
Abstract
BACKGROUND:
Kinesio tape (KT) has been in extensive use for the rehabilitation of injuries related to sports, however, only a handful of studies have focused on the efficacy of KT following extraction of a third molar tooth.
OBJECTIVE:
The study aims to assess whether pain and edema following surgical extraction of the third molar can be reduced by KT.
METHOD:
This research was carried out following the principles of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Web of Science, Embase, PubMed, The Cochrane Library, CNKI, VIP, and WanFang Data databases were searched for trials published from their inception to eighth October 2021. They included published randomized controlled trials in Chinese or English languages. The methodological quality of the included studies was assessed using the Physiotherapy Evidence Database scale. Mean differences (MDs) with 95% confidence intervals (CIs) were used for the analysis of continuous data. The heterogeneity was measured using the
RESULTS:
Eight studies comprising 453 participants in total were included. In comparison to the no kinesio tape group, KT did not furnish improved results on mouth opening ([MD
CONCLUSION:
Despite the fact that KT can reduce pain and has been shown to have positive effects in several studies, there is no convincing evidence that it can reduce the swelling after surgical extraction of the third molar.
Background
Extraction of impacted third mandibular molars is perhaps the most frequently performed surgical intervention for oral and maxillofacial surgery [1]. The decision to do the surgical procedure for the eruption of an impacted lower wisdom tooth must be carefully considered, and potential postoperative complications and contraindications should be carefully evaluated [2]. The swelling of soft tissues, post-extraction pain, and trismus comprise the trio of the most commonly occurring complications that are noninfectious and surface from injury resulting from surgery and associated procedures; thereby traumatizing the periodontal tissues and causing pain and edema. These complications affect the quality of life of patients to a certain extent [3, 4]. Traumatizing methods include the mucosa incision, mucoperiosteal flap disengagement, removing the bone casing, and retracting the surgical field using a surgical hook, generally leading to additional localized stagnation of the lymph [5]. Currently, no safe and effective technique has the potential to reduce the risk of the incidence of the stated complications.
A physical method known as dynamic taping (Kinesio tapeKT) has recently been proposed in the area of oral and maxillofacial surgery to treat some postoperative complications. The activation of the human body’s natural self-healing processes is the precise underlying mechanism for regulating the function of the tape [6]. The therapeutic impact of the tape revolves around improving the blood and lymph flow at the site of its application by tugging the skin away from the subcutaneous tissue and muscles. Through stretching the skin and causing pressure thereby activating the mechanoreceptors via the central nervous system, eventually giving rise to escalated excitability in muscles [7]. Many reports have suggested its benefits on swelling and trismus symptoms following oral and maxillofacial surgery [8, 9, 10]. KT has been claimed to reduce postoperative swelling by creating a space between the fascia layer and dermis, thereby improving lymphatic and blood flow [11]. Their relieving impact on postoperative pain is primarily a consequence of dermal stimulation [12]. The afferent neurons of pain receptors are hypothesized to change into second neurons in the dorsal horn of the spinal cord and transmit pain information via a large number of synaptic connections. The pain afferent fibers of the higher center (cortex and brainstem) reach the dorsal horn of the spinal cord. At the same level, there are mechanical signal afferent pathways of the higher center. Before these signals are transmitted to the center, pain and mechanical signals (such as proprioception) are filtered and integrated. Therefore, there is an inhibitory impact between these pathways. The mechanical receptors in the skin are stimulated when Kinesio tape is placed on the skin. It restricts pain transmission by simultaneously interpreting information and pain into the dorsal horn of the spinal cord [13]. Drugs provide more relief in the first few days following surgery than Kinesio taping, but tapes resolve pain faster by increasing internal fluid flow pressure, which causes a faster reduction in inflammatory mediators [14, 15].
KT has been in extensive usage for rehabilitation of injuries related to sports, however, only a handful of studies have focused on the efficacy of KT following extraction of a third molar tooth [16]. In terms of its effectiveness, meta-research is not based on critical assessments or accusations of individual research. It works by highlighting where and how the research standards and scientific methods across all fields can potentially be improved [17]. Hence, after prioritizing high-impact and high-quality research, we will utilize meta-research to assess whether KT can cause a reduction in edema and pain following third molar extraction surgery.
Methods
Search strategy
The current systematic literature review has been registered under the International Prospective Register of Systematic Reviews (PROSPERO registration number: CRD 42021225241). This review was planned and subsequently coordinated following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [18]. The researchers primarily searched a total of eight databases including Web of Science, Embase, PubMed, The Cochrane Library, VIP, CNKI, and WangFang Data up until eighth October 2021. For the PubMed-based search, the researchers used the following keywords: (“Molar, Third” [Mesh] OR “third molar” OR “third molars” OR “wisdom teeth” OR “wisdom tooth”) AND (“Athletic Tape” [Mesh] OR “orthotic tape” OR “Kinesio tape” OR “Kinesio tape” OR “Kinesio tape”) and searched all fields of studies. There were no limitations set on the search in terms of publishing dates or language. Supplementary Table 1 shows the search method strategy for all eight databases.
Search strategies used in databases
Search strategies used in databases
Two researchers independently screened the literature back-to-back, extracted the data and crosschecked the results. In case of any disagreement, it was settled through discussion or negotiation with a third party.
People requiring their mandibular wisdom teeth to be surgically removed were the main participants of the study. Studies with participating individuals who required the maxillary third molar tooth to be surgically removed at the operation were excluded from this research. Except, that the maxillary third molar was removed and erupted as a simple extraction using forceps or an elevator, or both. The underlying logic was the resulting uncertainty as to which operation led to the reported outcome (e.g., restricted mouth opening, pain, or swelling). Studies enrolling participants that required their mandibular wisdom tooth removal using only forceps or elevators without the elevation of the flap were also excluded.
Types of interventions
Removal of mandibular wisdom teeth using various surgical techniques including lingual nerve protection, surgical flap design, bone removal technique, root retention techniques, wound irrigation technique, suturing techniques, wound closure, the use of surgical drains, and the use of plasma rich protein/plasma rich fibrin (PRF/PRP).
Studies were excluded if any of the following criteria were met: (1) Non-Chinese and Non-English literature; (2) Information in their original form could not be achieved upon contacting the author in case the original data could not be extracted; (3) The literature was based on multiple publications, duplicate records, animal experiments, clinical case studies, or similarly designed studies; (4) or the literature had inconsistent outcome indicators.
Extraction of data and evaluation of literature quality
Two researchers independently and systematically searched the literature in PubMed and EMBASE databases from their inception to eighth October 2021. They extracted the data and the results were cross-checked by employing different sources. If a disagreement arose, it was resolved by negotiation or discussion with a third party. While searching the literature, the title and abstract of a study were read, followed by a full-text reading to identify and decide whether or not the study should be included. The Criteria for the data to be extracted consisted of 1) basic information of the included studies such as the title of publication, first author, publication year, etc.; 2) basic characteristics and intervention measures of the control and experimental groups; 3) key information of bias risk assessment; 4) outcome indicators. The risk of deviation for each qualified study was evaluated following Cochrane reviewer’s manual 5.1.0 [19].
Flow diagram of the selection process.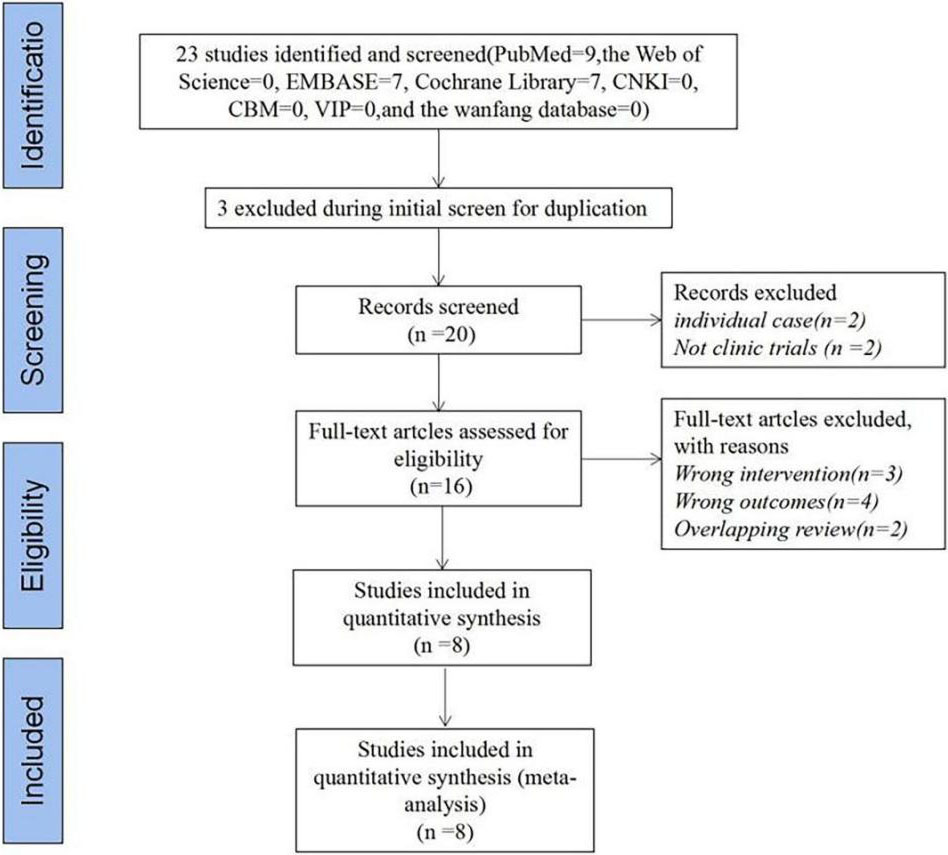
The analyses of the current study were performed using Revman 5.4 software. Odds ratio (OR) and weighted mean difference (WMD) were used for data measurement, with a 95% confidence interval (CI) for statistical analysis. Analysis of the heterogeneity among the included research results was performed through the chi-square test (the test level was
Results
Results of the search
In addition to the studies included in the 2014 Cochrane Review search, we identified 23 new references from the updated searches after using the reference manager software EndNote X9 (Thomson Corporation, Thomson ResearchSoft, USA) for the removal of duplicates, which covered the period until eighth October 2021. Through the Covidence database, the titles and abstracts of the new references were independently and in duplicate reviewed by at least two authors. A total of eight references were discarded at this stage since they were irrelevant to this review (Fig. 1).
Study characteristics
Eight [2027] trials comprised 235 individuals in the experimental group and 218 individuals in the control group. Pain intensity was recorded subjectively using a Visual Analogue Scale (VAS), where zero indicated no pain, five indicated moderate pain, and ten indicated the worst pain. Pain and analgesic usage were recorded on the postoperative first, second, third, and seventh days. Trismus was evaluated by measuring the maximum mouth opening (MMO) between the incisal edges of the upper and lower central incisors using a caliper before the surgery and on the second and seventh days. The facial edema was analyzed using the VAS and by measuring the lengths of the following three lines using a flexible plastic tape measure on the second and seventh days. Detailed information regarding the trials and patients included in this study is presented in Table 2.
Quality assessment
In total, among the eight RCTs, four (57%) studies [20, 22, 23, 26] had reported random sequence generation, five (71%) studies [20, 21, 22, 23, 26] reported the use of allocation concealment methods, whereas two (28%) studies [22, 25] reported the blinding methods for participants and personnel; and three (42%) studies [20, 21, 25] mentioned blinding methods for outcome assessments. Figure 2(A) and (B) summarize the bias risk together with an evaluation of its consistency.
Primary outcome
Mouth open
As shown in Fig. 3, five studies [22, 23, 24, 26, 27] had
Main characteristics of the eight studies included in the meta-analysis
Main characteristics of the eight studies included in the meta-analysis
Outcome: ⟀ 3dMD swelling ⟁ interincisal distance ⟂ operative times ⟃ pain intensity ⟄ ecchymosis ⟅ mouth-opening values ⟆ edema.
(A) Risk of bias summary: review of the authors’ judgments about each risk of bias item for the included studies, (B) risk of bias graph: review of the authors’ judgments about each risk of bias item presented as percentages across all included studies. Note: Each color represents a different level of bias: red for high risk, green for low risk, and yellow for unclear risk of bias.
a total of 342 cases, with homogeneity between the studies (
Forest plot of the comparison of the mouth open between the experimental and control groups.
As shown in Fig. 4, four studies [20, 24, 25, 26] had a total of 125 cases. The results of the heterogeneity tests of the included literature show a significant heterogeneity (
The results from the random effect model were as following: [MD
Forest plot of the comparison of the swelling (after seven days) between the experimental and control groups.
Forest plot of the comparison of the operation time between the experimental and control groups.
As shown in Fig. 5, five studies [20, 21, 23, 24, 26] had a total of 193 cases. The result of the heterogeneity test showed no heterogeneity among the studies (
Edema
As shown in Fig. 6, four studies [20, 22, 23, 27] had a total of 282 cases. The result of the heterogeneity test was
Pain intensity (after 24 hours)
As shown in Fig. 7, seven studies [21, 22, 23, 24, 25, 26, 27] had a total of 408 cases. The result of the heterogeneity tests of the included literature showed a significant heterogeneity (
The results from the random effect model were as following: [MD
Forest plot of the comparison of the edema between the experimental and control groups.
Forest plot of the comparison of the pain intensity (after 24 hours) between the experimental and control groups.
Funnel plot of publication bias of pain.
The funnel chart provided by the review manager software is used to evaluate whether there is significant publication bias in the literatures included in the meta-analysis. The effect value RR of the total effective rate of the treatment group and the control group is the abscissa, and the ordinate is the standard error of the logarithm of RR (selogRR). The funnel plot showed obvious asymmetry, which demonstrated that there was a publication bias in the pain of the included studies (Fig. 8). However, considering that the total number of included articles is only eight the results of publication bias may be prejudiced. The possible causes of publication bias are related to the implementation of the randomized scheme, allocation concealment, and blind method.
Discussion
A lower third molar surgical extraction is a typical oral surgical procedure performed frequently. Owing to the phylogenetic transformations that occurred within the jawbones, there has been a constant increase in the incidence of preservation of third molars. This has led to a noticeable increment in the medical requirements that necessitate extracting wisdom teeth surgically [28, 29, 30]. Non-infectious postsurgical complications are the most common consequence of this procedure and may include trismus, facial swelling, and pain after tooth extraction. In immunocompetent patients, the danger of developing infectious complications is, however, low. Nevertheless, numerous noninfectious complications such as trismus, swelling of the soft facial tissues as well as postextraction pain are very frequent during the postoperative period.
Following surgical wisdom tooth extraction, a minimally invasive method focused on preventing noninfectious complications is required. The dynamic taping method (Kinesiology taping) may qualify as one such technique lately, which was only in use in medical treatment following sports injuries [31, 32, 33]. The specific weight, extensibility, and thickness of the tapes are more or less identical to the characteristics of the epidermis [34, 35, 36]. At present, there has been only a limited amount of research that deals with KT in the maxillofacial area, particularly focusing on the third molars in the mandible [37]. The introduction of dynamic taping techniques to the surgical removal of the mandibular third molar was first made by Ristow [38]. Since then, quite a few authors have reported the various taping techniques employed in their research. Several authors utilized a modified method of KT application since the new method was reported to have improved efficacy in minimizing postoperative complications in comparison with the classical technique [16]. Menziletoglu and Genc evaluated the application of surgical drainage and KT, respectively, after impacted mandibular tooth extraction. Both studies reported that the two therapies significantly reduced postoperative discomfort. However, regarding postoperative satisfaction, the results from the two studies are inconsistent [39, 13].
Few publications focused on the impact of patients’ age and time duration of the surgical eruption of wisdom teeth upon the severity of jaw compression, edema, and pain following surgery [40]. Since the study and control groups employed in this work were not different in terms of age and duration of surgery, it is rather safe to conclude that the application of Kinesio tape patches only resulted in an impact on parameters such as mouth opening, swelling, and pain.
In total, 453 patients from a total of 8 randomized controlled trials were included in this systematic review and meta-analysis, which is based on the evaluation of the benefits and efficacy of Kinesio tape in patients following surgical extraction of the third molar. Based on the current meta-analysis, we have concluded that in terms of ease of mouth opening and reduction in swelling, Kinesio tape does not have a clinical or statistical advantage over no Kinesio tape. However, Kinesio tape showed a reduction in operation time edema, and pain favoring the Kinesio tape group. Overall, the size of this effect was found to be small to moderate.
Compared with Wang’s review [41], the evaluated three indicators (pain, swelling, and restricted mouth opening). The funnel plot indicated no publication bias, and the combined results of this meta-analysis are reliable and robust. This meta-analysis evaluated five indicators (pain, swelling, restricted mouth opening, operation time and edema), regardless Kinesio tape can reduce the pain, operation time and edema, there isn’t any convincing evidence regarding Kinesio tape can reduce the swelling after surgical extraction of the third molar. The funnel plot indicated publication bias and the results of this study showed that some of the outcome indicators are heterogeneous The plausible reasons are as follows: 1) the literature included in this study are from different countries around the world, and the population and course of the disease may be different; 2) The KT, techniques of application, therapist experience, and treatment time of different research treatment options are different; 3) the researches included in the study also had obvious differences in sample size and document quality; 4) Since there is no standardized recovery for the third molar after extraction, there is no specific standard for the pasted method and course of treatment of the Kinesio tape used in the literature, and the outcome indicators and measurement methods are entirely different.
There are some definite limitations to this meta-analysis. Firstly, the analyses are rather limited owing to the number of eligible randomized controlled trials. Secondly, only short-term results have been reported by most studies; hence, our meta-analysis is based entirely on the short-term impact of KT. Additionally, most of the studies involved in this analysis were published in different countries, indicating that the methods for employing KT vary by region and country, and the regional differences will also affect the treatment effect. Besides, the results of the studies could have been altered by the high heterogeneity. Though the included studies had a quality ranging from moderate to high, some important aspects, for instance, the sample size and power of studies, have not been evaluated by the physiotherapy Evidence Database scores. Several studies included in this meta-analysis had relatively limited sample sizes since the results should be interpreted attentively.
Conclusion
Although KT resulted in a reduction in pain favoring the KT group following surgical extraction of the third molar, there is a lack of direct scientific evidence about its edema. Upcoming projects should plan to achieve adequate, clear, and precise results by acquiring an appropriate sample size, adequate study design, and proper statistical analysis, thus improving the quality of the research to see if the KT really can reduce postoperative complications, especially in terms of pain and edema. Clinicians should concordantly pay attention to these limitations when utilizing KT for patients.
Author contributions
Conception and design: Jing Qi, Haiquan Yue, Jiahui Chen
Administrative support: None
Provision of study materials or patients: All authors
Collection and assembly of data: Haiquan Yue, E Liu
Data analysis and interpretation: Jing Qi, Haiquan Yue, Jiahui Chen
First draft of manuscript writing: E Liu, Guang Chen, Yuting Liu
Final version and approval of manuscript: All authors.
Funding
This study was supported by the Science-Technology Foundation for the health care industry of Gansu Province of China (Grant NO: GSWSKY2020-77) and Key Discipline project Fund of Gansu Provincial Hospital of China (Grant NO: 18GSSY1-7) and Science-Technology Foundation for the health care industry of Gansu Province of China (Grant NO: GSWSKY2020-17).
Footnotes
Conflict of interest
The authors declare that they have no competing interests.