
Abstract
BACKGROUND:
Calcific tendinitis of the shoulder is a common disorder resulting in restricted motion and pain.
OBJECTIVE:
This study compared the effects of ultrasound-guided fine-needle puncture (USNP), radial shock wave therapy (RSWT), and the combination of both treatments (COMB) on calcific tendinitis of the shoulder.
METHODS:
We enrolled 62 patients who had unilateral shoulder pain for more than 3 months. The patients were randomly divided into three groups: USNP, RSWT, and COMB. All USNP needle punctures were guided with ultrasound (US), and RSWT was delivered at 2 Hz (2000 shock waves; 0.26 mJ/mm
RESULTS:
A within-group comparison at 3 months revealed significant improvements in the pain VAS (
CONCLUSIONS:
Although no significant differences were observed among the groups in the treatment of calcific tendinitis of the shoulder, more satisfactory outcomes were noted in the USNP and COMB groups than in the RSWT group. Larger samples, longer follow-up times, and other treatment protocols are suggested for future studies.
Introduction
Calcific tendinitis of the shoulder is a common disorder associated with inflammation around calcium hydroxyapatite crystal deposits [1]. This disorder is commonly observed in individuals between 30 and 50 years of age and is painful in 50% of patients [2]. It may also result in a considerably restricted range of motion (ROM) of the affected shoulder. Calcific tendinitis progresses through three distinct stages, namely the precalcific (metaplasia of matrix), calcific (calcification of matrix and resorption of calcific deposits), and postcalcific (reconstitution of matrix) stages.
The classification system proposed by Gartner based on radiographic findings using plain films of the shoulder consists of three types. In type I, deposits are sharply outlined and densely structured, and in type II, the deposits are similar to those in type I or have a cloudy and dense outline and are transparent; in type III, the deposits have a cloudy outline with a transparent structure [3]. Type III plaques have a tendency to resorb. Because of the progression of musculoskeletal ultrasound (US) technology, Chiou proposed another classification system of calcific tendinitis based on US findings as follows: arc-shaped, fragmented or punctate, nodular, or cystic [4]. Plaques that appear fragmented, nodular, or cystic in US images are considered to be in the resorptive phase.
In a recent systematic review [5], needling proved beneficial for patients with subacute or chronic symptoms; however, few studies have compared the effects of needling on the various stages of calcific tendinitis. The failure rate of nonsurgical therapy did not differ significantly between Gartner’s type I and II calcifications in one study [6], whereas in another study, extracorporeal shockwave therapy (ESWT) promoted the breakdown of calcific deposits in both type I and type II calcifications, with respective elimination rates of 30.8% and 61.0% [7]. Consequently, patients with these two types of calcific tendinitis were suitable for the receipt of US-guided needling or ESWT.
Patients with calcific tendinitis are typically treated conservatively, with reported success rates of 30% to 85% [8]. Arthroscopic and open procedures may be advised to curette the calcium deposits in instances in which the pain is chronic or intermittent after several months of conservative treatment; additional subacromial decompression can be performed if necessary [9, 10]. Alternatively, minimally invasive ESWT has been suggested to be an effective treatment option for calcific tendinopathy of the shoulder before surgery [11, 12]. Although ESWT has been studied extensively in relation to musculoskeletal injuries in recent decades, the precise mechanism involved in promoting tissue repair remains elusive [13]. Loew et al. reported that ESWT can induce fragmentation and cavitation of calcific deposits and promote phagocytosis; additionally, it can exert an analgesic effect by influencing pain receptors and neurotransmitters [14].
In recent years, radial shock wave therapy (RSWT) has gained popularity. A radial shock wave is a low-to-medium-energy shock wave that is pneumatically generated through the acceleration of a projectile inside the handpiece of the treatment device and then transmitted radially from the tip of the applicator to the target zone. Radial shock waves exhibit lower pressure and considerably longer rise times than do extracorporeal shock waves. In RSWT, the focal point is not concentrated on the target zone, as in ESWT, but rather on the tip of the applicator [15].
Another conservative method for treating calcific tendinopathy is US-guided fine-needle puncturing (USNP) of the calcific plaque [4, 16]. This method is easy to operate, cheap, safe, and highly successful. Although percutaneous needle aspiration with a large (
A study reported promising clinical and radiological outcomes through a combination of shock wave therapy and US-guided needling [7]. Repeated needle punctures could break down calcific deposits, and RSWT induced fragmentation and cavitation, which made calcium deposits more absorbable [7]. However, few scientific studies on the combined effects of RSWT and USNP have been published. The present study compared the efficacy of USNP, RSWT, and the combination of both to treat calcific tendinitis of the shoulder.
Materials and methods
Design
This prospective randomized controlled trial (RCT) was approved by the institutional review board of Shin Kong Wu Ho-Su Memorial Hospital (20120801R) and registered at ClinicalTrials.gov (NCT02677103). An assignment scheme was generated from a table of random numbers. Written informed consent was obtained from all patients, who were subsequently randomly divided into three treatment groups: USNP, RSWT, and RSWT plus USNP (COMB).
Participants
Between January 2013 and December 2014, 75 patients with calcific tendinitis of the shoulder were recruited from the outpatient clinic at the Department of Physical Medicine and Rehabilitation of the authors’ institution. The inclusion criteria of this study were as follows: 1) between 20 and 75 years of age; 2) at least a 3-month history of unilateral shoulder discomfort; and 3) radiological evidence of both type I and type II calcification – as defined by Gartner – or US-based evidence of arc-shaped calcification – as defined by Chiou [4]. The exclusion criteria were pregnancy, clotting disorders, anticoagulant or antiplatelet treatment, cardiac pacemaker, chronic inflammatory joint disease, infection or tumor of the shoulder, adhesive capsulitis, hyperalgesia of the shoulder due to resorption of a calcific deposit, Garner’s type III calcification, or Chiou’s nodular or cystic calcification [4].
Interventions
All treatments were administered at the Department of Physical Medicine and Rehabilitation by a physiatrist who was familiar with both types of therapy. RSWT was delivered at 2 Hz (2000 shock waves; energy level, 0.26 mJ/mm
All needle punctures for the USNP and COMB groups were guided by US and performed once. A 3.8-cm-long 22-gauge needle attached to a 5-mL syringe was used for puncturing. The puncture site was sterilized with iodine, and the transducer was covered with a sterilized plastic bag. After injecting 3 cc of lidocaine (1%) into the subcutaneous tissue, muscle layer, and subdeltoid bursa, multiple punctures (10–20, depending on plaque size) were performed without aspiration or barbotage. The needle tract was monitored with US to ensure that the needle penetrated through the calcific plaque but not the rotator cuff [4]. The patients in the COMB group received three weekly rounds of RSWT after USNP.
Assessment
All assessments were performed by a masked assessor who was a trained study assistant. The patients were instructed not to reveal any treatment details to the assessor. Except for shoulder radiographs, all assessments and standard sonograms were conducted at baseline and 1.5 and 3 months after completion of the treatment.
Demographic data, namely age, sex, body weight, height, history of diabetes mellitus, and exercise habits, were recorded at baseline. Additionally, information regarding complaint duration (months), previous treatments (injections, physical therapy), and current pain medications was obtained. Occurrence of concomitant diseases and use of medications were also recorded.
Initial radiographs of the shoulder comprised anteroposterior films in neutral, internal, and external rotations. Deposits in the supraspinatus were readily visible on the films in the neutral position, whereas deposits in the infraspinatus and teres minor were most clearly observable during the internal rotation. Calcifications in the subscapularis were most clearly observable in the external rotation of the shoulder.
Outcome measures
The primary outcome measure was the visual analog scale (VAS) to assess pain. Pain was measured using three VASs (horizontal lines measuring 100 mm in length, with 0 on the left indicating no pain and 100 on the right indicating severe pain) pertaining to shoulder pain at rest, during movement, and during sleep. The pain VAS is a reliable and sensitive tool for measuring pain, with a test-retest reliability of
Demographic and clinical characteristics of the subjects
Demographic and clinical characteristics of the subjects
Abbreviations: USNP
The secondary outcome measures in this study were the Constant scores, the 36-Item Short-Form Health Survey (SF-36) for general health status, and the ROM of the afflicted shoulder. The Constant score is a 100-point scoring system comprising 15 points for pain, 20 points for activities of daily living, 40 points for shoulder motion, and 25 points for muscle power of the affected arm [20]. The psychometric properties of the SF-36 have been established in Chinese. The SF-36 is a generic measure of quality of life comprising eight subscales: physical functioning, social functioning, role-physical (role limitations due to physical limitations), role-emotional (role limitations due to emotional problems), mental health, vitality, body pain, and general health. Each subscale generates a score between 0 and 100, with a higher score indicating superior health. Two summary scales for physical and mental health can be computed based on these eight items [21]. Following the guidelines of the American Academy of Orthopaedic Surgeons [22], active and passive ROMs were measured using a conventional goniometer; the measurements included abduction in the frontal plane, forward flexion, internal rotation, and external rotation with the arm at 0 degrees of abduction. Goniometric measurements of the shoulder maintained high reliability when performed by a physical therapist [23].
The calcific deposit size was measured with ultrasonography at baseline and during follow-ups at 1.5 and 3 months. Resorption of the calcific deposit was graded as none, partial, or complete by a physiatrist who was blinded to the treatment modes allocated to the patients.
Statistics
The sample size was calculated by assuming the presence of differences in the primary outcome (pain VAS during activity at 3-month follow-up) among the three groups before conducting the study. Based on power calculations performed using G*Power 3.1.9.2, a total of 63 patients were required to achieve a power of 80% at a type I error level of 0.05 and effect size of 0.5.
Means and standard deviations were reported for continuous measurements. A chi-squared test and the Mann-Whitney U test were used for baseline comparisons and to measure changes in the pain VAS values during activity. No violation of normal distribution from the outcome measurements data was detected using the Kolmogorov-Smirnov test of normality. Analysis of variance for repeated measures was used to analyze the effects of time and the interaction between time and groups. Significance was set at
Flowchart of enrolment and randomisation of the patients in this study. Abbreviations: USNP, ultrasound-guided needle puncture; RSWT, radial shock wave therapy; COMB, combination of both treatments.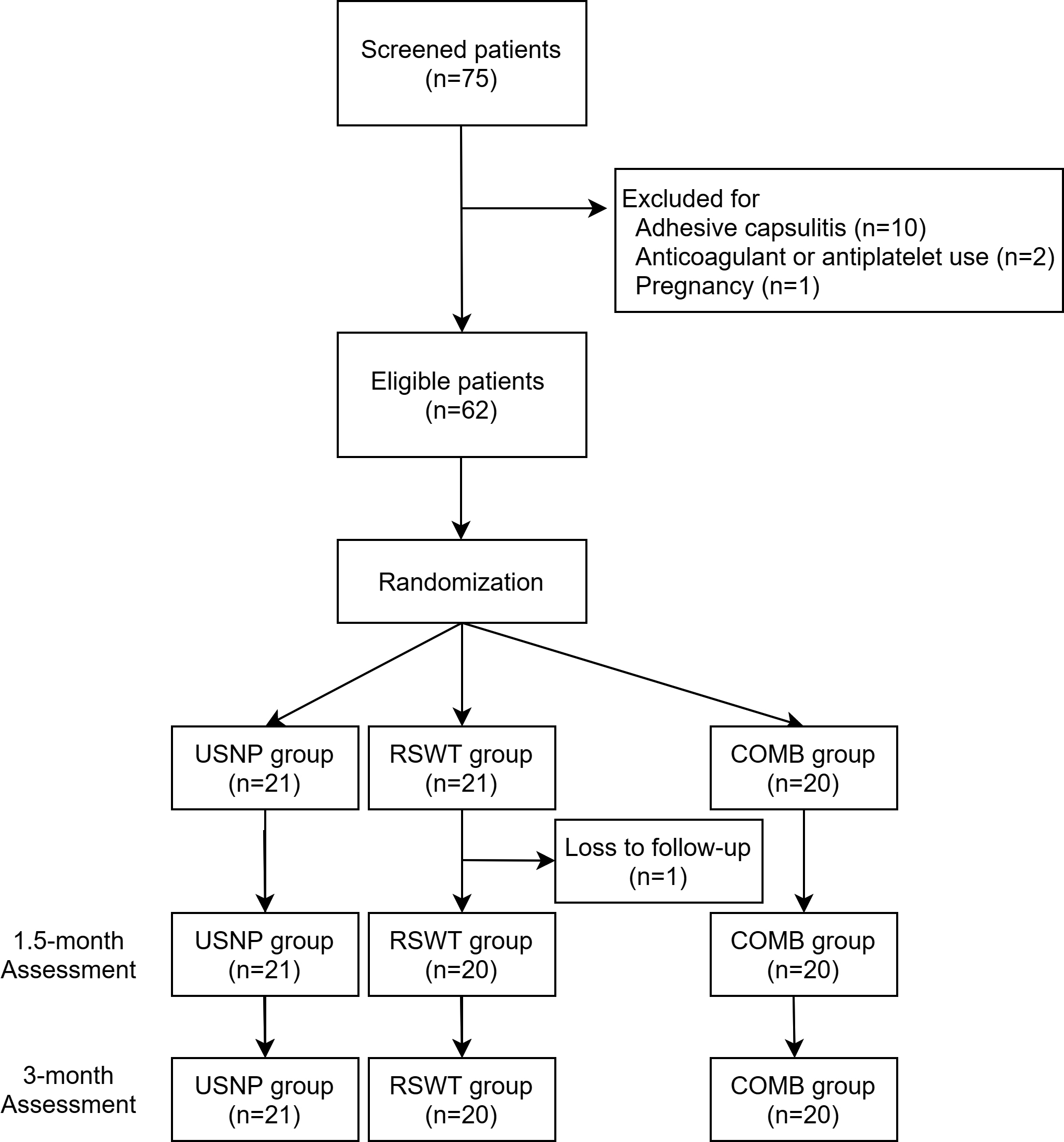
A case in COMB group with ultrasonography during needling of the calcific plaques in the right supraspinatus tendon (A), radial shock wave therapy (B), pre-treatment X-ray (C) and post 3-month X-ray (D). (Abbreviations: D, deltoid; SS, supraspinatus; med, medial; lat, lateral; CP, calcific plaques; 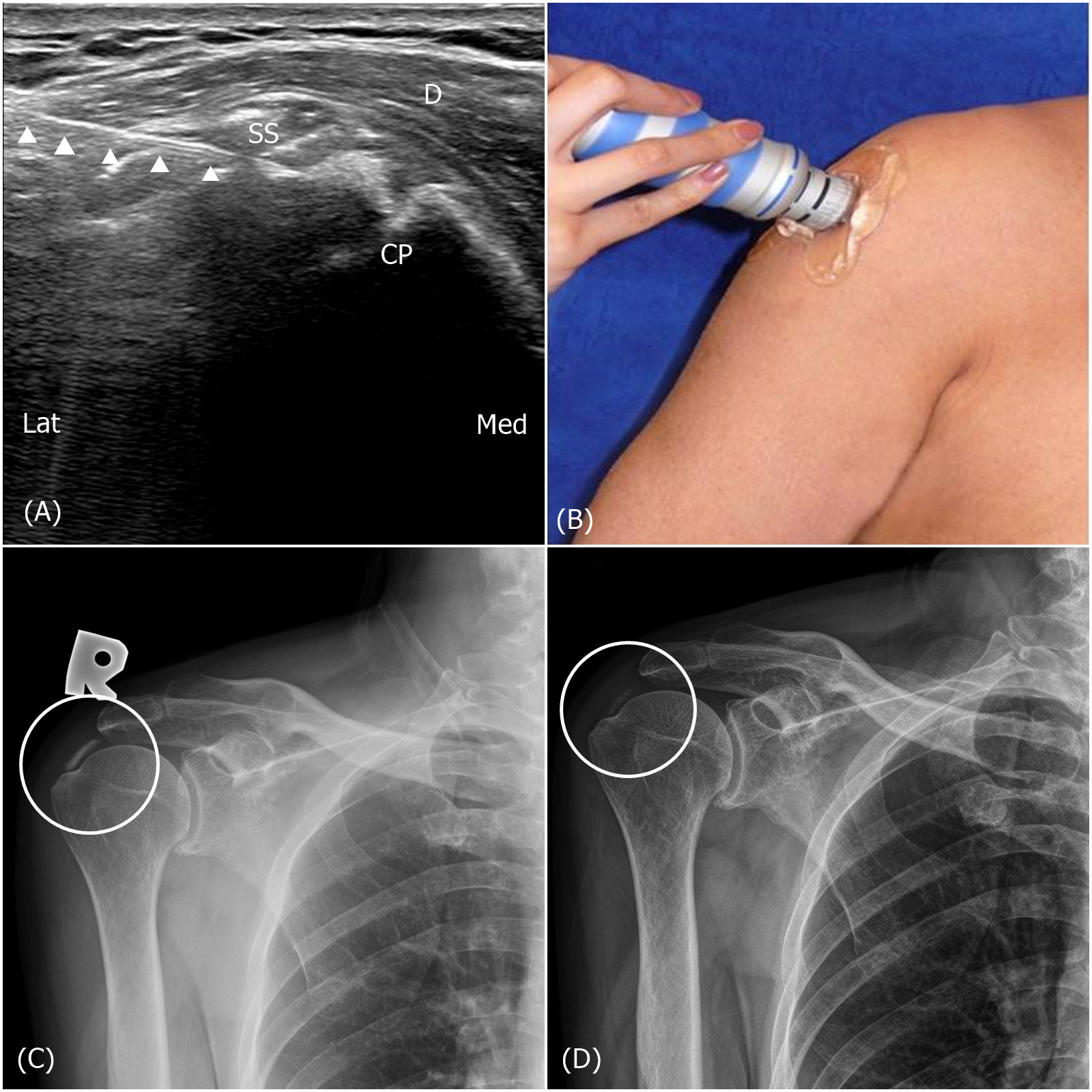
Baseline characteristics
A total of 75 patients with calcific tendinitis of the shoulder were examined in this study. Thirteen patients were excluded because of adhesive capsulitis (10), anticoagulant or antiplatelet medication (2), or pregnancy (1). One participant in the RSWT group was lost to follow-up at the 1.5-month evaluation. A total of 21, 20, and 20 patients were included in the USNP, RSWT, and COMB groups, respectively (Fig. 1). No significant differences in age, sex, body weight, height, disease duration, exercise habits, history of diabetes mellitus, previous treatment (including injection and physical therapy), or current nonsteroidal anti-inflammatory drug medication use were observed among the three groups (Table 1). A patient in the COMB group is presented in Fig. 2.
Primary outcome measures
Within-group comparisons at the 1.5- and 3-month follow-ups revealed significant improvements in the pain VAS during sleep, rest, and activity (Table 2). No statistically significant differences were observed among the groups during the 1.5- and 3-month follow-up periods (Table 2). Furthermore, we analyzed the number of patients whose changes in the pain VAS (during activity) score reached the minimal clinically important difference (MCID) in each group. The MCID of the pain VAS was 1.4 cm, according to a previous study [24]. A significant difference was observed between the USNP and RSWT groups at the 1.5-month follow-up (
Scores from questionnaires for the USNP, RSWT, and COMB groups at three evaluation times
Scores from questionnaires for the USNP, RSWT, and COMB groups at three evaluation times
Abbreviations: USNP
Numbers of the patients whose changes of the values in the pain VAS during activity reached the MCID
Abbreviation: MCID
Within-group comparisons at 1.5- and 3-month follow-ups revealed significant Constant score improvements, but no other significant difference was observed among the groups during those periods (Table 2). Between-group comparisons conducted using the SF-36 revealed nonsignificant improvements in the physical functioning, role-physical, bodily pain, and role-emotional subscales among three groups over time. Only the role-emotional subscale revealed a significant time-group interaction (
Range of motion for the USNP, RSWT, and COMB groups at three evaluation times
Range of motion for the USNP, RSWT, and COMB groups at three evaluation times
Abbreviations: ROM
Average changes in physical-functioning (SF-36), role-physical (SF-36), role-emotional and active external rotation at pre-treatment, post 1.5-month and 3-month. Abbreviations: SE-36, 36-Item Short-Form Health Survey.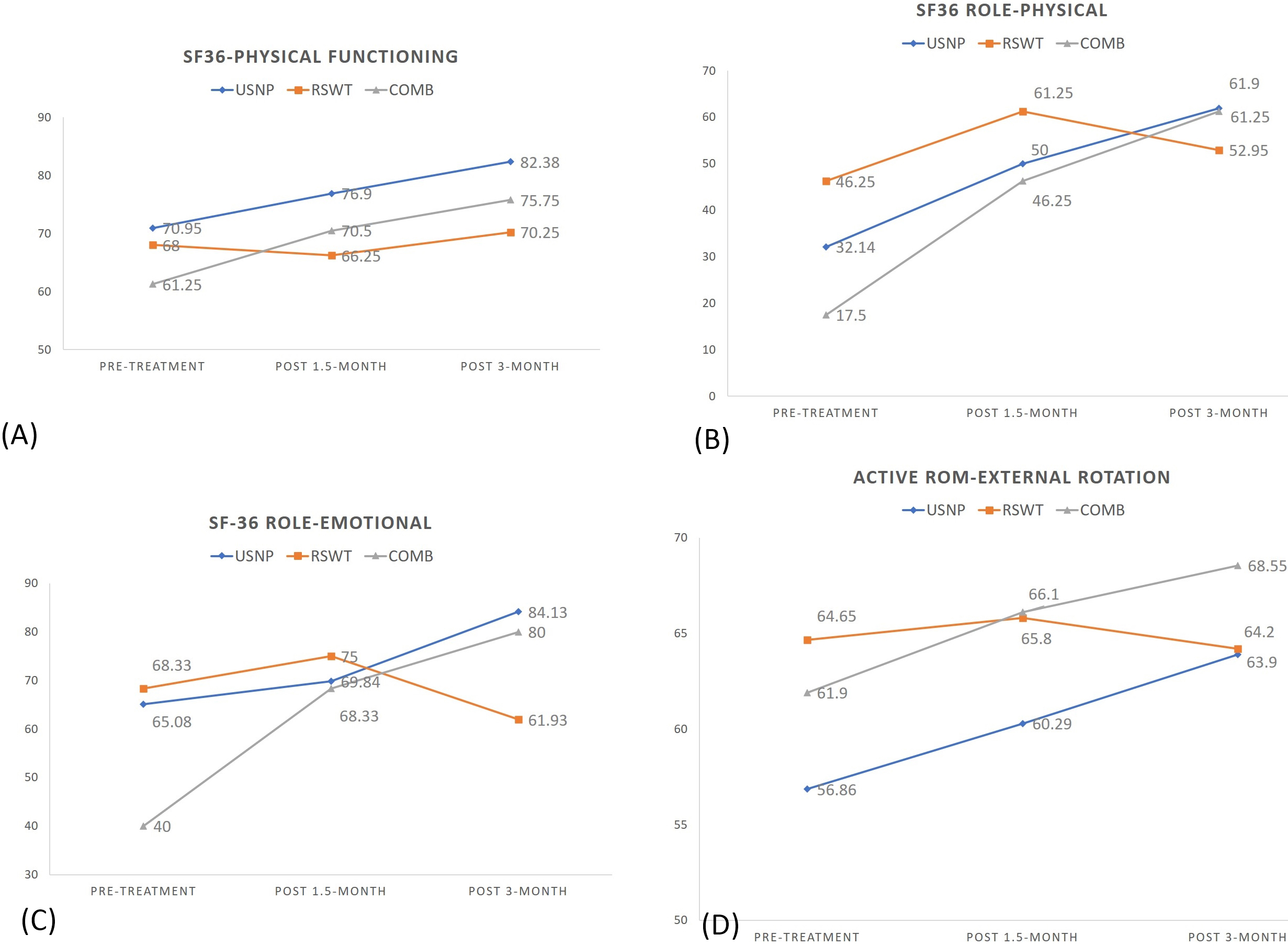
Calcification was observed at the long head of the biceps (1 patient), supraspinatus (53 patients), subscapularis (11 patients), and infraspinatus (10 patients) tendons. Eleven patients exhibited calcification in more than one tendon. The average calcification size was 0.99
Discussion
A comparison between the groups indicated no significant differences in pain and shoulder functioning. Nonetheless, the USNP and COMB groups demonstrated a superior trend in pain VAS scores during activity (Table 3), some SF-36 subscales, and ROM, compared with the RSWT group during follow-up (Fig. 3). The benefits of USNP and the combined treatments could be attributed to several factors. First, USNP utilizes radiation-free image guidance to visualize calcification, thereby facilitating repeated punctures more precisely. Second, the needle’s mechanical breakdown of the calcific deposits could aid the reabsorption of the calcium particles into blood. Third, subsequent shock wave therapy could lead to further disintegration. Additionally, the temporary analgesic effects produced by lidocaine in the subcutaneous tissues and bursa in the USNP and COMB groups might have influenced the outcomes. A 2014 systematic review presented moderate evidence that US-guided needling plus ESWT was more effective than ESWT alone, but evidence regarding a comparison among ESWT, USNP, and combined treatments is limited [25]. A further meta-analysis demonstrated that USNP combined with subacromial corticosteroid injections was more effective than other treatments in terms of the Constant scores, VAS scores, and size of the calcium deposits [26]. To the best of our knowledge, this was the first study comparing RSWT, USNP, and combined treatments for calcific tendinitis of the shoulder.
Krasny et al. compared USNP followed by high-energy shockwave therapy and shockwave therapy alone in an RCT. In that study, shockwave therapy was applied only once for each patient in a fixed amount of 2500 impulses with an energy flux density of 0.36 mJ/mm
On the basis of two studies that compared US-guided needling and shock wave therapy alone, US-guided needling appeared superior to ESWT in restoring functions, providing short-term relief from pain, and accelerating the resorption of calcification [27, 28]; however, corticosteroid injections were provided to the patients in the US-guided needling group in both studies, a practice that differed from the current study. Corticosteroids can suppress inflammation and have possible analgesic effects on neuropeptides, but may cause adverse reactions such as bursa infections, tendon ruptures, and postinjection pain [29]. To eliminate possible adverse events from corticosteroids and focus on the mechanical effect of needling, we only injected lidocaine during US-guided needling.
A statistically significant difference was found in the role-emotional subscale of SF-36 and the active external rotation with time. At baseline, the scores of the role-emotional subscale were significantly lower in the COMB group than in the other groups. Because the patients were not blinded in this study, they may have had expectation bias that influenced their emotions. Although the degree change in patients’ active external rotation was statistically higher in the USNP and COMB groups, the MCID of 13 degrees was not reached [30]. Overall, a superior trend was observed in some SF-36 subscales for the USNP and COMB groups (Fig. 3), but no significant difference was noted in the ROM of the shoulder among the groups.
Because of the widespread use of high-resolution ultrasonography, several studies have examined multiple techniques to approach calcification. Among them, needle barbotage, a procedure involving repeated punctures combined with aspiration, was used most often. This technique can be performed using single or double needles, both of which present favorable outcomes [5]. However, frequent pain and discomfort were reported during the procedure because of the repeated puncturing of the skin’s surface [13]. Additionally, posttreatment complications of US-guided needling, such as frozen shoulder and subacromial bursitis, have been reported, albeit rarely [13]. Zhu et al. compared the effects of USNP with and without aspiration and revealed no significant differences in outcomes [16]. Therefore, we used single needle puncturing without aspiration in the current study to minimize discomfort and the risk of tendon injury.
RSWT has a lower peak pressure and longer rise time than focused shock wave therapy, which could reduce pain during treatment and lower the complication rate [15]. Hence, medium-energy RSWT was applied in the present study [31]. Cacchio et al. reported a high reabsorption rate of calcification after the administration of RSWT in a randomized study; nonetheless, to the best of our knowledge, no study has compared the effectiveness of radial and focused ESWT for treating calcific tendinitis [15].
One limitation of this study was the absence of a control group because of ethical concerns and difficulties in the experimental design. The natural course of calcification reabsorption could not be observed in our study. Therefore, we focused on the effects between combined therapy and a single treatment. Second, the follow-up period was only 3 months; a long-term follow-up may yield a higher resorption rate of calcium deposits [16, 32]. Third, neither the doctors nor patients were blinded because of technical limitations.
Conclusion
In our study, the application of USNP, RSWT, or a combined therapy regimen in the treatment of calcific tendinitis of the shoulder revealed lower pain intensity and improved function during a 3-month follow-up period than at baseline. Although no statistical significance was observed in pain, function, quality of life, or ROM among the three groups, a trend was noted in favor of the USNP and COMB groups. Additional studies with a placebo group, other treatment protocols, larger samples, and longer follow-up durations are required to validate the efficacy of these treatments.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This study was financially supported by Shin Kong Wu Ho-Su Memorial Hospital of Taiwan (SKH-8302-102-DR-33).