
Abstract
BACKGROUND:
Piriformis syndrome (PS) is the common entrapment neuropathy causing buttock pain. Patients are conventionally treated with lifestyle modification, exercise, non-steroidal anti-inflammatory drugs, corticosteroid or botulinum toxin injections. However, some patients may not respond to these conventional treatment methods. Platelet rich plasma (PRP) injection has been shown to be beneficial in various muscular injuries, but its effects have not yet been investigated in PS.
OBJECTIVE:
The aim of this study was to explore the effect of PRP on pain and functional status in patients with PS, and to identify any correlations between clinical changes and demographic features.
METHODS:
A total of 60 patients with PS were randomly separated into two groups (PRP and control groups). All patients received one session of either PRP or saline injection performed under ultrasound guidance. The pain was measured with a visual analog scale (VAS) and Oswestry Disability Index (ODI) scores were noted at three intervals in both groups: before treatment, 1 week after treatment and 1 month after treatment.
RESULTS:
The VAS and ODI scores were improved in both groups. The improvement was more obvious in the PRP group in the first week, and the results were similar for both groups when measured 1 month after the treatment.
CONCLUSION:
Ultrasound-guided PRP injection provided greater improvements in both pain and functional status in patients with PS, starting in the early period after treatment. A repeat injection might be needed for a long-term effect.
Introduction
The piriformis muscle is located below and in the same plane as the gluteus medius muscle in the buttock. It originates from the anterior surface of the sacrum, in the superior margin of the greater sciatic notch, and is inserted to the greater trochanter of the femur. The main function of this muscle is external rotation of the hip, and it contributes to abduction in the flexed hip joint [1]. It has a close relationship with the sciatic nerve, as the sciatic nerve passes under or goes through the piriformis muscle [2]. Piriformis syndrome (PS) is defined as the spasm and/or edema due to overload of the piriformis muscle with repetitive trauma and ischemia, which may result in sciatic nerve entrapment and presents with pain, numbness or tingling in the gluteal region [3]. Mostly, patients are affected in the fourth and fifth decades of life [4, 5]. There is no specific test for this syndrome. The diagnosis of PS is usually obtained from the patient history and the findings of physical examination using provocative tests to elicit pain. Radiological and electromyographic studies might be needed for differential diagnosis, as the symptoms may mimic a herniated disc [4, 5]. Conventional methods for treatment include rest, stretching exercises, non-steroidal anti-inflammatory drugs, physical agents and dry needling. In addition to piriformis stretching, strengthening of the abductor and adductor muscles of the hip should be added to the rehabilitation protocol [6]. In patients with severe or resistant symptoms, corticosteroid or botulinum toxin injections might be performed for the treatment of PS [5, 7]. However, some patients may not respond adequately to conventional treatments, and these methods might be contraindicated in some patients (i.e; hypersensitivity of drugs, uncontrolled hyperglycemia or hypertension for corticosteroids).
Platelet rich plasma (PRP) is defined as the plasma component rich in platelets, which is obtained from centrifugation of whole blood [8]. PRP contains various growth factors, proteins and cytokines which are necessary in the tissue healing process [9]. PRP has been increasingly used in musculoskeletal disorders [10], and it has been reported that PRP may reduce inflammation, thereby reducing associated edema and pain in the injured tissue [11]. As the main purpose of PRP injection is to increase the factors that play role a tissue healing at the injury site, it is important to show that PRP is appropriately delivered to the target tissue and/or distributed to the injured area [11]. Therefore, ultrasound (US) guidance is recommended for PRP injections in the treatment of musculoskeletal disorders [12, 13]. Although PRP injections have been used to treat numerous musculoskeletal disorders, to the best our knowledge, the effect of US-guided PRP injection in patients with PS has not been previously studied. Accordingly, the aim of this study was to evaluate the effect of PRP injection in patients with PS. The study hypothesis was that PRP injection might be an effective treatment method for this condition because of the tissue healing, anti-inflammatory, and anti-edematous effects.
Methods
This prospective, randomized, controlled study included 60 patients with PS aged between 18–60 years who were admitted in the outpatient clinic between April 2019 and March 2020. The diagnoses were derived from patient histories (starts with pain, tingling, or numbness in the buttocks) and the modified FAIR (flexion, abduction, internal rotation) diagnostic test. The FAIR test was performed as follows: First, the patient was positioned supine, and the affected hip (60
The patients were randomly separated into two groups as the PRP group and control group. Each patient was numbered according to the order of admission to the outpatient clinic. A computer program (
T-Lab PRP kit (Bursa, Turkey) was used for the preparation of PRP. A total of approximately 16 ml blood was withdrawn into two tubes. The PRP tubes were centrifuged at 830 G for 5 minutes using a T-Lab centrifuge with swing rotor. After centrifugation, 2 ml plasma rich in platelets, just above the buffy coat was aspirated from each tube using a manual pipette (total 4 ml) (Fig. 1). 4 ml saline was injected to each patient in the control group.
Preparation of PRP.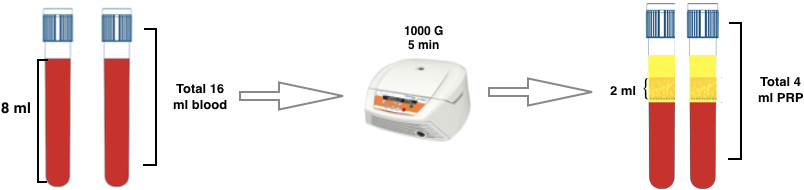
All injections were performed by the same experienced physician under ultrasound guidance. Prior to the injection, the gluteal region was sterilized with chlorhexidine solution. With the patient in the prone position, the US probe was placed over the piriformis muscle, parallel to its long axis (Fig. 2). The physician identified the pirifomis in dynamic US examination with the help of performing internal/external rotation of the patient’s hip joint with flexed knee. A 22 gauge, 90 mm needle was inserted in plane with the US probe and advanced until it reached the piriformis muscle, near to the sciatic nerve. Care was taken to avoid injection into or around the sciatic nerve.
a) Probe position in piriformis injection (patient in prone position); b) ultrasound imaging during injection. P: piriformis muscle, GT: greater trochanter.
The age, gender, body mass index (BMI) and disease duration of all the patients were recorded. The severity of persistent pain and quality of life were assessed before the procedure, and at 1 week after the treatment and 1 month after the treatment. A 100 mm Visual Analog Scale (VAS) was used to evaluate the severity of persistent pain, where 0
Statistical analysis was performed using SPSS software for Windows version 21.0 (IBM Corp Armonk, NY, USA). Data were stated as mean
Of the 85 patients diagnosed with PS, a total of 60 patients who were willing to participate in the study and met the inclusion criteria were included (Fig. 3). All patients completed the study. No side effects were observed in any patient. The demographic characteristics are shown in Table 1. Age, gender, BMI and disease duration were similar in both groups (all
Demographic features of the patients
Demographic features of the patients
Data are given as mean
Flowchart of the patients.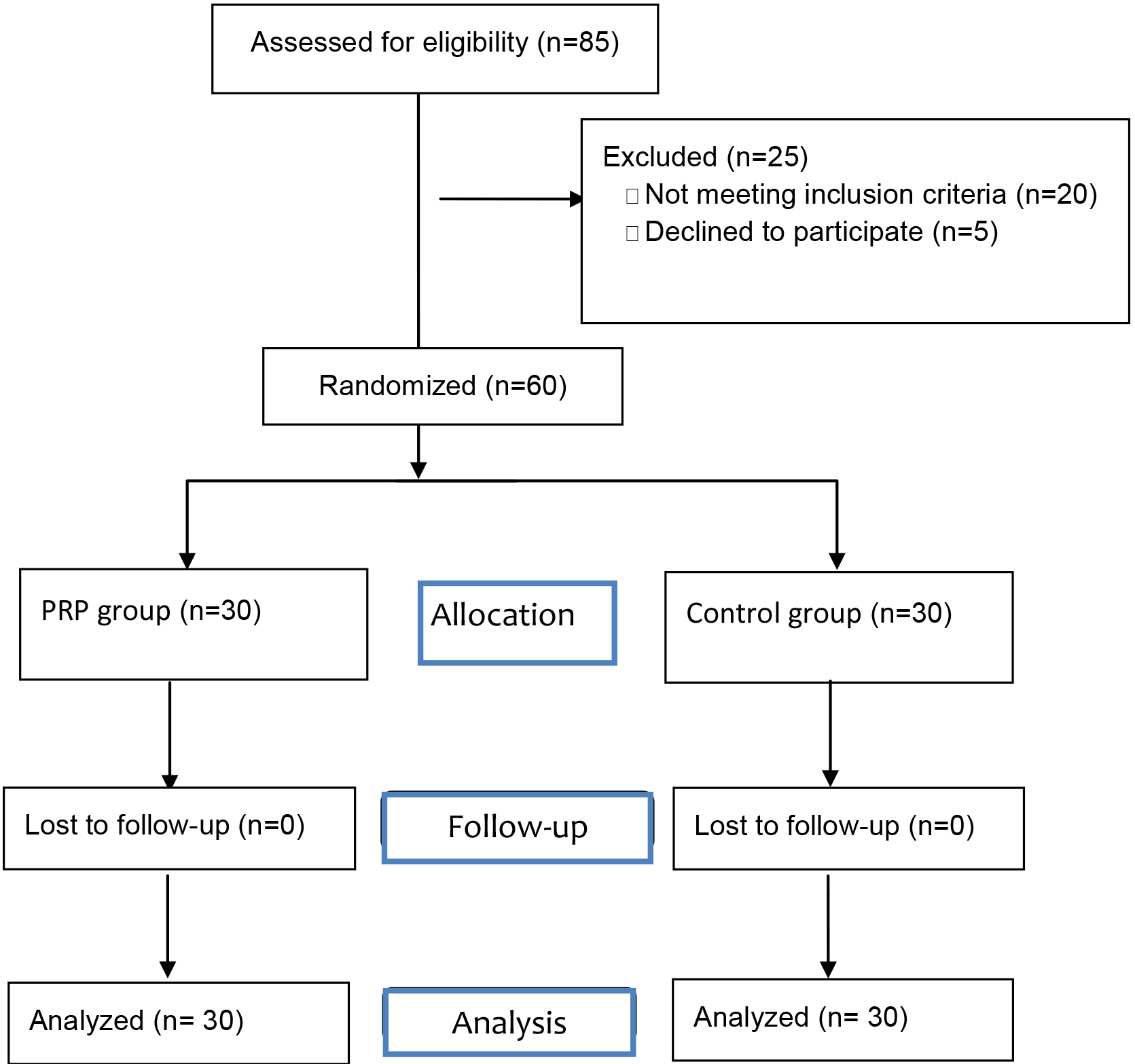
The clinical features of the patients are summarized in Table 2. The VAS and ODI scores were similar before treatment. These scores improved significantly in both groups at 1 week and 1 month after the intervention (
Clinical features of the patients
Data are given mean
The aim of this study was to determine the effect of PRP injection on PS and to compare this with saline injection. According to the findings of this study, both PRP and saline injections improved pain and functional status in these patients. Although this improvement was more prominent in the PRP group in the early period, they were similar in both groups at the end of the first month after treatment. Although the effect of PRP in various musculoskeletal conditions has been previously investigated, to the best of our knowledge, this study is the first that evaluated the effect of PRP in PS.
It has been reported that PRP may contribute to the healing process through several different mechanisms via the secretion of various growth factors including platelet derived growth factor (PDGF), hepatocyte growth factor (HGF), vascular endothelial growth factor (VEGF) and insulin like growth factor (IGF) in an injured muscle tissue [17, 18]. First, it provides improvement of the inflammatory state and reduction of fibrotic scar [19]. Second, it might induce regenerative process of myofibers by increasing satellite cell activation and expression of different myogenic regulatory factors [20, 21]. Furthermore, it may correct the defects of mitochondrial function in myocytes and improve the endogenous antioxidant system [22], and decrease apoptosis in the injured skeletal muscle [23]. It has been reported that PRP injections to the injured muscle tissue are beneficial with regards to more rapid pain relief, and an earlier return to activities without increased risk of re-injury in patients with acute muscle strains [24, 25, 26, 27]. In a previous randomized controlled study, a single PRP injection combined with a rehabilitation program was found to be more effective than a rehabilitation program alone in patients with acute muscle injuries including hamstrings, gastrocnemius and quadriceps [24]. It was shown that adding PRP injection to the rehabilitation program significantly shortened the time to return to activities without increasing the risk of re-injury. In a study of 61 patients with gastrocnemius muscle lesion, the effect of 3 sessions of ultrasound-guided PRP injections was evaluated [25]. At the end of treatment, it was found that PRP combined with an exercise program reduced the time and cost of functional recovery. Consequently, the authors concluded that ultrasound-guided injection of PRP into the site of muscle injury has to be considered a valid therapeutic approach. In a study by Wetzel et al. the effect of a single PRP injection was compared with traditional treatment methods (i.e.: physiotherapy, activity modification, home exercise program, rest and ice massage) in patients with proximal hamstring injuries [27]. The study revealed superior improvements in the PRP group. In the current study, patients with PS were evaluated 1 week and 1 month after PRP or saline injection. When compared to the baseline values, reduction of pain and improvement of function were shown to be higher in the PRP group than in the control group at 1 week after treatment. In this respect, these findings were consistent with previous studies evaluating the effect of PRP in muscle injuries. Therefore, to the best of our knowledge, this study has demonstrated the effect of PRP on pain and functional status in patients with PS for the first time.
Another result of the current study was that despite superior improvements in pain and functional status in the PRP group in the early period, the superiority of PRP injection over saline was not long lasting as there was no difference between the results of the two groups at the end of the first month after treatment. There are two likely causes for this result. First, one of the major causes of PS is repetitive trauma, and the continuation of this trauma may have caused the positive effect of PRP to have disappeared by the end of the first month after treatment. However, the presence of improvement in both groups at 1 month after treatment compared to the pre-treatment values weakens this possibility. The other reason may be the short half-life of growth factors in PRP. Growth factors in PRP are known to have a short half-life (from minutes to hours) [28]. The positive effects of PRP may decrease as the amount of growth hormone released from activated platelets decreases. Therefore, it can be considered that more than one application will have a longer lasting positive effect in these patients.
Mechanical stimulation using a needle causes involuntary contraction of the muscle fibers in a taut band, thereby reducing the concentration of nociceptive substances in the chemical environment near myofascial trigger points. Furthermore, needling may lead to the formation of a small focal lesion that triggers satellite cell migration in the injured muscle. Therefore, the regenerative process is started. The effects of US-guided dry needling in patients with PS have been previously reported [7, 29]. Similarly, in the current study, a significant improvement in pain and functional status was observed in the saline injection group compared to the pre-treatment values. This effect was thought to have been caused by the mechanical stimulation of the needle.
The relatively small sample size and lack of blindness of the patients to the treatment procedure (due to procedure of PRP preparation) are major limitations of this study. Therefore, the placebo effect of PRP could not be evaluated. Another limitation was that the PRP was injected to the patients for only one session which might have impacted the efficacy of the treatment. Nonetheless, the results of this study are noteworthy and important.
Conclusion
The results of this study demonstrated that a single injection of PRP improved pain and functional status in patients with PS in the early period after treatment. It can be used as a new and promising therapeutic approach in the treatment of patients who do not respond to conventional treatment and for whom these treatments are contraindicated. These results need to be confirmed in future studies with larger samples, interventions of more than one session, and placebo controlled studies.
Footnotes
Conflict of interest
None to report.
Funding
T-Lab provided the PRP kit and centrifuge device.