
Abstract
BACKGROUND:
The effectiveness of side-sling plank (SSP) exercises on trunk and hip muscle activation in subjects with gluteus medius (Gmed) weakness is unclear.
OBJECTIVE:
To quantify muscle activation of the rectus abdominis (RA), external oblique (EO), erector spinae (ES), lumbar multifidus (LM), Gmed, gluteus maximus (Gmax), and tensor fasciae latae (TFL) during SSP with three different hip rotations compared to side-lying hip abduction (SHA) exercise in subjects with Gmed weakness.
METHODS:
Twenty-two subjects with Gmed weakness were recruited. SHA and three types of SSP exercises were performed: SSP with neutral hip (SSP-N), hip lateral rotation (SSP-L), and hip medial rotation (SSP-M). Surface electromyography was used to measure the activation of the trunk and hip muscles.
RESULTS:
The trunk and hip muscles activations were generally significantly higher level during three SSP than SHA. SSP-M showed significantly lower EO activation while significantly higher ES and LM activation than SSP-L. Gmed activation was significantly higher during SSP-M than during SSP-L. TFL activation was significantly lower during SSP-M than during SSP-N and SSP-L.
CONCLUSIONS:
SSP could be prescribed for patients who have reduced Gmed strength after injuries. Especially, SSP-M could be applied for patients who have Gmed weakness with dominant TFL.
Introduction
During functional lower-extremity activities, the gluteus medius (Gmed) plays an important role in controlling femoral adduction and pelvic frontal plane alignment [1, 2]. Gmed weakness is associated with abnormal balance, gait, running, and lower-extremity joint pathologies [2]. Previous studies have examined the several exercises for activating Gmed, such as side plank, single-limb squat, forward lunge, lateral step-up, side-lying hip abduction (SHA), and hip clam exercise [3, 4, 5, 6]. Among these exercises, side plank exercise, or side bridge exercise showed the highest-level of Gmed activation in healthy subjects [6]. In addition, side plank exercise is a weight-bearing exercises that better replicate the functional activities of daily living than nonweight-bearing exercises [7].
However, the relative activation of synergist muscles, such as the tenor fasciae latae (TFL) and quadratus lumborum, should be considered when performing exercises focusing on Gmed muscle activation [7]. For example, repeated compensatory activation of the TFL for a weak Gmed can lead to pain in the hips, lower back, and knee [8]. Therefore, previous studies investigated several interventions for preventing compensatory movement or muscle overactivation. Cynn et al. reported that lumbar stabilization leads to reduced lateral pelvic tilt during SHA exercise in healthy subjects [9]. Lee et al. reported that hip medial rotation during SHA showed a higher ratio of Gmed/TFL muscle activation than neutral hip or hip lateral rotation in subjects with Gmed weakness [10]. Monteiro et al. reported that the ratio of Gmed/quadratus lumborum was significantly higher with hip medial rotation than with hip lateral rotation during standing pelvic drop exercise in healthy subjects [11].
An individual’s body weight can provide resistance when performing sling-based exercises [12]. Closed-kinetic-chain exercises, such as sling-based exercises, also provides joint stability by generating co-contraction of several muscle groups [13]. Previous studies have demonstrated that unstable support provoked by suspension devices causes neuromuscular stimulation, which is helpful for recovering normal movement patterns and muscle strength during sling-based exercises [14, 15]. Therapeutic sling and similar exercises can also activate local spine stabilizers, such as the core muscles, without pain or muscle compensation [12, 16].
However, the effectiveness of side-sling planks (SSPs) on trunk and hip muscle activation in subjects with Gmed weakness is unclear. Therefore, this study aimed to 1) quantify muscle activation of the rectus abdominis (RA), external oblique (EO), erector spinae (ES), lumbar multifidus (LM), Gmed, gluteus maximus (Gmax) and TFL during three SSP exercises compared with SHA; and 2) determine the effect of hip rotation in the transverse plane on trunk and hip muscle activation during SSP in subjects with Gmed weakness. Our hypotheses were as follows: 1) the tested muscles except TFL would produce more activation during the three SSP exercises than during SHA and 2) SSP with hip medial rotation (SSP-M) would produce higher activation of the Gmed and Gmax muscles than SSP with neutral hip (SSP-N) or SSP with hip lateral rotation (SSP-L).
Methods
Study design
This was a cross-sectional study. The independent variable was the type of exercise, and dependent variable was muscle activation of the RA, EO, ES, LM, Gmed, Gmax and TFL.
Subjects
The current study included 22 subjects (12 men and 9 women) with Gmed weakness (mean
Subjects with Gmed weakness, no history of lower extremity injuries, such as sprains or fractures, and ability to maintain the exercise position for 5 seconds without any pain were included in this study [10]. A manual muscle test was performed to confirm Gmed weakness. The subjects were instructed to lie on their side on the treatment table. The non-test leg (bottom leg) of each subject was flexed for comfort and stability, and the test leg (upper leg) was aligned with the trunk. The test leg was abducted to 50% of the full range of motion, and the investigator’s hand was placed 10 cm proximal to the lateral femoral epicondyle. An isometric hold for 5 s was performed. Verbal cues were provided to maximize the subjects’ performance, avoiding hip flexion, hip medial rotation, and pelvic hiking of the upper leg caused by the TFL or quadratus lumborum [10]. If bilateral Gmed weakness was present, the weaker leg was measured (right side: 19 subjects, left side: 3 subjects). The weaker leg was defined as the leg with lower performance in the manual muscle testing.
Subjects with past or present musculoskeletal, cardiopulmonary, neurological diseases, inflammatory arthritis, back pain, upper and lower extremity dysfunction [8], shortness of TFL (hip adduction
Instrumentation
An electromyogram (EMG) (Noraxon TeleMyo DTS Wireless System; Noraxon, Scottsdale, AZ, USA) was used to measure the activation of the RA, EO, ES, LM, Gmed, Gmax, and TFL muscles during SHA and the three SSP exercises. The sampling rate was 1500 Hz. A digital band-pass filter, between 20 and 450 Hz, filtered the raw signals, and the root-mean-square values were calculated with a moving window of 50 milliseconds. Myo-Research Master Edition 1.06 XP was used to analyze the EMG data.
A MyoMotion (Noraxon, Scottsdale, AZ, USA) three-dimensional (3D) motion analysis system was used to calculate hip rotation during the three SSP exercises and hip abduction during all exercises. The system also monitored compensatory movement (trunk or hip rotation in the sagittal plane, frontal plane, and transverse plane) during all exercises. A small inertial measurement unit (IMU) sensor placed on a body segment tracked the 3D angular orientation. Three IMU sensors were attached to the pelvis (between the posterior superior iliac spines) and anterior region of the both thighs. The sampling frequency was 200 Hz, and the Myo-Research 3 software was used to analyze the 3D motion data.
Procedures
Before the experiment, subjects jogged at a submaximal speed for 5 minutes as warm-up to reduce discomfort or pain while performing the exercises [19]. They were then familiarized with the exercises and equipment such as pressure biofeedback unit (PBU) until they demonstrated the ability to perform the exercise precisely.
The SHA was performed first, and then the three SSP exercises were performed. The sequences of the three SSP exercises were randomized with random numbers generated in Excel (Microsoft Corp., Redmond, WA, USA). All exercises were performed at a comfortable speed. EMG data were collected for 5 seconds during the isometric phase and were calculated from the average of the middle 3 seconds of each exercise to reduce any starting or ending effect or skin-electrode connecting element [20, 21]. The mean values were used for statistical analysis.
Side-lying hip abduction. Subjects were required to assume a position with the non-test leg (bottom leg) contacting a treatment table with the pelvis, and the test leg (upper leg) was aligned in a straight line with full knee extension. The non-test leg was flexed at the hip and knee joints at 45
Side-lying hip abduction.
Side-plank using a sling with neutral hip. Subjects were positioned on their side on the treatment table with the test leg (bottom leg) contacting the treatment table first, and then both legs were suspended on the sling by the principal investigator (SMB). The narrow sling was positioned at the knee joint of the test leg, and the height of the narrow sling was placed at the perpendicular line drawn across the upper shoulder and the foot of the test leg. Thus, the subjects lifted their hips off the table by abducting the test leg until the spine was in neutral position while abducting the non-test leg (upper leg) until the distal tibia touched the target bar, maintaining the position for 5 seconds, and then slowly returned to the starting position. The target bar was placed at 20% of the maximal range of hip abduction motion to prevent compensation by activation of the hip adductor of the non-test muscles. The subjects were asked to maintain their neck, shoulder, spine, pelvis, and hip joints in a neutral position and put their hands on their shoulders by crossing their arms over the chest during the exercise (Fig. 2). If the pelvis and hip joint deviated by more than 5
Side-plank using a sling with neutral hip.
Side-plank using a sling with lateral hip rotation.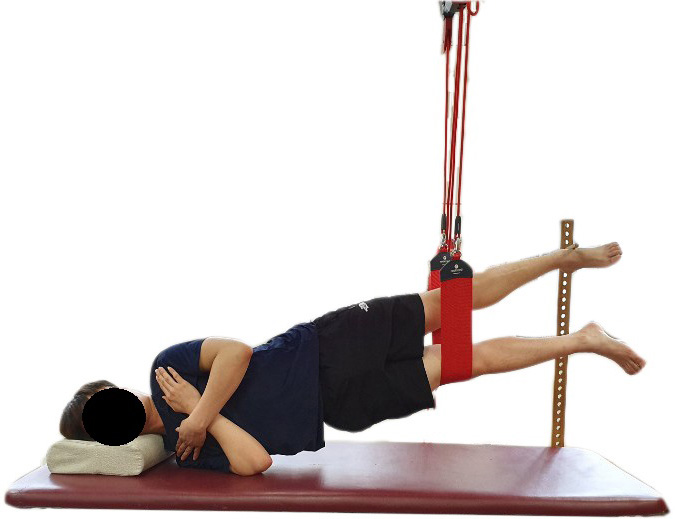
Side-plank using a sling with hip lateral rotation. SSP-L was performed in the same way as SSP-N except for a hip lateral rotation of the test leg (bottom leg) at approximately 50% of the maximal range of motion (Fig. 3), which was measured by the Myomotion 3D motion analysis system. If the pelvis and hip joint lost their neutral position or rotated by more than 5
Side-plank using a sling with hip medial rotation. SSP-M was performed in the same way as SSP-N except for hip medial rotation of the test leg (bottom leg) at approximately 50% of the maximal range of motion (Fig. 4). The hip medial rotation range was measured using the Myomotion 3D motion analysis system. If the pelvis and hip joint lost their neutral position or rotated by more than 5
Side-plank using a sling with medial hip rotation.
EMG data collection. The same side as that of the Gmed weakness was used for data collection. The electrode sites were prepared by shaving any hair from the immediate vicinity of the muscle belly and cleansing the skin with isopropyl alcohol applied with a sterile gauze pad to reduce EMG signal impedance and to allow for proper electrode fixation [22]. Disposable Ag/AgCl surface electrodes were placed approximately 2 cm apart in the direction of the muscle fibers. Electrodes were placed over the midsection of the muscle bellies and described by Cram et al. and Youdas et al. [23, 24]. Electrodes were placed as follows: for the RA, approximately 2 cm lateral and 3 cm superior to the umbilicus, for the EO, midway between the anterior superior iliac spine and rib cage parallel to the muscle fibers, for the ES, 3 cm lateral to the L3 spinous process, for the LM, 2 cm lateral to the lumbosacral junction; for the Gmed, proximally one-third of the distance between the iliac crest and greater trochanter; for the Gmax, at half the distance between the second sacral spinous process and the greater trochanter; for the TFL, approximately 2 cm below the anterior superior iliac spine.
Comparison of trunk and hip muscles activity (% MVIC) during SHA and three SSP exercises
%MVIC, percentage of maximal voluntary isometric contraction; RA, rectus abdominis; EO, external oblique; ES, erector spinae; LM, lumbar multifidus; SHA, side-lying hip abduction; SSP-N, side plank using a sling with neutral hip; SSP-L, side plank using a sling with hip medial rotation; SSP-M, side plank using a sling with hip lateral rotation.
The maximal voluntary isometric contraction (MVIC) in the standard manual muscle test position was used to normalize the RA, EO, ES, LM, Gmed, Gmax and TFL EMG signals [17]. To obtain the MVIC for the RA, the subjects were positioned supine with a flexed leg, where the subjects performed a curl-up against maximum resistance on the shoulder. To obtain the MVIC for the EO, the position of subjects was the same as that of the RA. The subjects performed an oblique curl-up to the opposite knee while applying resistance to the shoulder. To obtain the MVIC for the ES and LM, the subjects were positioned prone with hands clasped behind their head, where the subjects extended the lumbar vertebra until their thorax was raised from the bed. To obtain the MVIC for the Gmed, the subjects were positioned on their sides with the test leg up and the bottom hip and knee flexed, where the test leg abducted approximately 50% of hip abduction with a slight extension and external rotation of the hip joint against maximum resistance on the ankle. To obtain the MVIC for the Gmax, the subjects were positioned prone with the test leg flexed at 90
Statistical Package for the Social Science ver. 24.0 software (IBM Inc., Armonk, NY, USA) was used for all statistical analyses. A 1-sample Kolmogorov-Smirnov test was used to test the normality of the data distribution. A one-way repeated-measures analysis of variance was used to assess the statistical significance of RA, EO, ES, LM, Gmed, Gmax, and TFL muscle activation during four exercises (SHA, SSP-N, SSP-L, and SSP-M). The level of statistical significance was set at
Results
There were significant differences in the muscle activation of the RA (
A 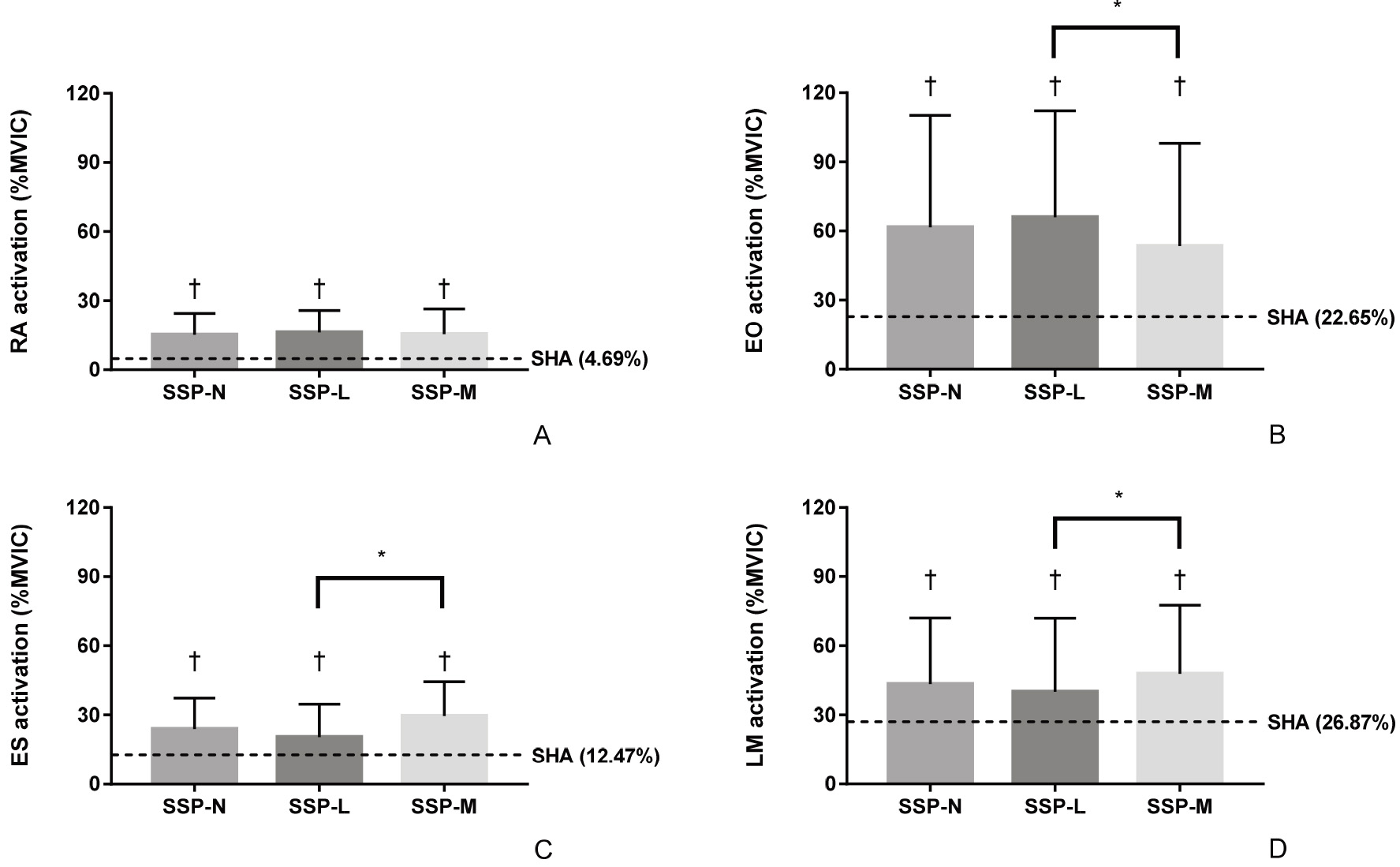
A 
Muscle activation of the RA was significantly lower during SHA than during the SSP-N (
We compared the effects of SHA and the three SSP exercises on the activation of the trunk and hip muscles in subjects with Gmed weakness. The three SSP exercises generally showed significantly higher trunk and hip muscle activation than SHA. SSP-M showed significantly higher Gmed activation than SBUS-L and significantly lower TFL activation than SSP-N and SSP-L. These results partially supported these hypotheses.
The muscle activations of the RA, EO, ES, and LM were significantly higher during the three SSP exercises than during SHA. These results support our first hypothesis. The RA, EO, ES, and LM muscles are stabilizers of the trunk. Performing exercises using a sling can provide an unstable base of support; therefore, the activations of proximal muscles increase to maintain balance [12]. As there is no contact with the floor, the sling also creates an unstable base under multiple conditions; therefore, increased demanded for stability results in higher activation of muscles contributing to trunk stabilization [16].
SSP-M showed significantly lower EO activation than SSP-L. Nakai et al. reported that EO activation was significantly lower with ipsilateral isometric hip internal rotation than with ipsilateral isometric hip external rotation during trunk-stabilizing exercises [26]. They suggested that abdominal muscles were effectively promoted by counteracting the rotation moment acting on the trunk because of the external load on the unilateral lower extremity [26]. Kim et al. also reported that ipsilateral EO showed a greater level of activation than contralateral EO during the single-legged hold on the round foam roll [27]. They explained that the contralateral IO and ipsilateral EO lead to a stable pelvis and spine posture. During SSP-M or SSP-L, lower extremity rotational force was likely to cause rotation moment of the trunk toward the ipsilateral direction. Thus, contralateral EO and ipsilateral IO, as a contralateral rotator of the trunk [28], are required to contract to counteract the rotational moment of the trunk caused by the lower extremity rotation (i.e., ipsilateral EO measured in this study and contralateral IO showed significantly lower activation). The findings of the current study indicate that the decrease in ipsilateral EO can be explained by the same mechanism in previous studies. Ipsilateral EO was reduced, whereas ipsilateral IO may have been activated further to counter-rotate the trunk to maintain the trunk during SSP-M than during SSP-L (the activity of ipsilateral IO was not measured in this study).
LM and ES showed significantly higher activation during SSP-M than during SSP-L. The results of LM activation in this study were also consistent with the results of Nakai et al.’s study [26]. LM activation was significantly higher with ipsilateral isometric hip internal rotation than with ipsilateral isometric hip external rotation during trunk-stabilizing exercise showed [26]. Bilateral LM stabilized the trunk by co-contraction with abdominal muscles [26]. Contraction of the unilateral LM also produces an opposite internal torque with the contralateral EO during spinal axial rotation in the horizontal plane [28]. Therefore, LM activation during SSP-M was promoted to stabilize the trunk by co-contraction with the contralateral EO. ES, as a back extensor and lower trunk rotator when pelvic-on-femoral rotation is occurred [28], also acts as a trunk stabilizer during SSP-M.
Hip muscles activation during the three SSP exercises generally showed significantly higher activation than SHA. SSP-L showed no significant differences in Gmax activation with SHA. These results partially support our hypotheses. During side-plank exercises, the hip abductor muscles contract against gravity and nearly the entire body mass to maintain correct positions, whereas during SHA, the muscles contract against gravity and unilateral lower extremity mass. Abdominal core activation also increases hip muscle activation, minimizing the need for compensatory movements of the lumbar spine and pelvis [29]. Thus, hip muscles showed greater activation level during three SSP exercises than SHA.
SSP-N and SSP-M showed significantly higher Gmed activation than SSP-L. SSP-M also showed significantly lower TFL activation than SSP-N and SSP-L, and no significant difference with SHA. The results of significantly different Gmed and TFL activation among the three SSP exercises agreed with previous studies that investigate the effects of hip rotation during several interventions for strengthening the Gmed [8, 10, 11]. They explained that hip medial rotation is a preferable position to increase Gmed activation because the length and muscle tension of the Gmed can be increased by altering the position of the sarcomeres, whereas hip lateral rotation is favorable for increasing TFL activation. During SSP-M, gravity acts as a hip external rotation resistance, and subjects must internally rotate and abduct the hip to counteract this [30]. The Gmed and TFL act as synergistic muscles during hip abduction. Therefore, increased Gmed activation can lead to decreased TFL muscle activation, and vice versa. However, Gmax and TFL, as a hip lateral rotator and hip medial rotator, have a relationship between the agonist and antagonist in the transverse plane. With reciprocal inhibition, agonist muscle contraction can inhibit the alpha motor neuron of the antagonist muscle. Therefore, higher activation of TFL could lead to lower activation of Gmax during SSP-L.
When selecting an exercise for patient, previous studies suggested that the physical therapist should consider the demands on the muscle and the level of difficulty, and regarding to results, the three SSP exercises might be more difficult than SHA [31]. Myers described a myofascial chain as a tensional force transmitter that controls mechanical communication across all body tissues [32]. The EO, Gmed, Gmax, and TFL are connected through a lateral line, which is a myofascial chains that provides pelvo-femoral stability during functional movements such as single-leg standing, lunge, stair climbing, and gait [32]. Because SSP facilitates multiple joints, deep trunk-stabilizing muscles and lateral line muscles can be strengthened. In particular, the EO, LM, and Gmed activation during SSP-M reached the threshold of 40% to 60% MVIC, which can effectively stimulate muscle strength gains, while the TFL activation was significantly lower than that of SSP-N and SSP-L [33]. Thus, SSP-M may be an effective exercise for subjects of Gmed weakness with dominant TFL by specifically strengthening Gmed as well as trunk muscles.
This study had several limitations. First, this study had a cross-sectional design; therefore, the long-term effects of the three different SSP exercises on trunk and hip muscle activation could not be determined. Second, the ages of subjects were between 20–26 years. Thus, generalization was limited. Lastly, although we took all safety measures, EMG crosstalk was possible between the muscles. Further studies should determine the long-term effects of the three SSP exercises on trunk and hip muscles activation in subjects of all ages with Gmed weakness.
Conclusions
This study investigated the effects of three different SSP exercises on the RA, EO, ES, LM, Gmed, Gmax, and TFL activation in subjects with Gmed weakness. The three different SSP exercises generally showed higher RA, EO, ES, LM, Gmed, Gmax and TFL activation than SHA. In particular, hip medial rotation during SSP resulted in significantly higher ES, LM and Gmed activation than neutral hip or hip lateral rotation and significantly lower TFL activation than hip lateral rotation. Therefore, SSP-M may be an effective exercise to increase EO, ES, LM, and Gmed activation while decreasing TFL activation in subjects with Gmed weakness.
Footnotes
Conflict of interest
None declared.