
Abstract
BACKGROUND:
Due to the anatomical characteristics of the anterior epidural space, dorsal migration of material from herniated lumbar disc is quite rare. Also, bilateral foot drop due to unilateral dorsal migration of disc herniation is extremely rare. This report presents a case of sudden bilateral foot drop caused by the unilateral dorsal migration of material from a herniated lumbar disc.
CASE DESCRIPTION:
A 51-year-old male presented with sudden onset severe leg pain with bilateral foot drop. The patient was referred to our emergency department by a local clinic. Neurological examination showed bilateral ankle and big toe dorsiflexion weakness grade 1. There was no perianal anesthesia, anal sphincter weaknesses, or voiding difficulty. Apart from essential hypertension, this patient’s medical history was unremarkable. Magnetic resonance imaging showed that intervertebral disc material in the dorsal extradural space at the L3-4 level had compressed the dural sac from the left side to the center. We performed an emergency operation. The pathologic result revealed fibrous cartilaginous materials. After the operation, the leg pain was markedly resolved. At postoperative three months, the patient showed improvement of foot drop.
CONCLUSION:
We recommended emergent mass removal, which produced a favorable outcome.
The spinal magnetic resonance imaging (including (A) sagittal and (B) axial image) revealed that a dorsally migrated herniated intervertebral disc (arrow) at the L3-4 level compressed the thecal sac (asterisk) from the left to the contralateral side.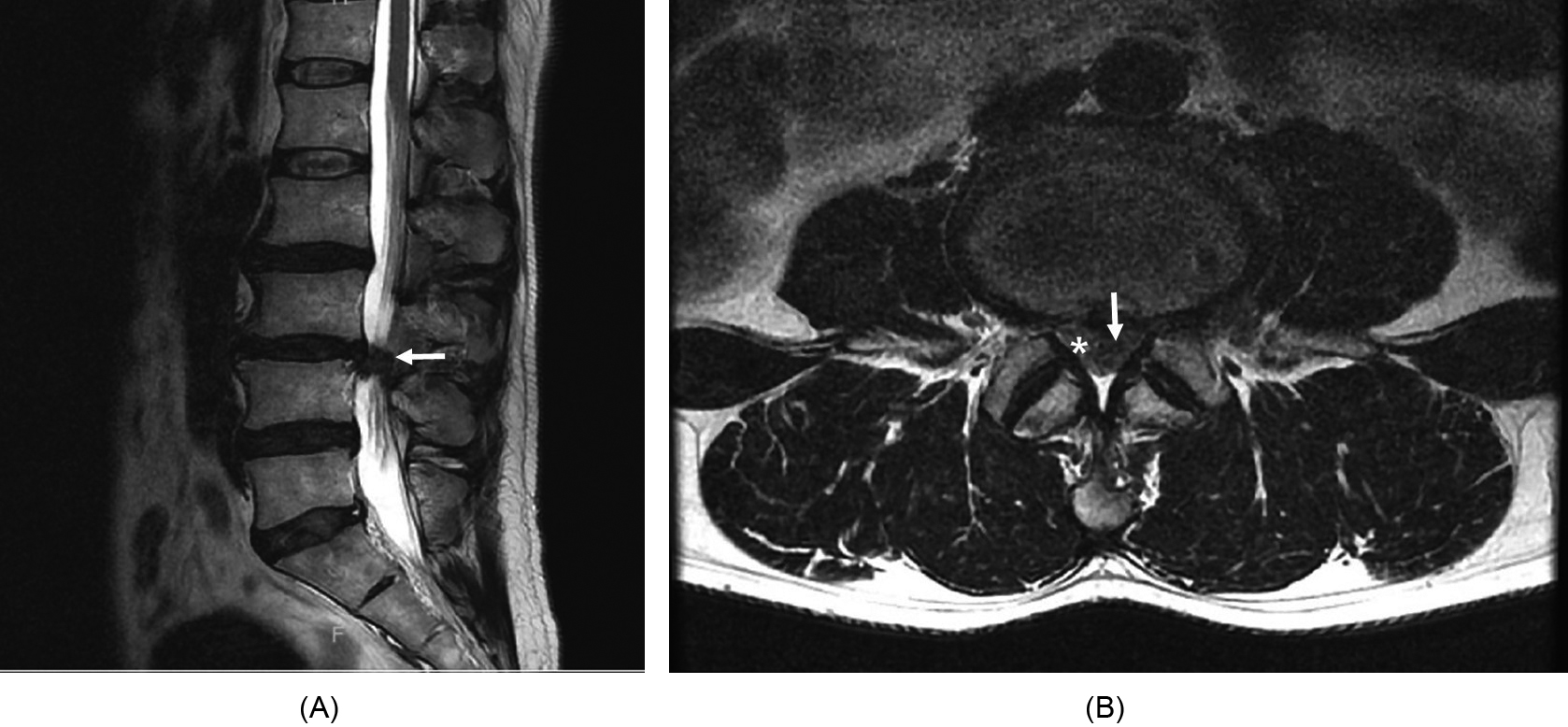
Usually, lumbar disc herniation involves penetration of the annulus pulposus or posterior longitudinal ligament (PLL) by the nucleus pulposus [1, 2]. Due to the anatomical characteristics of the anterior epidural space, the migrated herniated lumbar disc can migrate in upward, downward, or lateral [2] so, the dorsal migration is quite rare [1] and there have been few reported cases [2]. Foot drop results from a weakness of the foot and ankle [3], which makes it difficult to lift the foot as well as the toes. Acute unilateral foot drop due to disc herniation is a well-known condition [4]. However, bilateral foot drop due to unilateral dorsal migration of a herniated disc herniation is extremely rare. This report presents a case of sudden bilateral foot drop caused by the unilateral dorsal migration of a herniated lumbar disc.
Case description
A 51-year-old male presented with sudden-onset of severe leg pain with bilateral weakness of ankle dorsiflexors. The patient was transferred from another hospital to the emergency room two days after onset. Neurological examination showed bilateral positive straight leg raise test [5] and bilateral weakness of ankle and big toe dorsiflexors (grade 1). There was severe pain (Visual Analogue Scale 7) and hypoesthesia at the L5 dermatome bilaterally and a decrease of deep tendon reflex of the ankle. This pain was provocated by leg raising with knee-extended. Muscle power of knee extensors and flexors were grade 5 bilaterally, however, ankle and big toe plantar- and dorsi-flexors were grade 1 bilaterally. There were no upper motor neuron signs such as hyperreflexia, clonus, spasticity, flexor and extensor spasms, and spastic dystonia. The patient did not show perianal anesthesia, anal sphincter weakness and voiding difficulty. Apart from essential hypertension, the patient’s medical history was unremarkable. A complete blood counts, basic metabolic panel, thyroid panel, and nutrient tests for iron and vitamin B one month prior were either normal or negative. He had neither a history of recent surgery nor exposure to toxins or heavy metals. Magnetic resonance imaging (MRI) showed that a mass in the dorsal extradural space at the L3-4 level had compressed the dural sac from the left to the contralateral side (Fig. 1).
The Institutional Review Boards of the Soonchunhyang University Bucheon hospital approved this study (2021-02-004-001). Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Management and outcomes
We performed an emergency unilateral hemilaminectomy and gross total mass removal. To create a wide space for safe removal, we chose wide unilateral laminectomy. After removal of the ligamentum flavum, we observed dorsally migrated herniated intervertebral disc material (arrow) compressing the thecal sac (asterisk) and we performed gross total removal without any neural damage (Fig. 2).
An intraoperative photograph shows (A) compression of the thecal sac (asterisk) by the herniated intervertebral disc material (arrow) gross total removal of disc material, the relaxed thecal sac is visible (B).
The pathologic results revealed a fibrous cartilaginous mass, which suggested intervertebral disc. After the operation, the patient’s leg pain was markedly resolved. However, ankle and big toe plantar- and dorsi-flexors were still grade 1 bilaterally at postoperative 1 day. He was transferred to the department of rehabilitation medicine at postoperative 7 day and started comprehensive rehabilitation including range of motion (ROM) exercise, strengthening exercise and functional gait training. Electrodiagnostic study conducted at three weeks after surgery, which showed bilateral L4, L5 radiculopathy with incomplete axonal degeneration. At discharge, his motor power of the ankle plantar- and dorsi-flexion was grade 4, but big toe plantar- and dorsi-flexors were still grade 2 bilaterally. Three months postoperatively, the patient showed improvement in that the motor power of the ankle and big toe dorsiflexion was grade 4 bilaterally.
The intervertebral disc is comprised of the nucleus pulposus and annulus fibrosus [6, 7, 8]. Migration of fragments herniated lumbar disc is a common phenomenon; theses fragments often move in the cranial, caudal, and lateral directions [9]. Sequestration of a herniated disc fragment is a type of herniated disc migration that accounts for approximately 28.6% of all symptomatic disc herniations [10]. There are three main anatomical structures that preserve the intervertebral disc architecture; the annulus fibrosus, PLL, and Hofmann’s ligaments [11]. Hofmann’s ligaments are fibrous connective tissues that track ventro-laterally from the dura mater to the PLL. Hofmann’s ligaments are generally thick and well-developed in the lower lumbar spine [12] where they provide additional support for the spinal dural sac and secure the vertebral bodies and intervertebral discs [12]. The PLL extends along the posterior surfaces of the body and the intervertebral discs [11]. The ligament in the lumbar and thoracic region presents a widest at the area of the intervertebral disc. The PLL is firmly attached to the annulus, and the lateral part of the Hoffman membrane, the vertebral end-plates, and the vertebral body [11, 13]. The lateral edge of the PLL extends to the lateral wall of the spinal canal [2]. This makes it difficult for a disc to herniate posterior to the dural sac [14]. Because the anatomical structure that preserves the intervertebral disc architecture is very tight and firm in the center of the anterior spinal canal, the dorsal epidural migration of an extruded disc in the lumbar region is relatively rare [9].
Herniated lumbar disc disease produces many symptoms such as radiating leg pain, numbness, dysesthesia, paresthesia weakness, cauda equina syndrome, and so on [2]. L4-5 radiculopathy is the most common cause of foot drop, and is usually caused by disc herniation or foraminal stenosis [3]. Bilateral foot drop is very rare and shows slow progression in many cases. Several diseases and various metabolic conditions can cause bilateral foot drop, unfortunately, the exact pathophysiologic mechanism is not still unrevealed [15, 16, 17]. Huge lumbar disc herniation may cause cauda equina syndrome leading to foot drop. However, foot drop is usually a unilateral, progressive condition accompanied by loss of bowel, bladder, and sexual function [4].
Rapid onset bilateral foot drop is an extremely rare condition [15]. There are few case reports of the bilateral foot drop and these cases mostly had other features of cauda equina syndrome, such as urinary involvement [15]. Oluigbo et al. reported acute bilateral foot drop case due to lumbar spinal stenosis [18]. Mahapatra et al. published acute bilateral foot drop case report due to an intervertebral disc herniation at L3-4 level [15]. This patient also had symptoms of cauda equina syndrome. They performed emergent L3-4 laminectomy and discectomy. The patient showed good recovery.
Rapid growing spinal nerve root compressive lesion may cause a more serious deficit than a slow growing lesion. However, the recovery is more rapid after early decompression in ptientient with rapid growing spinal nerve root compressive lesion [19]. Both patients recovered well after early decompressive surgery. Although we could not estimate the exact pathophysiologic mechanism, in this case, the acute onset of bilateral foot drop was caused by a herniated disk at the L3-4 level. MRI showed that a left dorsal herniated disc mass at the L3-4 level had compressed the dural sac from the left side to contralateral side. Finally, it compressed both side nerve roots, and cause a bilateral neurological deficit. However, there was no perianal anesthesia, anal sphincter weaknesses, or voiding difficulty.
This study is not without limitations. Because this concerns only a case report, it is difficult to conduct a statistical analysis about the improvements of neurological status. In the next study, we will collect some similar cases, conduct a literature review and perform a statistical analysis.
Conclusion
Acute bilateral foot drop by unilateral dorsal migration of herniated lumbar disc material is an extremely rare entity. Emergent lumbar spinal MRI with extension to the lower thoracic vertebrae and early mass removal is recommended and may produce a favorable outcome.
Author contributions
Conceptualization: Hoon Seok, Je Hoon Jeong.
Data curation: Seung Yeol Lee, Dong Seong Shin, Soo Bin Im.
Investigation: Seung Yeol Lee, Dong Seong Shin, Soo Bin Im.
Supervision: Je Hoon Jeong.
Visualization: Hoon Seok.
Writing-original draft: Hoon Seok, Je Hoon Jeong.
Writing-review and editing: Hoon Seok, Seung Yeol Lee, Dong Seong Shin, Soo Bin Im, Je Hoon Jeong.
Availability of data
All data generated or analysed during this study are included in this article.
Funding
This work was supported by the Soonchunhyang University Research Fund.
Footnotes
Acknowledgments
This document has been checked by at least two professional editors, both of whom are native English speakers.
Conflict of interest
The authors have no conflicts of interests to disclose.