
Abstract
BACKGROUND:
Vibration training is an adjuvant to muscle-strengthening exercises.
OBJECTIVE:
To investigate the short-term effects of direct vibration on the deep trunk muscles of patients with non-specific chronic low back pain (CLBP).
METHODS:
Participants with non-specific CLBP were randomly placed into two groups: the vibration-plus stabilization exercise (VSE) group (
RESULTS:
Ultrasonography revealed that the ratio of muscle thickness to contraction and relaxation was statistically increased after exercise in the bilateral transversus abdominis (TrA) and lumbar multifidus (LM) muscles in the CSE group (
CONCLUSION:
Direct vibration can increase the selective activity of contracting deep trunk muscles.
Keywords
Introduction
Spinal stabilization training is a well-known therapeutic method that is commonly used in clinical practice. The main goal of stabilization exercises is to improve neuromuscular control, strength and the endurance of central muscles, and to maintain dynamic spinal and trunk stability [1]. Various studies with long-term outcomes have shown that stabilization training as a single or combined modality improves pain intensity and disability and prevents the recurrence of chronic LBP (CLBP) episodes [2, 3].
Previous studies have examined the application of physical training, including vibrations, based on improvements in neural adaptation and reflex modification mechanisms [4]. Bosco et al. first reported an increase in leg strength when they analyzed the acute effect of vibration as an exercise modality on strength [5]. Since then, many studies have reported the positive impact of vibration on muscle strength and performance [6, 7, 8]. However, little is known about the effects of vibration exercises on the clinical symptoms of patients with CLBP. One comparative study analyzed the impact of spinal stabilization exercises, including whole-body vibration at 25 Hz for 2 weeks, and found no significant difference in the endurance of the multifidus muscle with or without vibration [9].
Two different vibration methods, indirect or direct, have been used to apply vibration in previous vibration training studies. The method used to apply vibration can affect the intensity of the vibration load on the trained muscle, as well as its magnitude, amplitude, and frequency [10]. Nevertheless, no previous studies or clinical trials have reported spinal stabilization as a result of direct vibration of the trunk muscles. Direct vibration has the advantage of selective muscle strengthening compared to the indirect method. The hypothesis of this study is that local direct vibration application is effective for selective activation of the deep trunk muscles required for spinal stabilization exercises in patients with non-specific CLBP.
Materials and methods
Design and participants
To analyze the effect of direct vibration on trunk muscles, we assessed the maximal and rested trunk muscle contraction after applying direct vibration during stabilization exercise. We measured the patients’ anatomical and electrophysiological features using a randomized comparative study design. We measured the contracted and rested muscles using ultrasonography and surface electromyography. The participants performed preprogrammed spinal stabilization exercises and three visits were scheduled to measure trunk muscle contraction. The protocol was approved by the Institutional Review Board of the Korea University Anam Hospital in Korea (KCT0003858; registered on 26 April 2019). Each participant signed a written informed consent form prior to participation. All procedures were performed in accordance with the relevant guidelines, including the Declaration of Helsinki.
Participants were enrolled in a single center from May to December 2019, based on the following inclusion criteria: non-specific CLBP for
Participants were excluded if they displayed symptoms of recognizable pathologies such as infection, malignancy, inflammatory disease, structural deformity, overt neurologic signs, history of trauma, abdominal or lumbar surgery, or pregnancy (suspected or confirmed). The exclusion criteria from the clinical trial were deterioration of back pain, severe physical or physiological damage, refusal of the patient, drastic reduction of compliance, non-attendance of three or more sessions, and any intervention of other treatments.
We used random allocation because the subjects’ tasks or living environments could not be controlled. The participants were randomly allocated to groups at a 1:1 ratio by an independent data manager using a computer-generated randomization list. The subjects were enrolled in the order they were diagnosed with non-specific CLBP and were approved for participation in this study. Because the participants were clearly aware of the vibration itself even though they did not know in advance whether the device was vibrating or not, the data were exchanged without identifying the subjects between the physical therapist, variable measurer, and data analyst; consequently, a single blind study was applied.
Participants (
Flowchart showing subject recruitment and randomization. CLBP 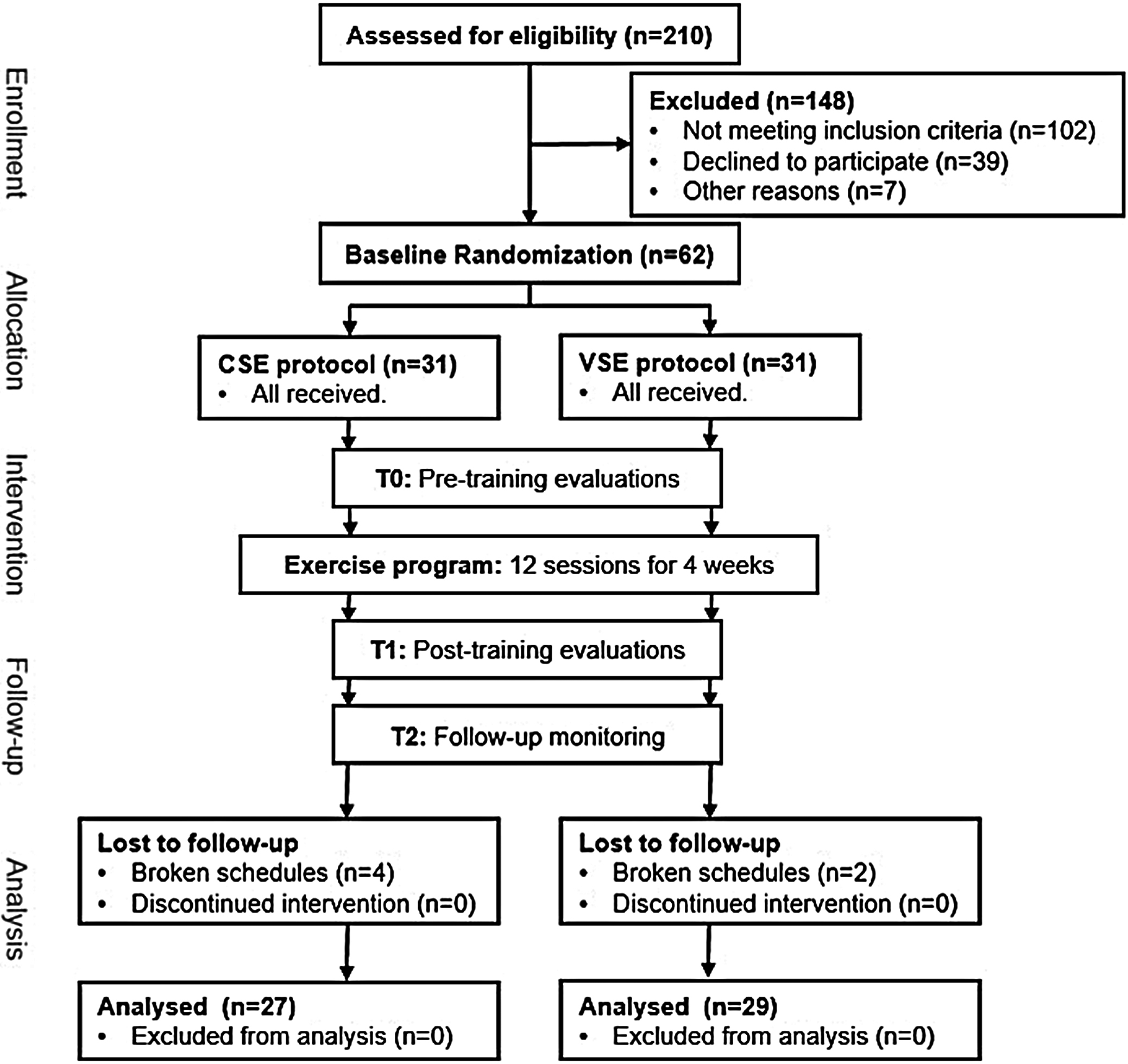
Spinal stabilization exercise program consisted of five different exercises: upper-body extension (A), alternate arm and leg lift (B), alternate arm and leg extension (C), diagonal curl-up (D), and curl-up (E).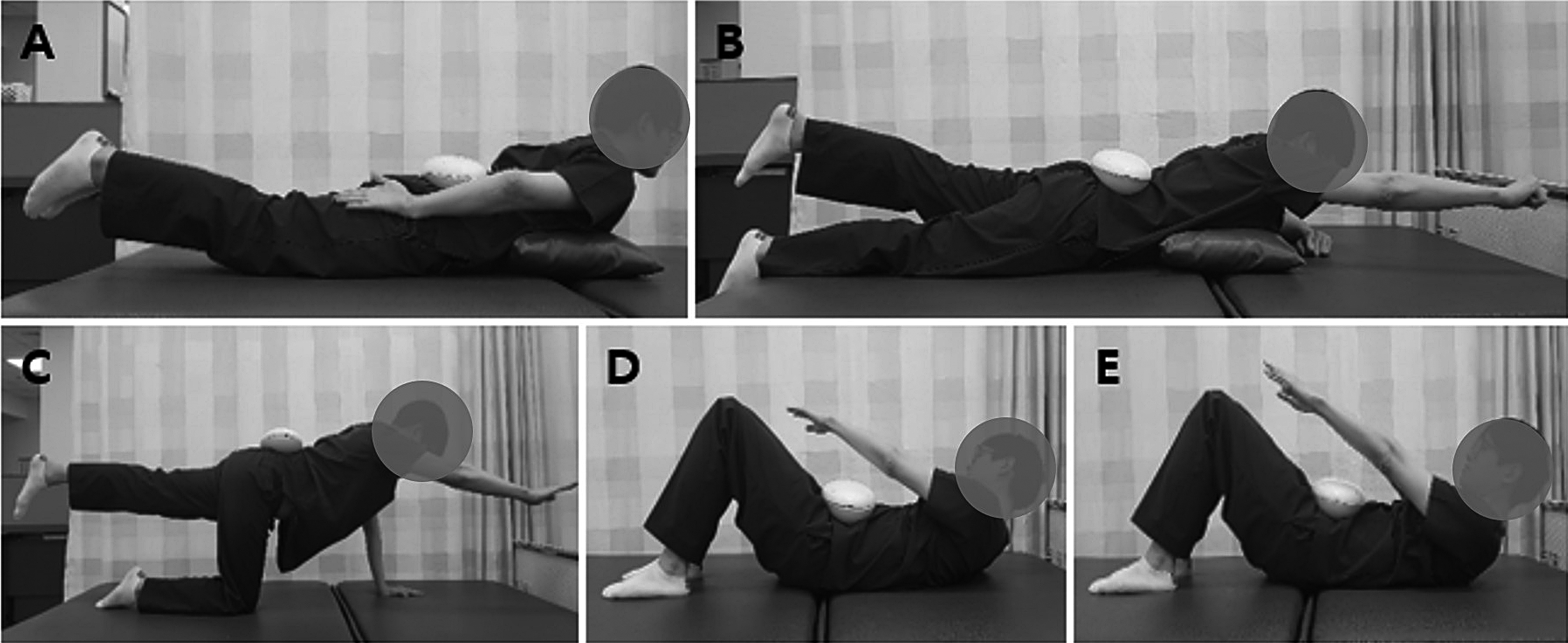
The spinal stabilization exercise protocol for the rehabilitation of patients with CLBP is based on commonly advocated spinal stabilization exercises [12, 13, 14]. The spinal stabilization exercise program consisted of five exercise types repeated in each session, including upper-body extensions, alternate arm and leg lifts, alternate arm and leg extensions, diagonal curl-ups, and curl-ups. The subjects exercised three times a week in our gym under the supervision of two physical therapists with more than 10 years’ experience. The therapists varied the order and amount of exercise according to the subject’s compliance, but applied all five types of exercise. The therapists helped the subjects to maintain accurate postures for 10–15 s and encouraged the completion of the 30-min exercise protocol, including warm-up, cool-down, and proper rests (Fig. 2).
We designed and manufactured a vibration device (330
Patients’ clinical and demographic characteristics (
56)
Patients’ clinical and demographic characteristics (
CSE, conventional stabilization exercise; VSE, vibration stabilization exercise; SD, standard deviation; BMI, body mass index; VAS, visual analog scale; ODI, Oswestry disability index (%).
Ultrasonographic images were taken of the rectus abdominis (RA), external oblique (EO), internal oblique (IO), transversus abdominis (TrA), lumbar erector spinae (LES), and lumbar multifidus (LM) muscles at the L4/5 level during both resting and activation states. We determined the patients’ position and transducer location based on previous studies. Briefly, halfway between the anterior superior iliac spine and the ribcage along the mid-axillary line to the EO, IO, and TrA; halfway between the umbilicus and xyphoid process to the RA; and paravertebral muscles adjacent to the spinous process line at the level of the posterior iliac crest lines to the LES and LM [15, 16]. We measured the thickness of the contracted EO, IO, and TrA during an abdominal drawing-in maneuver (ADIM) of the RA during curl-ups, and of the LES and LM during maximal resistive lumbar extension on prone [17]. We calculated the change in muscle thickness due to contraction for all muscles using the following equation: [thickness ratio
We recorded the muscle activity of the bilateral EO, IO, TrA, RA, LES, and LM muscles using surface electromyography (sEMG). We determined the patients’ positions and testing protocol based on previous studies [18]. We positioned electrodes on the abdominal muscles (EO, IO, TrA, and RA muscles) according to McGill [19]. We placed the electrodes on the LES muscles by positioning them 4 cm laterally from the L4 spinous process at the level of the iliac crest [20]. For the LM muscles, we placed the electrodes above the posterior superior iliac spine on the spinous processes of the lumbar and sacral vertebrae [21, 22]. We verified the quality of the EMG signal to ensure correct electrode placement [23], and used reference voluntary contractions (%RVCs) to normalize muscle activation. Raw EMG data were collected using the wireless EMG system TeleMyo 2400R, which was connected to a Noraxon Myosystem 1200 unit (Noraxon, Scottsdale, AZ, USA) with a sampling rate of 1000 Hz. The mean muscle activity was expressed as the percentage of RVC. We calculated the ratios of muscle activation as the %RVCs of IO relative to RA (IO/RA ratio), TrA relative to RA (TrA/RA ratio), and LM relative to LES (LM/LES ratio).
Pain intensity was measured using a visual analog scale (VAS), which has been shown to have linear scale properties for pain intensity. We evaluated the CLBP-correlated functional disability using the Korean version of the Oswestry Disability Index (ODI), which consists of ten items that evaluate pain intensity and interference with typical physical activities. The duration of the data measurements was 12 weeks. Pain and disability levels were assessed at T0 (initial), T1 (after 4 weeks), and T2 (after 12 weeks).
Statistical analysis
All statistical analyses were performed using SPSS (version 22.0; SPSS Korea Data Solution Inc., Seoul, Korea). Wilcoxon’s signed-ranks tests were employed to compare the muscle thickness ratio, sEMG data, disability level, and pain intensity of the subjects before and after training, and Mann-Whitney U tests were used to identify any significant differences in the baseline data between the two groups. We also used a repeated-measures analysis of variance (rm-ANOVA) to determine the presence of a temporary interaction of the three measures within each group. Assumptions about the normality of the data distribution and homogeneity of variance were evaluated. Assumption of sphericity was tested by Mauchly’s sphericity test. We presented three epidemiologic and measured variables and two explanatory variables of symptoms in a regression analysis of each group. Statistical significance was set at
Pain and disability data before versus after training
Pain and disability data before versus after training
Ultrasonographic muscle thickness ratios (contracted/rest) for the trunk muscles of patients in the CSE (A) and the VSE (B) groups. 
A total of 56 patients (27 in the CSE group and 29 in the VSE group) completed the full exercise program and evaluation. The clinical and demographic data of the participants are summarized in Table 1. There was no statistically significant difference in the baseline data between the two groups (
We calculated the thickness ratios (contracted/rest) of each muscle. In the CSE group, the thickness ratios of the left IO, bilateral TrA, and LM muscles were statistically increased before and after exercise. In the VSE group, we found a significant increase in the left EO, bilateral IO, TrA, and LM (Fig. 3).
The activation of the right RA, bilateral EO, IO, and LM was significantly increased in the CSE group. In the VSE group, we measured significantly higher levels of activation in the bilateral IO, TrA, and LM. Moreover, the bilateral LM/LES ratios in the CSE group and the bilateral IO/RA, TrA/RA, and LM/LES ratios in the VSE group were significantly increased (Fig. 4).
Multiple regression analysis of epidemiologic and measured data for efficacy of VAS and ODI in the CSE group
Multiple regression analysis of epidemiologic and measured data for efficacy of VAS and ODI in the CSE group
The ratio of muscle activation (IO/RA, TrA/RA and LM/LES muscle activities) in the CSE (A) and the VSE (B) groups. 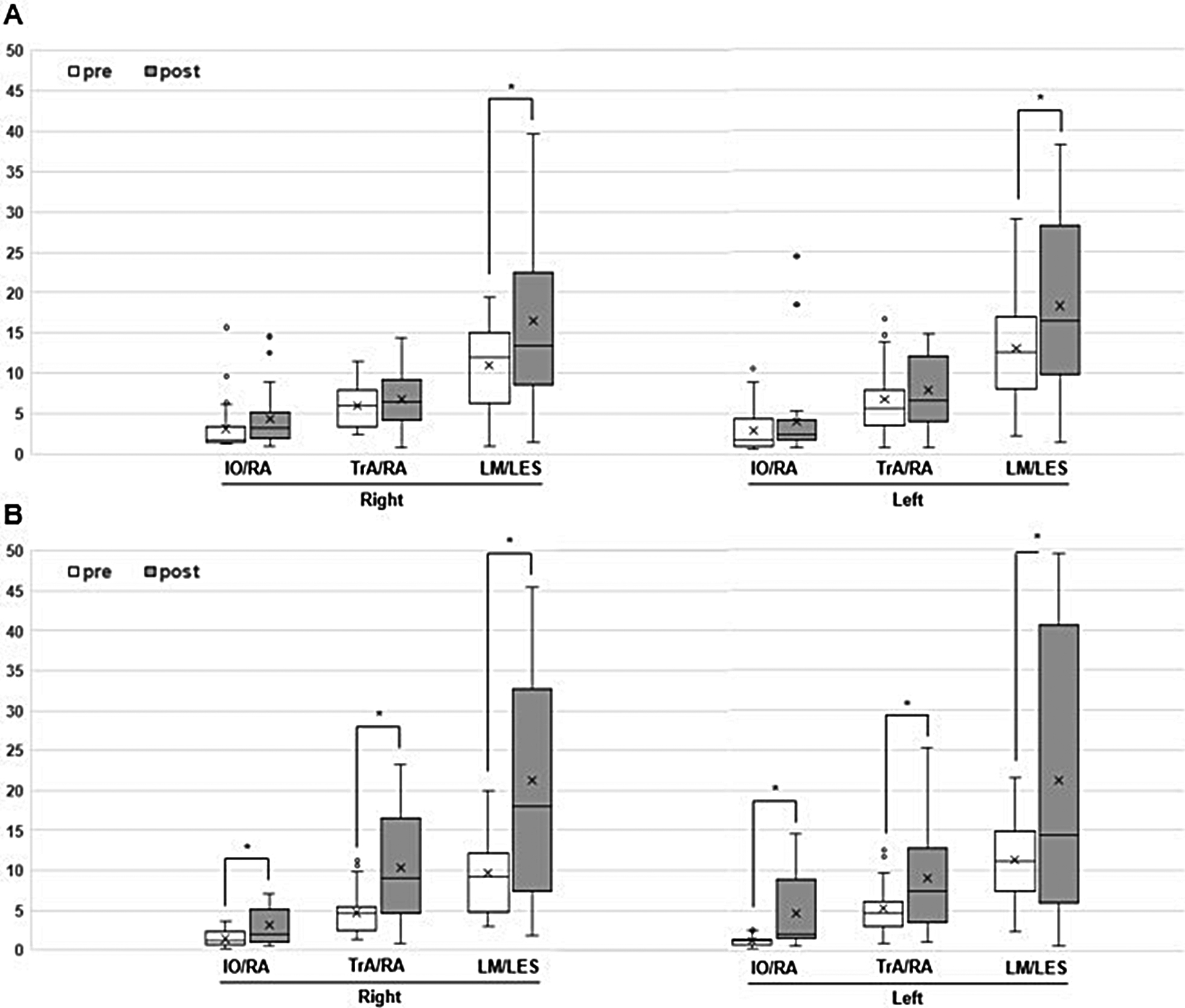
We used a multiple linear regression model to analyze the factors influencing the VAS and ODI efficacy, which was calculated using the following formula: [Efficacy
Multiple regression analysis of epidemiologic and measured data for efficacy of VAS and ODI in the VSE group
This study was performed to investigate the clinical effects of vibration on direct application of human body surface to influence static and dynamic muscles of lumbar spine. In the patients with non-specific LBP, the pain intensity and the related disability were decreased in both groups with and without the vibration after the five common core stabilization exercises. Ultrasonographic examination revealed the ratio of the muscle thickness to the muscle contraction and relaxation before and after the intervention. The thickness ratio of TrA and LM muscles showed statistically significant difference in the CSE group. In the VSE group to which the vibration was applied, the thickness ratios of the TrA, LM, and IO muscles were statistically different. The results of the surface EMG evaluation were more remarkable. Statistical differences in post-treatment muscle activity in the CSE group were significant in both EO, IO, and LM muscles. On the other hand, the statistical difference in the VSE group was found in both TrA, IO and LM muscles. When calculating the ratio of muscle activity, the CSE group showed statistically significant difference in both IO/RA, and the VSE group showed a statistically significant increase in all three ratios of muscle activity; IO/RA, TrA/RA and LM/LES ratios. These results indicate that the direct vibration stimulation applied at the same time as isomatric contraction during spinal stabilization exercise relatively improves the activity of muscles located in the more deeper region such as static muscles.
Spinal stabilization exercises are a single application that can be used as an effective adjuvant therapy for patients with CLBP. An exercise protocol that includes stability exercises has been reported to help reduce the pain and disability of patients with CLBP. Several studies on the impact of therapeutic exercise on patients with CLBP have focused on stabilization through the reinforcement of trunk muscles such as the TrA and the LM. In particular, researchers have stated that the coordinated activity of the deep paraspinal muscles plays an important role in fine-tuning the intersegmental mobility of the spine [24]. We considered the available data to design a proper and compatible eight-session exercise protocol over a period of 4 weeks.
Whole-body vibration (WBV) using specific frequencies is a treatment technique that is currently marketed for LBP. It has been suggested that WBV can help to improve LBP by promoting a stretch reflex action and by strengthening trunk muscles, which are known to be weak in patients with LBP [25, 26]. Previous studies have shown that WBV at frequencies below 20 Hz may reduce LBP by reducing spasms in the paravertebral muscles [27, 28]. However, the method used for WBV relies on indirect vibrations applied to the lumbar region, which can cause perturbations at a systemic level.
The effectiveness of short-term WBV training on improving lower limb muscle strength, power, and functional mobility of subjects has been reported [29, 30, 31]. Some studies have demonstrated that WBV intervention rapidly increases muscle activity during exposure using sEMG records [32, 33, 34, 35]. In addition, there are reports of deviations in activity between functional muscle groups. It has been reported that WBV had a greater influence on the isometric muscle activity of the flexor muscles in the knee than the ankle, and another study reported that WBV improved knee extensor muscle strength selectively at low frequencies ranging from 2–20 Hz [36, 37]. Recent meta-analysis suggested based on several reports that WBV significantly strengthens knee extensor muscle power with some additional exercise, but does not strengthen knee flexor muscle power [38].
Vibration therapy on muscles and tendons is administered by direct or indirect methods [39, 40]. Indirect vibrations are usually applied using vibration platforms, dumbbells, and vibratory motors attached to resistance training machines and cables. On the other hand, direct vibrations are applied with electromotor devices that need a direct contact on the body. Focal vibrations on the musculoskeletal system can be applied to specific muscles or tendons and have tried to use for relief of focal spasticity due to upper motor neuron lesion [41, 42]. However, there are few reports on the impact of strengthening and stabilizing the coordinated function of the trunk muscles on motor control by direct vibration.
Mischi et al. performed a meaningful study on indirect focal vibrations. The authors delivered 28 Hz vibration stimulation on the elbow flexor and extensor muscles during isometric contractions using a belt and found that this system caused a low-level co-contraction of the muscles [43]. This was probably due to the increase of vibration-induced muscle activity and motor unit synchronization and the alteration of muscle spindle sensitivity. This mechanism resembles the well-studied tonic vibration reflex, which is a physiologic response to a mechanical vibration applied to muscles or tendons which can cause a reflex muscle contraction through Ia fibers [44]. Based on this theory, some studies have reported that vibration applied at a certain frequency to limb muscles or tendons located at the extremities enhanced synchronization [6, 45]. The study of Issurin et al. is noteworthy as it established the acute and residual effects of vibratory stimulation during explosive strength exercises. The vibration was applied focally on the biceps brachii muscle using an indirect method. The authors reported that the significant difference in the muscle response between elite and amateur athletes was associated with the higher sensitivity of the muscle receptors and the central nervous system of elite athletes due to additional stimulation [46]. Core stabilization exercise using a sling with vibratory stimulation is similar to a direct method and it is based on regional vibration stimuli. The vibration generator is connected to the harness via a sling rope, which is in contact with a part of the body. The design of this system is also associated with the clinical efficacy of various vibration treatments based on the existing tonic vibration reflex (TVR) theory [47]. In a comparative study using this system on healthy subjects, the authors reported a significant increase in the activity of trunk muscles [48].
To our knowledge, there has been no study on the effect of direct focal vibration on the contraction of trunk muscles. This was part of an effort to find an efficient core stabilization exercise method that any patients could do on their own. Sling exercises associated with vibration stimulation is effective and has good compliance, however, it is difficult to implement at home.
In addition, a comprehensive review of existing studies suggests that the TVR effect is influenced by muscular facilitation. In other words, TVR is expected to augment the motor stimulation in the contracted muscle and increase its force. Mischi et al. also reported a similar phenomenon and showed differences in the EMG activity of the elbow flexor and extensor muscles after upper extremity exercises with vibration stimulus. The researchers introduced this as an interesting observation and concluded that this was a preferred neural strategy for the more commonly used flexors in daily activities [43]. Further studies will confirm whether the vibrational effects are selectively occurring during muscular contraction and relaxation.
Study limitations
This study has several limitations. First we could not control the variability of physical vibration. To promote the compliance of the patients in the VSE group, we applied the vibrations in a relaxed state before initiating the treatment and set the intensity and frequency at a level acceptable for the subject. Therefore, the frequency and intensity applied to each subject were different. Further research should be carefully designed to control this variable and assess the physical quantities of vibration applied to the human body. Second, we could not evaluate the sustainability of the vibration effect as self-exercise of the subjects was not controlled between T1 and T2. Finally, we could not reevaluate sEMG; this issue requires an independent research design.
Conclusion
In this study, we showed that direct and focal vibration stimulation during trunk muscle contraction through stabilization exercises significantly changed the muscle activity pattern. This finding has important implications for future research. The precise control of vibrations and anatomical considerations are still needed to establish evidence for the effects of vibration on neurophysiological mechanisms.
Footnotes
Acknowledgments
This work was supported by the Korea Medical Device Development Fund grant funded by the Korean government (The Ministry of Science and ICT, the Ministry of Trade, Industry and Energy, the Ministry of Health & Welfare, and the Ministry of Food and Drug Safety) (Project number: 1711138408, KMDF_PR_ 20200901_0189).
Conflict of interest
None to report.