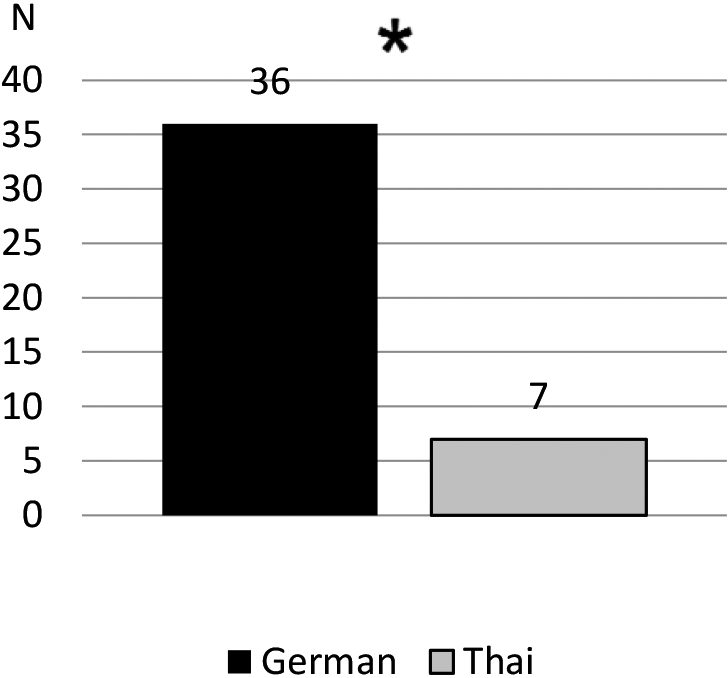
Aside from that, according to the psychological evaluation, we found that German participants (
Our results demonstrated the impact of cultural attitudes towards CLBP among the German and Thai participants. These findings support previous results investigating the influence of cultural differences in chronic pain between Asian and Western countries [8, 15, 16]. In a study by Thong et al., the American group had more depressive symptoms and high CES-D scores compared to the Singaporean group whereas the subjective pain levels were almost identical. This was also observed in our study that the German participants were more psychologically affected compared to the Thai participants. In contrast, in a recent study, Rodrigues-De-Souza et al. found no significant differences in pain intensity, depressive symptoms, and sleep quality between Brazilian and Spanish individuals with CLBP [17]. While these findings seem to differ from the results comparing Asian and Western populations, the religion and cultural beliefs of Brazilian and Spanish people are very similar. Moreover, in our study, according to the PDI scores, the German participants could perform fewer daily activities compared to the Thai participants. This may indicate an overall pronounced functional disability which can result in higher levels of emotional distress in the German participants. In earlier studies by Brena et al. and Thong et al., it was shown that there were similarities in respect to disability between Asian and Western societies suffering from chronic pain. Japanese patients feel vocationally and avocationally less impaired than the American patients [8]. Also, the Singaporeans viewed themselves as less disabled by their pain compared to the Americans [15].
Previous studies have shown that the chronic pain between Asian and Western populations were different due to the cultural factors [8, 15, 16]. Our findings are in line with these reports. A frequently mentioned influencing factor is stoicism which refers to tolerating pain or pleasure without displaying emotion. Stoicism is considered a positive characteristic in Chinese culture [18], and this notion extends to other Asian countries as well [8, 15].
Traditional stoicism in Asian countries may be one of the reason why there is a lower emotional response to pain and better coping skills in the Thai participants. As a consequence of a stoic mentality, displaying emotional reactions in response to pain is less desirable in Asian societies, and pain may therefore be concealed [16].
Compared to Asian countries, pain related dysfunctions are more accepted in the Western societies [8, 19]. In Germany, affected individuals may be more prone to seek attention from their health care professionals, family members, friends and colleagues, expecting others to respond to their situation. Reactions may be in form of emotional, social, or financial support and is considered to be a driving force for chronification [16]. The lower levels in minimum pain intensity over the last four weeks in the Thai group may also reflect psychosocial influences. Since our exclusion criteria excluded people with major pathological conditions, thus, a relatively high resting pain is not likely to be the result of biological origin. The difference in the mentality between both groups could explain the varying response to the question, to which degree the pain levels were acceptable after treatment. The German participants reported a significantly lower acceptable pain intensity (NRS
According to our results, the Thai participants attributed their symptoms predominantly to mechanical factors, while Germans more frequently mentioned psycho-social factors contributed to their pain. In both groups, the majority of the participants attributed their reason for back pain to physical causes, but 48% of the German participants considered psychological factors to be involved in their pain, while only 2% of the Thai participants made that statement. The German participants were more open towards considering psychological confounders to be a part of their pain experience. The Thai participants embraced a more mechanical model of pain experience. These differences may partly be due to the underlying framework that in most industrialized Western societies, the biopsychosocial concept of chronic pain is used, even in primary care settings [20]. The German participants had more than 3-fold as many doctor visits, and by that, possibly had a higher chance than the Thai participants to learn more about the biopsychosocial model from health care experts. Moreover, the participants in Germany were recruited from a specialized pain clinic, while the participants from Thailand were recruited from a hospital, which may have also served the participants as a primary health care facility.
Previous studies support the presumption that cultural factors primarily affect CLBP compared to socioeconomic differences. The studies by Brena et al. and Thong et al. were both conducted in high income countries, Japan and Singapore, respectively [8, 15]. Thailand is considered a medium income country, with a significantly lower GDP and healthcare budget. Nevertheless, our data showed similar findings in response to chronic pain as that seen in Singapore and Japan. Even though there seems to be a consensus about the management of CLBP internationally, the clinical reality often does not reflect the established management, and treatment seems to be frequently independent of the nation’s socioeconomic status/circumstances. Contrary to the recommendation, there is a general overuse of diagnostic imaging and analgesic therapy, and the access to psychological interventions is generally low. In high-income countries, only a few number of patients are initially referred to behavioural therapy whereas in countries with low income, psychological interventions are rare. Because of this, there are high discrepancies between evidence-based guidelines and the general practice. Considering our results, the differences in CLBP management are not primarily related to different healthcare services or financial reasons. Instead, the cultural background may be a more important factor affecting CLBP.
Due to the design of the study, there were several limitations. The data collected from the German participants were collected retrospectively via self-reported questionnaires, while the Thai participants were interviewed by a medical doctor. However, prior to completing the questionnaires, all German participants were diagnosed with CLBP by diagnostic imaging and laboratory tests. Due to the self-reported way of answering the questions, the German participants had no time constraints in completing the questionnaires. As for the Thai participants, the doctor gave the participants plenty of time to answer the questions to reduce the feeling of time pressure.
The cohorts of both populations were not representative for the total population of either country. Both populations were recruited from urban areas and the German participants were selected from a specialized clinic. The demographic and socioeconomic data showed significant differences between the investigated groups. Compared to the German participants, the Thai participants had generally a higher education level which may be due to the study’s location in the urban area of Bangkok and the clinic’s status. A multicentered study collecting data from diverse health care facilities located in both rural and urban regions in Thailand and Germany could have minimized this bias.
In Germany, the data were collected from the participants at an interdisciplinary pain unit of a university hospital. Many of the participants had a long history of low back pain, which was not significantly different than the duration of pain in the Thai group. The German participants had significantly more doctor visits due to their health care system and referrals to medical specialists. In addition, German participants tend to change health care providers often when they feel unsatisfied with their treatment. Unlike the German participants, the Thai participants did not visit their primary or secondary care facilities but came directly to our university hospital which has medical specialists so referrals are not necessary.
Conclusion
Our findings were in line with previous studies that have shown that cultural factors between Western and Asian countries differentially affected how people coped with CLBP even though the pain severity was the same. As a result, we recommend that cultural effects should be considered when designing a comprehensive management and treatment plan for CLBP.
Footnotes
Acknowledgments
This research was funded by a grant from the Rachadapiseksompoch Fund (RA60-094), Faculty of Medicine, Chulalongkorn University, and Erasmus Funding EU international grant program.
Conflict of interest
The authors report no conflict of interest.