
Abstract
BACKGROUND:
Numerous studies have investigated factors for trunk, balance stability and gait parameters of post-stroke patients. Evidence-based recommendations are required for the treatment of ankle proprioceptive exercise with thermal stimulation in post-stroke patients.
OBJECTIVE:
We investigated the effects of ankle proprioceptive exercise with thermal stimulation on the trunk stability, balance, and gait ability of post-stroke patients.
METHODS:
A total of 30 patients were randomly divided into the ankle proprioceptive training and thermal stimulation group (APT) and control group. The APT group performed ankle proprioceptive exercises with thermal stimulation for 60 min five times a week for eight weeks. The control group followed conservative treatment for 60 min five times a week for eight weeks. Trunk stability was measured with the trunk impairment scale (TIS) and balance tests were performed with the center of pressure (COP), limits of stability (LOS), Berg Balance Scale (BBS), and functional reach test (FRT) and gait ability was performed by OptoGait and 10 m WT.
RESULTS:
There was a significant difference (
CONCLUSION:
This study can be used as intervention data for recovering trunk, balance stability and gait parameters in post-stroke patients.
Introduction
Stroke is a central nervous system disease that occurs as a result of poor blood supply to the brain tissues due to blockage or bursting of the blood vessels supplying blood to the brain [1], causing motor, sensory, speech, perceptual, and cognitive impairments depending on the location of the damage [2]. Despite the considerable advancements in the prevention of strokes and their circumstances, their incidence continues to increase as an increasingly unpredictable situation begins to unfold [3].
The trunk, as the center of the body, adjusts functional movement postures to prepare for movement and, by regulating weight shifting against gravity during dynamic movement, allows adaptation to new postures [4]. Independent trunk control in a sitting posture is an important predictor of functional recovery after a stroke and is an important goal in terms of the rehabilitation of stroke patients [5].
Balance, or the ability to continuously maintain body posture by responding to environmental changes during weight shifting while maintaining the center of gravity within the base of support [6], is involved in a variety of functional factors. Therefore, impairment in these factors can result in the loss of balance [7]. The factors that reduce balance include delayed reflexes, reduced proprioception, postural sway as a result of weakened muscles, reduced coordination in the ankles and knees, and reduced flexibility [8].
Stroke patients can experience many different impairments depending on the damaged area, including gait disturbance and balance disorders as a result of damage to the motor and sensory nerves. These are the major functional impairments of stroke patients [9]. Furthermore, an increase in weight bearing on the non-paretic side reduces stable locomotor skills due to the difficulty in distributing weight evenly on both sides [10]. In contrast to regular people, stroke patients have limited passive and active movements in their joints and, over a long period of time, suffer changes in the epidemiological characteristics of their muscles or the connective tissues surrounding their ankles as a result of limited movement from weakened and stiff muscles surrounding the ankles, specifically the ankle joint, this, in turn, reduces movement [11]. Patterson et al. [12] stated that independent walking is one of the most important training goals for stroke patients and that goals for improving postural control and balance are set up to achieve unimpeded mobility. Nonetheless, the difficulty of improving the balance of stroke patients arises from the various mixed elements that form their balance [13].
The various approaches for fostering proper balance and gait among stroke patients include balance training [14], visual feedback training [10], unstable support-surface exercises [15], and dual task exercises [16], along with an intervention for the ankle joint, which is a balance strategy.
The most important roles of the ankle joints and feet are balance control against postural sway, shock absorption during walking, and forward movement of the lower limbs, all of which require a sufficient range of motion from the ankle joints, muscle strength, and proprioception [17]. Somatosensory loss occurs in approximately 50% of stroke patients, and postural control is impaired due to difficulty in somatosensory integration [18, 19, 20]. Serving an important role in the balance control of the body, the reeducation of ankle joint movement plays a key function in solving problems regarding a patient’s gait and balance control by resolving abnormal forms of muscular control by the ankle joints and persisting joint contractures and proprioception impairment [21]. Bayouk et al. [22] reported an increase in the postural stability of stroke patients through the use of proprioception exercises for the ankles, while Pajala et al. [23] claimed that exercises for an ankle joint strategy are effective in improving postural stability. As demonstrated, improving the gait and balance of stroke patients requires strengthening the ankle joints and an approach toward proprioception. However, there is a dearth of research on ankle joint strategies and proprioception, particularly, on a thermal sensitivity stimulation (TS) approach promoting the activation of tactile or mechanical stimulation to the patient.
Therefore, the present study attempts to present reference data for an intervention aimed at improving the trunk stability, balance, and gait ability of stroke patients by examining the impact of ankle joint proprioception exercises and TS on the trunk stability, balance, and gait ability of post-stroke patients. The hypothesis of this study is that ankle joint proprioception exercises and TS will affect the improvement of trunk, balance stability and gait parameter in post-stroke patients.
Methods
Study subjects
This study was performed between May and July 2019. Thirty patients who met the inclusion criteria and who received treatment were included as the research subjects. The inclusion criteria were: (1) patients whose first stroke diagnosis had passed six or more months, (2) those with no visual or auditory impairments, (3) those with no cognitive impairments, scoring 24 or higher on the K-MMSE (Korean Mini-Mental State Examination), (4) those capable of walking independently for six minutes, and (5) patients who consented to participate in the study, with both the patients themselves and the guardians understanding the purpose of the study. On the other hand, exclusion criteria were: (1) patients with hemineglect or hemianopsia, (2) patients with a somatosensory loss which affects the intervention, and (3) patients with a musculoskeletal injury or a degenerative disease which affects their balance and gait. The number of study subjects was determined by setting effects d
Flow diagram of total experimental procedure. TIS, trunk impairment scale; COP, center of pressure; LOS, limits of stability; BBS, Berg balance test; FRT, functional reach test; APT, ankle proprioceptive training and thermal stimulation group; CON, control group.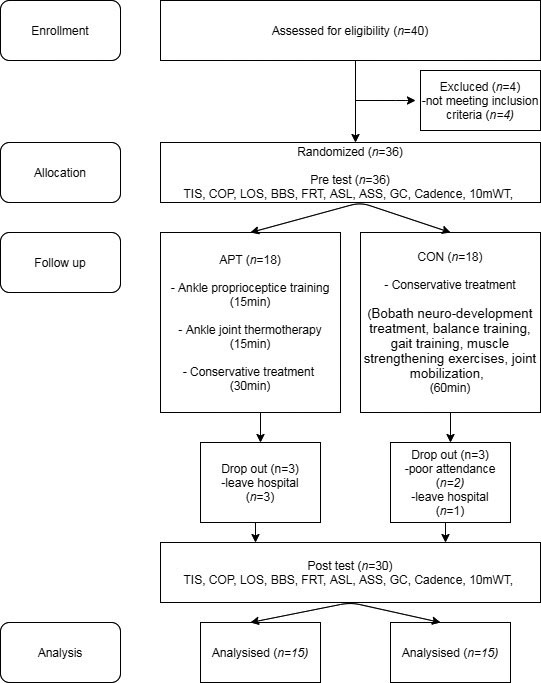
The subjects were divided into two groups through a computer excel program using random placement before the start of the training in order to minimize selection bias, with 15 placed in the ankle proprioception and thermotherapy group and 15 placed in the conservative treatment group, with both groups undergoing 60-minutes of training, five days a week, for eight weeks. The interventions were conducted over eight weeks and pre-test was performed one week before, and a post test was performed eight weeks later. Three physical therapists with more than a master’s degree or higher and 5 years of clinical experience performed measurements or interventions under blinded conditions. The evaluation examined trunk impairment scale (TIS). Balance were performed with the center of pressure (COP), limits of stability (LOS), Berg Balance Scale (BBS), functional reach test (FRT). Gait parameter were performed with affected step length (ASL), affected single support (ASS), gait cycle (GC), and 10 meter walking test (10 m WT).
All subjects sign a consent form to participate in the experiment after sufficiently listening to an explanation of the study. The study was approved by the Sham-yook university Institutional Review Board (2-7001793-AB-N-012019004HR).
Ankle proprioceptive training and thermal stimulation group (APT)
Before receiving 30 minutes of conservative treatment, the APT underwent 15 minutes of ankle proprioception training and then 15 minutes of ankle joint thermotherapy. After referring to, revising, and supplementing the contents proposed by Lynch and Grisogono [22], the ankle proprioception exercise program was implemented with the following routine: 1) boost ankle joint mobility for 1 minute; 2) repeat the exercise of sitting to standing five times for 3 minutes after shifting weight to the paretic side in a sitting posture; 3) weight-bearing strengthening exercise for 2 minutes on the paretic side in a standing position; and 4) shift weight five times for 2 minutes toward various directions from a standing posture. All of these activities amounted to 8 minutes of exercise (Fig. 2A). For Stage 2, weight shifting and task training while standing on one foot involved the following: 1) boosting ankle joint mobility five times for 2 minutes in a sitting posture; 2) raising the non-paretic foot five times for 1 minute; 3) Standing on paretic one leg, weight-bearing stabilization exercise of the paretic leg (five times for 2 minutes); and 4) performing upper limb tasks five times for 2 minutes while standing on one foot (Fig. 2B). For TS, the temperature was set and implemented by modifying and supplementing the study of Chen et al. [25]. First, the patients rested their head on one or two pillows and were mad to lie on their sides on a mat so that their lower limbs were visible. Hot packs (70
Ankle proprioceptive training.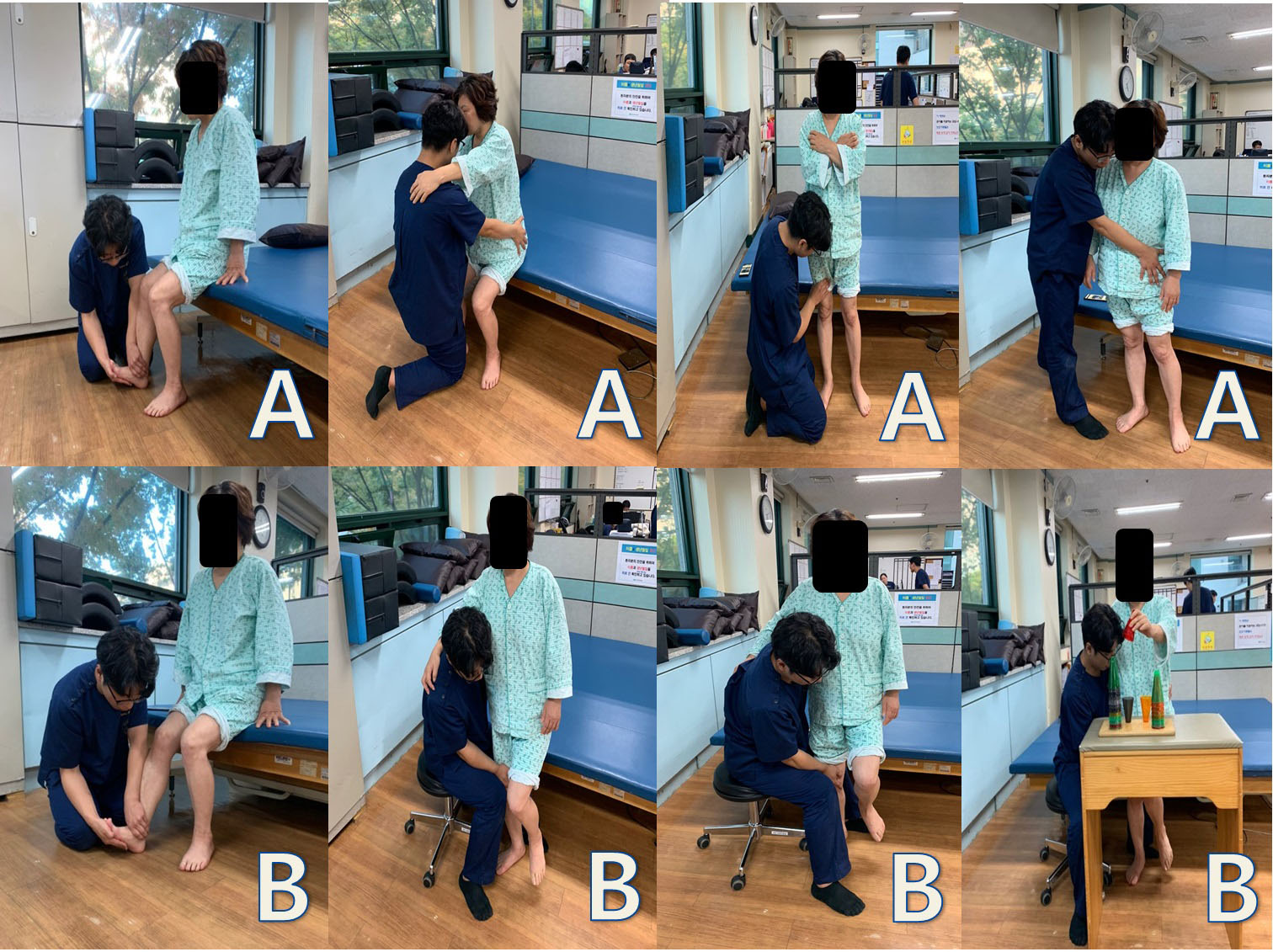
Thermal stimulation pack (A: hot pack; B: ice pack).
Control group (CON)
The CON received conservative treatment for 30 minutes and conservative treatment for an additional 30 minutes. CON was performed one-on-one between the therapist and patient to improve the subject’s motor control. Conservative treatments included proprioceptive neuromuscular facilitation, Bobath neurodevelopment therapy, balance training, gait training, muscle strengthening exercises, and joint mobilization, depending on the subject’s conditions and needs.
A pre-test was conducted before the first intervention and a post-test was conducted after all interventions were completed. To correct for inter-tester differences, one physical therapist (per assessment) with more than five years of clinical experience and a master’s degree or higher performed the measurements under blinded conditions. To exclude any interference from other intervention effects, the assessments were performed on days with no intervention plans; 30 minutes of rest was allowed between assessments.
Trunk impairment scale (TIS)
The TIS is a clinical test used to determine the impairment in movement of a stroke patient’s trunk; the static and dynamic balance abilities are measured in a sitting position, as well as the coordination ability of the trunk. The TIS consists of 17 items, 3 of which are related to the static balance ability in a sitting position, 10 are related to the dynamic balance ability, and 4 are related to the coordination ability of the trunk. The TIS is calculated as a point from a minimum of 0 to a maximum of 23 points; the higher the score, the better the control ability of the trunk. The inter-measure reliability is ICC
Biorescue (COP and LOS)
The balance measurement and training system (AP1153 Biorescue, France) was used to measure the movement distance of the COP at a standing posture. For COP measurement, subjects were made to look straightforward with legs spread by 30
Berg balance scale (BBS)
With a total of 14 questions, BBS can be divided into the three categories of sitting, standing, and postural changes. Each question is applied a minimum score of 0 to a maximum score of 4, which amounts to a sum total of 56 points. This measurement tool boasts a high level of reliability and internal validity for assessing balance, with an intra-rater reliability and an inter-rater reliability of
Functional reach test (FRT)
The FRT is used to measure activities regarding balance. Developed to find balance disorders in the clinic and test changes in balance performance with the passage of time, the test is relatively effective, as an easy-to-use, economical, and reliable tool, in measuring the LOS through the measurement of maximum distances subjects can reach horizontally by extending their arm while maintaining their base of support in a comfortable standing posture. Subjects are to stand position and reached their arms forward in parallel with one arm horizontally in a flexion of about 90 degrees. It was measured as the distance (cm) from the end of the third metacarpophalangeal joint in the starting position to the maximum reach. The hip joint and buttock’s posterior displacement and knee joint flexion were prevented from occurring. The inter-tester reliability is
OptoGait
OptoGait (Microgate Srl, Bolzano, Italy) was used to collect data on gait patterns for quantitative analysis.
The gait analyzer consists of two transmission and reception bars with a total length of 4 m and a webcam (Logitech Webcam Pro 9000). A 1 cm LED is installed on the inside of the bar, and the transmission bar communicates with infrared rays. Each subject was instructed to walk 7 m at a comfortable speed. Sensors on the feet collected information on walking variables while the subject walked for 3 m on platform, excluding the initial 2 m in the accelerating phase and the last 2 m in the decelerating phase. In connection with intervention protocol affected step length (ASL), affected single support (ASS), gait cycle (GC), and cadence were analyzed. The intra-rater reliability was
10 m walk test (10 m WT)
The 10 m Walk Test uses 10 cm width tape to connect a straight distance of 14 m between two points of a walk path. Two meters are marked inward from both ends of the 14 m walk path to create marker lines. The 2 m of both the start and finish are set up for acceleration and deceleration. The walk time for the 10 m walk path is measured with a stopwatch capable of measuring to the unit of 0.01 seconds, with the speeds obtained used as measurement variables for functional walking. All subjects were measured three times before their mean value was used as the outcome value. The inter-tester reliability of this test was
Statistical analyses
PASW Statistics 21.0 was used for all statistical analyzes performed in this study. Gender, paralyzed side, and stroke type were examined with a chi-square test, and variable homogeneity between the two groups before training was tested with an independent sample
Result
Table 1 shows the general characteristics of the patients. The APA group included 9 males (60%) and 4 females (40%), while the control group included 8 males (53.3%) and 7 females (46.7%). In terms of diagnosis, the APA group had 9 infarctions (60.0%) and 6 hemorrhages (40.0%), while the control group had 10 infarctions (66.7%) and 5 hemorrhages (45.5%). In terms of height, the subjects in the APA group were 163.09
Significant differences were observed in the trunk, balance stability and gait parameter before and after training within the groups (
General characteristics of the subjects (
30)
General characteristics of the subjects (
Mean(SD). MMSE, mini-mental state examination; APT group, ankle proprioceptive training and thermal stimulation group.
Comparison of trunk and balance ability between the groups (
Comparison of gait parameter between the groups (
The purpose of this study was to evaluate the effects of interventions on trunk, balance stability and gait parameter of chronic stroke patients. The study was performed on two groups: 1) ankle proprioceptive exercise with thermal stimulation group (15 subjects) and 2) control group (20 subjects).
Tyson et al. [6] reported an improvement in balance as one of the therapeutic objectives for hemiplegia patients. The most important training objective regarding therapeutic intervention for hemiplegia patients is independence activities and walking, with balance in a standing posture and postural balance control prioritized to achieve a smoother walking function [12]. However, balance consists of an extremely complicated system, including sight, hearing, the vestibular system, and proprioception, which must stimulate the central nervous system in order to enable an individual to respond to environmental changes quickly and accurately [33]. However, due to their inability to evenly distribute their whole weight between both legs, stroke patients experience a reduction in balance [34]. Moreover, walking undergoes a reduction in speed, cadence, and step length as a result of spatiotemporal asymmetry [30]. Therefore, balance training for stroke patients is absolutely necessary to achieve functional recovery and independent living. Hence, the present study examined the impact of proprioception ankle exercises and TS therapy on trunk stability, balance, and walking.
Upon examining the impact on trunk stability, balance, and walking after assorting 30 chronic stroke patients into, first, a group applying in parallel both ankle proprioceptive exercise with thermal stimulation (15 subjects) and, second, a control group which received conservative treatment (15 subjects), the present study found both groups improved in trunk stability, balance, and walking, with the APT group exhibiting greater improvement in the inter-group comparison.
Both groups exhibited improvement with regard to changes in trunk stability after undergoing ankle proprioception exercises and TS therapy, with the APT group exhibiting greater improvement. Anders and Brose [35] previously described the effectiveness of three-dimensional exercises, involving movement forward, backward, left, right, and toward all four diagonal directions, for the facilitation of proprioceptors, and for increasing in equilibrium and trunk stabilization, Mean, while, Karthikbabu et al. [36] reported an improvement in TIS for 30 stroke patients through the use of training on an unstable support surface. These previous results coincide with those obtained in the present study. This implies that summation data are entered into the proprioceptive receptors on the ligaments, muscles, joints, joint capsules, and tendons, from the nerve endings, and induces normal movement by providing the ratio data for muscle to joint movement [37], thereby improving anticipatory postural adjustments and trunk control.
Both groups experienced intra-group improvement with regard to changes in balance ability after undergoing the ankle proprioception exercises and TS therapy, with the APT group exhibiting greater improvement in the inter-group comparison. In a study on ankle exercises for stroke patients, Pajala et al. [38], in a study on the ankle exercises of stroke patients, reported a greater reduction in postural sway for the group applying exercises from an ankle joint strategy than the group applying ankle muscle strengthening exercises while Chen et al. [39] reported that TS in the lower limbs of stroke patients resulted in improvements in BBS scores and Barthel index. The coincide with the COP, BBS, and FRT measurement results obtained in the present study. Furthermore, Johansson et al. [40] stated that TS is deeply related to the activation of various regions of the brain, and that concurrent activation in vast areas of the brain causes neuroplasticity. The present study determined that the ankle joint proprioception exercise intervention improved the proprioceptive nerves in the ankle area and that TS caused neuroplasticity changes in the brain which, in turn, improved balance.
Both groups experienced intra-group improvement with regard to changes in gait parameter after undergoing the ankle proprioception exercises and TS therapy in the present study, with the APT group exhibiting greater improvement in the inter-group comparison. Chen et al. [39] reported an improvement in the functional ambulation classification as a result of thermal intervention on the paretic lower limbs of acute stroke patients. Meanwhile, Kim et al. [41] reported an improvement in the Timed Up and Go Test as a result of proprioception exercise intervention to the ankle joints. This coincides with the results of improvement in walking in the present study. In a study involving the 6-Minute Walk Test administered to stroke patients with ankle joint proprioception problems, Lee et al. [42] reported significant differences in ankle joint proprioception and walking distance, while Lin [43] reported significant differences in ankle joint position sense depending on walking speed and step length. The foregoing demonstrate how ankle proprioception exercises are an extremely important element for walking. Furthermore, Liang et al. [44] stated that the addition of TS to rehabilitation programs can produce much greater stimulation, creating a positive feedback cycle, and, ultimately, drawing out motivation for the paretic lower limbs to be involved in daily rehabilitation programs. In the present study, when stroke patients walk, ankle joint proprioception exercises and TS are thought to produce, an increase in motivation for paretic lower limb movement and improvements in step length and walking distance.
The study is not without limitations. First, a generalized interpretation of the research results for all stroke patients is not possible because only test subjects who satisfied the selection standards were included in the study. Second, the difficulty of finding out the sustainability of the intervention due to the absence of measurements for prolonged effect. Third, the impossibility to completely exclude the impact of daily life on the subjects due to the inability to completely control the daily lives of the subjects apart from the intervention. However, the ankle joint proprioception exercises and TS therapy of the present study were revealed as having a positive effect on trunk stability, balance, and walking for stroke patients. Future studies require an approach in stages including studies on various TS methods and posture and on the prolonged effect of training through the use of follow-up.
Conclusion
The present study confirmed the positive effect of ankle proprioception training and TS therapy on the trunk, balance stability and gait parameter of chronic stroke patients. This is significant as an intervention method for chronic stroke patients requiring long-term treatment. It is difficult to "confirm" positive effects due to sample size and study limitations. A study based on a larger sample size is suggested in the future.
Footnotes
Conflict of interest
None to report.
Funding
This paper was supported by a fund from Gimcheon University in 2019.