
Abstract
BACKGROUND:
One of the main problems faced by physiotherapists in primary care is low back pain with or without radiation to lower limbs. There are many different treatment approaches for the management of low back pain. Despite the large amount of published studies, the evidence remains contradictory.
OBJECTIVE:
To evaluate the influence of the osteopathic manipulation of the sacroiliac joint on low back pain with or without radiation to lower limbs.
METHOD:
Single-blind randomized clinical controlled trial. Participants with low back pain with or without lower limb radiation were randomized to osteopathic manipulation of the sacroiliac joint group (intervention, 6 sessions) or to an electrotherapy group (control, 15 sessions) for 3 weeks. Measures were taken at baseline (week 0) and post-intervention (week 4). The primary outcome measures were pain (Visual Analogue Scale), functional disability (Oswestry disability index and Roland Morris questionnaire). The secondary outcome measure was pain threshold at muscular tender points in the quadratus lumborum, pyramidal, mayor gluteus, and hamstrings.
RESULTS:
In all, 37 participants completed the study. The results of the intragroup comparisons showed statistically significant improvements in both groups in the visual analogue scale (Osteopathic manipulation group,
CONCLUSION:
Osteopathic manipulation of the sacroiliac joint improves pain and disability in patients with sacroiliac dysfunction after three weeks of treatment.
Introduction
One of the main problems faced by physiotherapists in primary care is low back pain with or without radiation to lower limbs. It is estimated that 3–4% of the primary care consultations of the Spanish health system are due to low back pain, only surpassed in demand by the common cold [1, 2].
Between 80–85% of low back pain cases are of unknown origin [3, 4]. The natural evolution of acute low back pain is remission within six weeks in 75–90% of the cases, regardless of the therapy approach used for its management [5, 6]. However, its high incidence along with the low therapeutic effectiveness due to the lack of knowledge of its cause means that the remaining 10–25% are at risk of developing chronic pain. This is a serious health problem in todays’ society, with great social, occupational and economic repercussions as well as professional, social and psychological consequences. For instance, up to 29% of them end up diagnosed with depression [7].
It has been evidenced that many patients with acute low back pain improve clinically without specific therapeutic treatment. In contrast, it is less clear why others develop recurrent or chronic symptoms [5, 7].
There are many different treatment approaches for the management of low back pain. Despite the large amount of published studies, the evidence remains contradictory [8]. Pharmacological treatments like NSAIDs have shown positive results in acute low back pain but not in chronic [9] pain. Conservative physiotherapy interventions (thermotherapy, laser, ultrasound, interferential currents, transcutaneous electrical nerve stimulation-TENS, mechanical lumbar traction and massage) have been studied and found to be ineffective [10, 11, 12].
In contrast, educational interventions, interdisciplinary rehabilitation, cognitive-behavioral therapy, exercise, manual therapy and spinal osteopathic manipulation [10, 11, 13] are among the recommended treatment approaches. The systematic review conducted by Chou et al. [13] showed evidence of the effectiveness of the cognitive-behavioral therapy, the interdisciplinary rehabilitation, the exercise and the spinal osteopathic manipulation for the management of sub-acute or chronic low back pain. In particular, spinal osteopathic manipulation is one of the techniques used to treat low back pain [14] and is recommended by many clinical practice guidelines [10, 11, 12].
Researchers have suggested that alterations in the electrical activity of the muscle, the decrease of the muscle inhibition, the reduction of reflex muscle spam and the increase of the joint range are some of the effects of spinal osteopathic manipulation that could explain the improvements achieved with this technique. These positive changes include the restoration of the range of movement of dysfunctional joints, the improvement of the muscle reflex responses, the reduction of the lower limb muscular inhibition and the improvement of movement symmetry [15, 16, 17].
In their clinical practice, physiotherapists find that the sacroiliac joint is one of the anatomical joints that most frequently need to be assessed in the objective evaluation of patients. This joint is recognised as a potential source of low back pain with or without radiation to lower limbs [18], between 15%–30% of the cases [19, 20]. Sacroiliac joint syndrome has been described as pain and decreased mobility of the sacroiliac joint resulting from a mechanical disorder of the joint [17]. The sacro-iliac joint is considered a part of the lumbo-pelvic-hip complex which includes the fourth and fifth lumbar joints, the two hip joints and the symphysis pubis [17]. Thus, what one does affects the position and movement of the others [17]. In addition, studies that used fluoroscopically guided diagnostic intra-joint injections [21] indicate that the sacroiliac joint dysfunction has a prevalence of 13–30% in patients with chronic low back pain. Consequently, one of the treatment approaches within the current paradigm for the management of sacroiliac dysfunctions is the osteopathic manipulation of the sacroiliac joint [12].
The objective of this study was to assess the effectiveness of the sacroiliac joint osteopathic manipulation on low back pain with or without radiation to lower limbs, as well as to compare this treatment technique with an electrotherapy-based programme.
Materials and method
This was a single-blind randomized clinical controlled pilot study. Ethical approval was obtained from the Bioethical Commission of the University of Extremadura (Spain) and the National Health Service Bioethical Commission (Spain) (Registration number: 100/2016). All the ethical considerations and requirements of human clinical research mentioned in the Declaration of Helsinki were met. The trial was registered with the ClinicalTrials.gov registry (Study Identifier: NCT03794830). Written informed consent was obtained from all participants.
Participants and procedures
A total of 151 patients with low back pain referred to the Physiotherapy Unit of the Gévora Health Centre (Extremadura, Spain) by a primary care physician. The inclusion criteria were: patients aged between 18–70 years old diagnosed with low back pain with or without radiation to lower limbs, sacroiliac joint dysfunction or hypo mobility, to have stopped taking anti-inflammatory medicines or analgesics three days before the commencement of the study. The exclusion criteria were: to present any contraindication for osteopathic manipulation of the sacroiliac joint such as the following medical conditions: spine and pelvis destructive injuries, fractures, lumbar surgery, sacroiliac instability, spondylolisthesis, pregnancy, cauda equina syndrome, abdominal aneurysm, infection, inflammatory arthritis, tumours or osteoporosis.
Measures were taken at baseline (week 0) and post intervention (week 4). The evaluation was performed the day after the end of the sessions to avoid immediate post-intervention effects. As the last session was held on the last day of week 3, the evaluation started in week 4. The primary outcome measures were pain measured with the Visual Analogue Scale (VAS) [15] and functional disability assessed with the Oswestry disability index [17] and Roland Morris questionnaire [10]. The secondary outcome measure was pain threshold at muscular tender points [17] in the quadratus lumborum, pyramidal, mayor gluteus and hamstrings which was evaluated with the Wagner digital algometer, (FPIX model). The sacroiliac dysfunction was assessed at the baseline measurement. The assessor was independent to the study and therefore, blinded to group allocation.
After the first assessment, the participants were randomly allocated to an osteopathic manipulation group (intervention group) and to an electrotherapy group (control group). A computer random number generator was used to produce even allocation ratios by using the IBM SPSS 23 statistical package. The randomisation list was held by an independent researcher who was unrelated to any aspect of the trial.
The osteopathic manipulation group patients were treated with a semi-direct osteopathic manipulation of the sacroiliac joint. The technique was performed with the patient in side lying and with the pelvis in oblique position. The physiotherapist hands were placed on the patient’s shoulder and on the posterior-superior iliac spine (Fig. 2). The treatment sessions were carried out twice a week every 3 to 4 days over a period of time of 3 weeks (a total of 6 sessions). The electrotherapy group patients followed the electrotherapy protocol of the Physiotherapy Unit. This protocol included the application of microwaves (circular antenna in lumbar area, pulsating-mode 120W for 12 minutes) followed by the application of conventional analgesic TENS (80 Hz frequency, 30 minutes). This method has been used for two main reasons: the patient’s high tolerance and the rapidity in which analgesic effects appeared. The electrotherapy treatment was carried out 5 days per week over a period of time of 3 weeks (15 sessions).
The participants did not receive any other treatment during the intervention. They stopped their medication (analgesics and anti-inflammatories) three days before the commencement of the study. Due to the nature of the treatment, neither the participants nor the therapist were blinded to the group assignment. Both treatments were performed by a qualified physiotherapist member of the Spanish Chartered Society of Physiotherapists, trained in joint osteopathic manipulation and electrotherapy and with extensive experience in the field.
Statistical analysis
The collected data was analysed with the SPSS 23.0 version (Statistical Package for the Social Sciences). For the statistical analysis, intragroup comparisons were carried out, i.e. within the same group and the time factor (pre and post-intervention), and intergroup comparisons, that is to say, between the participants of both groups and the group factor. Normative distribution was evaluated using the Shapiro-Wilk test. The intragroup analysis was performed using the Wilcoxon signed rank test for non-parametric related samples and the intergroup analysis was calculated through the Mann-Whitney U test (non-parametric test) for all the outcome measures. In order to analyse if there were variables that influenced pain reduction and disability in the osteopathic manipulation group, the Spearman’s correlation coefficient between two ranked variables was used for quantitative variables.
A value of
CONSORT flowchart of the study.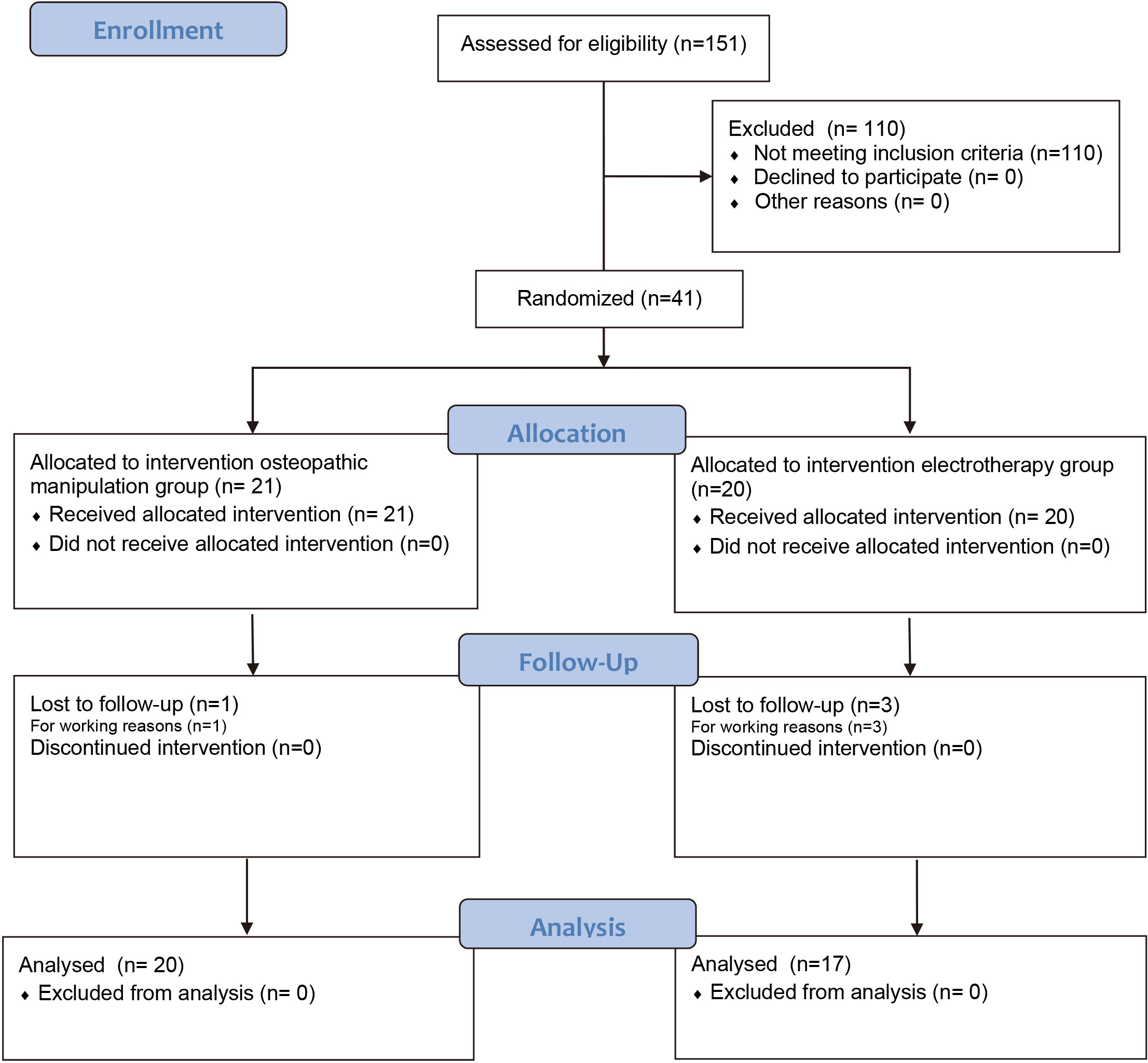
Accepting an alpha risk of 0.05 and a beta risk of 0.2 in a two-sided test, 12 subjects were necessary in the first group and 12 in the second to recognize as statistically significant a difference greater than or equal to 15 units [22]. The common standard deviation was assumed to be 10 and the correlation coefficient between the initial and final measurement as 0.35 [23].
Out of the 151 participants recruited, 41 met inclusion criteria and the final study sample consisted of 37 patients (Fig. 1). Participant characteristics were well balanced between arms at baseline (Table 1). The participants had the following clinical presentation: 4 patients had low back pain, 20 patients had lumbo-pelvic or pelvic pain, 8 patients had lower limb irradiation above the knee and 5 patients had lower limb irradiation below the knee.
Osteopathic manipulation of the sacroiliac joint.
Baseline characteristics of the participants
cm: centimeters; Kg: kilograms; m: meters; SD: Standard Deviation;
Pain and disability intergroup assessment
SD: Standard Deviation;
Pain and disability intragroup assessment
Note. Preint
Table 2 shows the results obtained in relation to pain and disability. The data suggest that osteopathic manipulation is much more effective than electrotherapy when it comes to pain relief and disability reduction in patients with low back pain with or without radiation to the lower limbs.
The results related to the muscle pain threshold assessment did not show statistically significant differences between both groups for any of the evaluated muscles (right quadratus lumborum:
In order to determine the existence of variables that could indicate when could be appropriate to apply an osteopathic manipulation of the sacroiliac joint and for which type of low back pain could be useful, the correlation of all the pain and disability outcome measures in both groups was analysed. The results of this analysis showed statistically significant changes in the osteopathic manipulation group: the pain threshold increased when applying pressure in the right quadratus lumborum (
Intragroup analysis
The analysis of pain and disability is shown in Table 3. Statistically significant results were obtained in both groups for all variables except for the Roland Morris questionnaire that was only significant in the osteopathic manipulation group.
The data also indicated that, at the end of the intervention (post-intervention), the pain threshold at all the muscular tender point assessed was significantly increased in the osteopathic manipulation group (right quadratus lumborum:
Discussion
The results of our study showed that, according to the changes obtained in the Oswestry disability index, both treatment techniques used, osteopathic manipulation and electrotherapy, improved significantly pain and disability. However, on the Roland Morris questionnaire, only the positive changes related to osteopathic manipulation were significant. In addition, the intergroup analysis revealed that osteopathic manipulation was more effective for pain and functional disability than electrotherapy treatment. The Oswestry disability index is considered the best option for patients with greater impairment (moderate-intense disability), as it discriminates better the differences in functional disability in the most affected patients, while the Roland Morris questionnaire is recommended in patients with less functional limitation, with the manipulation being effective in patients with greater or lesser impairment [17]. In contrast, electrotherapy only proved to be effective on the Oswestry disability index, i.e. when patients are more affected. Given these results, in the case of patients with little functional limitation, the use of osteopathic manipulations would be more indicated.
To date, no study that specifically compares osteopathic sacroiliac joint manipulation with electrotherapy in the management of low back pain has been found in the literature. However, osteopathic sacroiliac joint manipulation has been studied and compared with other treatment techniques. Wreje et al. [24] conducted an intervention in primary care with 39 patients with acute low back pain. They compared osteopathic sacroiliac joint manipulation with different manual interventions with placebo consisting of transverse massages on gluteus medius for 3 minutes. The therapist in charge in the patient’s clinic could decide whether to apply a sacroiliac manipulation (the same technique used in our study), or to apply joint mobilisations combined with stretching. Pain was measured using the VAS. Regarding the medication, the use of paracetamol was recommended in both groups. The results obtained showed that osteopathic manipulation reduced pain and medication intake as compared to the control group.
There are other studies carried out in a primary care health setting that have shown the benefits of applying osteopathic manipulation in patients with low back pain. Fritz et al. [25] conducted a clinical trial based on postural education and hygiene and found significant improvements in pain after at the measurements performed at week 4 and 12. A clinical trial carried out in the United Kingdom [26] compared two study groups. One group received osteopathic manipulation combined with exercise and the other group performed only exercise. Both groups improved on the Roland Morris questionnaire scores at 3 and 12 months, whereas the exercise-only group just had a small benefit at 3 months.
In the systematic review conducted by Licciardone et al. [27], the effectiveness of acute and chronic low back pain osteopathic manipulation was assessed. The analysis of the included studies evidenced its effectiveness on pain relief in the short (1 month), medium (3 months) and long term (12 months) versus the placebo control groups. The manipulation decreased the drug intake or led to drug withdrawal in some of the clinical trials [27].
There are important differences between our research and those clinical trials conducted in primary care, as well as with Licciardone et al. [27] systematic review clinical trials: in most of the studies drug intake was allowed and the rest was not specified. We consider that drug intake could influence the results of the interventions. In this respect, we were very strict in the selection criteria of our study to avoid the possibility that the benefits obtained from the manipulation may be due to the medication, as scientific evidence has demonstrated [10].
Additionally, we only chose one possible technique to treat sacroiliac joint dysfunction based on osteopathic manipulation. The approach of some clinical trials to use different techniques with different biomechanics and neurophysiological effects made difficult the comparison of results. Molins-Cubero et al. [28]investigated the effect of global bilateral osteopathic manipulation on both sacroiliac joints versus placebo (osteopathic manipulation simulating position held for 2 minutes) on low pelvic and lumbar pain in women with dysmenorrhea. The manipulation was effective and achieved a significant improvement in pain and sensitivity in both sacroiliac joints measured with algometry pressure, as it is shown in our study. One of the limits of their study was that anti-inflammatory medication intake was not controlled.
There is some controversy with regards to the effectiveness of the manipulation versus electrotherapy. The review carried out by Chou et al. [13] found good evidence that supported the effectiveness of manipulation in the treatment of acute and chronic low back pain, in comparison to microwaves and TENS. In contrast, Anderson et al. [29] did not find difference between osteopathic manipulation and standard allopathic treatment with medication and physiotherapy (diathermy, TENS and ultrasound among others). According to their criteria, the physical therapist may decide which area should be treated and which osteopathic manipulation technique should be used. These techniques could be a thrust, a muscle energy technique or a myofascial release. As previously mentioned, the use of different biomechanics and neurophysiological techniques which have different effects may alter the result. Furthermore, if the treated areas differ, the results will also differ. This was revealed by Chiradejnant et al. [30] who achieved different results in their study results depending on whether they treated the upper or lower back. Therefore, in our study, the intervention involved the use of the same osteopathic manipulation technique only in the sacro-iliac joint for treatment of all participants.
The results obtained indicate that the spinal mobilisation applied to the lower lumbar spine levels was associated with greater pain relief than when applied to the upper lumbar spine levels on five outcome measures: current pain intensity was reduced by 0.5 units more on the 0–10 Scale (
Limitations
One of the limitations of the study is the use of palpation tests as they can have a low reliability. However, in order to minimise this limitation, we used a battery of tests proposed and used by most researchers [31, 32, 33].
Future research should focus on prospective long-term studies in order to observe how long the effects of osteopathic manipulation of the sacroiliac joint last in the patients during the first post-treatment trimester. This would allow to reach more solid conclusions.
Conclusion
Based on the results of the present study, both osteopathic manipulation and electrotherapy treatments are effective in reducing pain and disability in patients with low back pain with or without radiation to lower limb in the presence of sacroiliac dysfunction. However, the results showed greater effectiveness in the osteopathic manipulation group. It would be advisable for treatment protocols for low back pain with or without lower limb irradiation to include osteopathic manipulation of the sacroiliac joint if the patients present sacroiliac joint dysfunction.
Footnotes
Conflict of interest
None to report.