
Abstract
BACKGROUND:
The relationship between the endurance of the lumbar paraspinal muscles and morphological changes needs to be clarified. In this context, the importance can be revealed of increasing the endurance level of the paraspinal muscles in the prevention and treatment of low back diseases.
OBJECTIVE:
The aim of this study was to examine the relationship between the clinical evaluation results of the cross-sectional area (CSA) and fat infiltration of the lumbar deep paraspinal muscles.
METHODS:
The study included 37 patients with mechanical low back pain (mechanical), 41 patients with lumbar hernia without root compression (discopathy) and 36 healthy individuals as a control group. The functional status of the lumbar deep paraspinal muscles was evaluated clinically with muscle endurance tests. The fat infiltration and CSA of the muscles were evaluated on axial MRI sections at the L3-S1 level.
RESULTS:
The mean values of the prone bridge, Biering-Sorenson, and trunk flexion tests were seen to be highest in the control group and lowest in the discopathy group (
CONCLUSION:
The study results demonstrated that the endurance of the paraspinal muscles is associated with the fat infiltration of the muscles. In patients with chronic low back pain, information about muscle morphology and degeneration can be obtained with simple endurance tests without the need for further measurements. On clinical examination, a weak endurance level of the paraspinal muscles indicates the presence of a low back problem and an increase in the amount of fat infiltration.
Introduction
Lumbar and spinal muscles provide support to the spine, allowing the body movements to be controlled. The deep back muscles play an important role in this control; deep dorsal muscles, deep upper layer (erector spinae
The different anatomic structure, function and unisegmental innervation feature of the L.MF make this muscle more vulnerable to damage than the other lumbar paraspinal muscles [7, 8]. Functioning of the back muscles is a prerequisite for spine rigidity and optimal control of movement. It has been reported that just as in lower back pain (LBP), the structure and function of the paraspinal muscles are affected by pain and injury [2]. Important studies have been conducted which have evaluated changes in the structure and function of several back muscles, including the L.MF and L.ES, and have shown varying results [7, 9, 10, 11, 12, 13, 14].
Two main findings in muscle degeneration are a reduction in muscle size and increased fat accumulation [7]. Studies have shown that there is a relationship between chronic low back pain and increased fat infiltration of the paraspinal muscles. Several studies have shown atrophy in the deep fibres of back muscles, especially the L.MF, fat infiltration, and connective tissue accumulation [7, 9, 10, 11, 15, 16, 17], and while some of these studies have reported fat infiltration in both the L.MF and L.ES [16, 17, 18, 19, 20], others have reported it only in the L.MF [7, 21]. It has been demonstrated that patients with chronic low back pain have a smaller multifidus cross-sectional area (CSA) [7, 8, 9, 11, 18, 21, 22, 23, 24, 25, 26]. In some studies, a smaller CSA has been reported in the psoas and quadratus lumborum muscles together with the L.MF [22]. However, many researchers have reported no significant differences in paraspinal muscle size (CSA) [16, 19, 24, 27, 28, 29] or fat content compared with healthy individuals [12, 28, 30, 31, 32].
Despite the inconsistencies in the literature, current data support the view that in patients with chronic low back pain, the paraspinal muscles are smaller on the symptomatic side than on the asymptomatic side compared to healthy individuals [2, 33]. In paraspinal muscle atrophy that has formed due to denervation and non-use, denervation is thought to be the primary factor initiating degeneration in the muscles. Denervation leads to progressive degeneration of contractile muscle fibers in skeletal muscle, rapid atrophy with the sheath of the muscle mass, increased fat infiltration in the muscle, and muscle fiber type changes [34, 35]. Of the muscle LBP, changes in the movement patterns (deep fibres of the L.MF protecting from weight-bearing) following the inhibitor and regeneration (acute period) and inflammatory (subacute period) processes, have been stated to form associated with loss of resistance force of the muscles and non-use (chronic period) [2].
Muscle endurance is the measure of the muscle’s ability to apply repetitive force and the duration of this activity. According to the American Department of Health and Human Services, muscle endurance is the ability of the muscle to maintain activity without fatigue [36, 37]. Studies have shown that endurance tests that do not require advanced technology have high reliability, are inexpensive, and can be easily applied for clinical use [38, 39]. It has been stated that muscle dysfunction and failure are widespread in patients with chronic low back pain, and compared to the healthy population, there is less muscle strength and endurance in the paraspinal muscles and greater fat content [16, 32, 40, 41]. The functional status of the lumbar muscles during pain has been studied experimentally [42, 43]. Previous studies have shown that the muscle fibre type changes form in LBP patients, with a decrease in type I muscle fibres and an increase in type II muscle fibres, resulting in a smaller muscle area and lower resistance to fatigue [44, 45]. Evidence of chronic LBP has shown decreased activation of L.MF deep fibres and increased activation of several muscles for protection of the spine and of the deteriorated muscle structure of the L.MF in particular and other paraspinal muscles [2].
In the literature there are different approaches to trunk muscle endurance with muscle morphological changes. The results are somewhat inconsistent in respect of function. While some of those studies have reported that trunk muscle strength is lower in patients with chronic low back pain than in healthy control subjects [46, 47, 48, 49, 50, 51, 52, 53], others have stated that no difference could be found [21, 54, 55, 56, 57]. Therefore, the aim of this study was to shed light on the protective and therapeutic approaches for mechanical low back pain and lumbar disc hernia by revealing the relationship between endurance tests of the paraspinal muscles and CSA and fat infiltrations.
Method
Participants
This prospective observational study was conducted between February-April 2021, and included 37 patients with mechanical back pain (mechanical group), 41 patients with lumbar hernia without radiculopathy (root compression) (discopathy group) and 36 healthy individuals (control group). According to the analysis of variance power test results, considering the average values of CSA, the minimum sample size to be included in the study was determined to be 78, with 95% confidence (
The mechanical group included patients who presented at the Orthopaedics and Traumatology Polyclinic of the hospital with complaints of low back pain ongoing for at least 3 months, determined as mechanical low back pain (non-specific low back pain) with no additional lumbar pathology determined in the physical examination, laboratory tests and radiology tests (no determination of lumbar discopathy on MRI). The discopathy group included patients with low back pain ongoing for at least 3 months, who did not describe root compression-related radicular pain and had no examination findings, for whom EMG was requested to reveal compression when root compression was suspected, and were determined with lumbar discopathy only on MRI with no findings of root compression. In the physical examination for the differential diagnosis, the specific orthopaedic tests for lumbar segmental instability (paravertebral intervertebral movement test, prone instability test) and the specific tests to reveal radiculopathy in lumbar hernia (straight leg raise test, contralateral straight leg raise test, Laseque test, femoral nerve tension test) were negative. There was no sensory loss and no loss of strength associated with nerve root compression in any of the patients.
In the radiological examination, no findings were determined on direct radiographs suggestive of fracture, deformity, infection, or neoplasm. On MRI, hernia types were classified as central, paramedian, foraminal and extraforaminal according to the position of the protruding part of the disc, and as bulging, protrusion, extrusion or sequestration on the basis of the degree of protrusion [58, 59, 60]. As the patients in this study did not have radiculopathy, an MRI-based nerve compression grading system was not necessary.
Pain intensity was assessed using a standard 100 mm visual analog scale (VAS), and all patients recorded pain intensity
LBP was defined as pain between the lower border of the costa and the gluteal fold. Patients were excluded from the study if they had a posture disorder affecting physical activity, cerebrovascular disease, a history of trauma or serious musculoskeletal disease, metabolic, neoplastic, infection, neurogenic, or inflammatory diseases (rheumatoid arthritis, ankylosing spondylitis etc.), previous lumbar operations, vertebral fracture, or structural deformity (leg shortness, spondylolisthesis, scoliosis, kyphosis).
Healthy individuals were invited to the control group through announcements and social media, and were randomly selected from volunteers who had not had any back pain in the last year, had no back problems in examination and radiology, and had not participated in active sports in the last three months.
Demographic, disease-related, and clinical data were obtained from face-to-face anamnesis in all groups. A detailed physical examination was performed, and tests for erythrocyte sedimentation rate, complete urinalysis, hemogram, Brucella, Salmonella, Anti-Streptolysin O (ASO), C-Reactive-Protein (CRP), and Rheumatoid Factor (RF) were requested for differential diagnosis in patients when deemed necessary. MRI was performed on all patients.
Lumbar spine MRIs were analyzed by a radiologist with spine MRI experience, who was blinded to the clinical history. The MRI scans were taken by a single radiology technician. All patients were examined by a single physician (Orthopedics and Traumatology specialist) experienced in spine surgery. Informed consent was obtained from all the participants before inclusion. The study was approved by the Ethics Committee of the Scientific Research Board of Near East University (YDU/2021/87-1272).
Measurements
Magnetic resonance imaging
Imaging was performed with a 1.5 Tesla MR device (Signa Explorer SV25.3 16 channel, up-to-date software, General Electric, Milwaukee, WI, USA). Shots were taken with the patient positioned supine, with a routine protocol for the lumbar spine with the measurement level between L3-S1 (L3-4/L4-5/L5-S1) at the center of the disc (Fig. 1). Turbo spin-echo T1 and T2 weighted sagittal and turbo spin-echo T2 axial 4 mm sections parallel to the disc spaces were taken. The fat content and CSA of the lumbar musculus multifidus and erector spinae were measured bilaterally at 3 levels (L3-4/L4-5/L5-S1), with each level examined separately. Evaluations were made on T2 axial sections. In the evaluation, both right and left sides of all levels were averaged.
A healthy control group subject: L4-L5, T2 sagittal and axial MRI slices.
MR imaging provides non-invasive information about muscle CSA and fat infiltration. It is usually applied when disc problems, tumor, stress fracture, and infection are suspected. When muscle-related changes have been evaluated, MRI has been found to be reliable [15, 16, 61]. In the current study, the CSA was measured quantitatively by determining the fascia boundaries of the muscles (epimysium) and drawing them manually using PACS Report imaging. Fat infiltration of the muscles was evaluated semi-quantitatively as Grade 1: fat infiltration up to 10% of the muscle CSA (normal), Grade 2: 10–50% fat infiltration (moderate), and Grade 3:
Muscle localisations and fat infiltration grades on T2 axial MRI slice MF: Musculus multifidus, ES: Musculus erector spina, and (A) Grade 1: 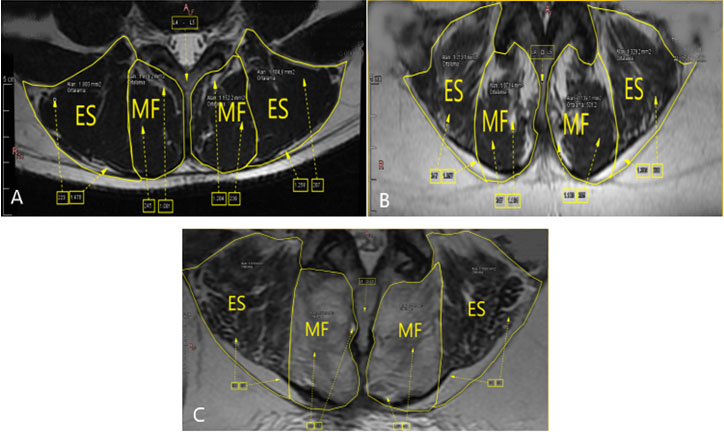
For intraobserver reliability, CSA and fat infiltration of the paraspinal muscles were re-evaluated one month later by the same radiologist in 11 randomly selected patients, and the resulting kappa value was 0.945 (0.899–0.993).
The Biering-Sorensen test was used to evaluate the endurance of the back extensors [63], the lateral bridge test to evaluate the endurance of the spinal stabilizer muscles [64], the plank (prone bridge) test to evaluate the trunk endurance [65], and the trunk flexor endurance test to evaluate the trunk flexor muscle endurance [64]. The time for which the participants could maintain the test positions was recorded in seconds. Trunk flexors were added to the endurance test for this study because the transverse abdominis activates the system as the first muscle to contract in spinal stability and creates a key point. The tests were carried out under the supervision of the same physiotherapist in a standard way, with a 1-minute rest break between each test.
Statistical evaluation
Data were analyzed with IBM SPSS V23 software (IBM Corp., Chicago, IL, USA). Conformity of the data to normal distribution was examined using the Shapiro Wilk test. The Chi-square test was used to compare categorical variables according to the groups. The Mann-Whitney U test was used to compare data that were not normally distributed according to paired groups. In the comparisons of three or more groups, One-way analysis of variance was applied to normally distributed data, and the Kruskal Wallis test to non-normally distributed data. The three-way MANOVA was used to compare CSA values by group, gender, and segments, and multiple comparisons were made with the Bonferroni test. Two-way MANOVA was used to compare test times by group and gender, and multiple comparisons were made with the Duncan test. Relationships between quantitative data that were not normally distributed were examined with Spearman’s rho correlation coefficient. Quantitative data were stated as mean
Comparison of the age, gender, BMI (body mass index), and pain duration of the patients according to the groups
Comparison of the age, gender, BMI (body mass index), and pain duration of the patients according to the groups
Comparison of endurance tests of the groups
Descriptive statistics of endurance tests by group and gender
The demographic characteristics of the participants are given in Table 1. The groups were similar in respect of age, BMI, duration of low back pain, and gender.
The average values of the prone bridge, Biering-Sorenson, and trunk flexion test were highest in the control group and lowest in the discopathy group (
In the control group, in the prone bridge test there was determined to be a statistically significant negative correlation with left L.MF (
The relationships between endurance tests and Right L.MF, Left L.MF and Right L.ES, Left L.ES cross-sectional areas (CSA) between the groups
The relationships between endurance tests and Right L.MF, Left L.MF and Right L.ES, Left L.ES cross-sectional areas (CSA) between the groups
Spearman’s rho correlation coefficient,
The relationship between fat infiltration and endurance tests
The relationships between right, left L.MF and right, left L.ES fat infiltration and endurance tests are shown in Table 5. The Biering-Sorenson test results differed according to fat infiltration in the right L.MF, and the lowest time was obtained at
The median values of the trunk flexion test also differed according to fat infiltration (
There was a significant difference between the groups in respect of CSA (
In the analysis of the relationship between age, BMI, duration of low back pain and CSA, there was a statistically significant positive correlation between BMI in the L3-L4 segment and right-left L.ES (
Comparison of fat infiltration values according to the groups
Chi-square test
When the relationship between age, BMI, duration of low back pain and test times was examined, a negative correlation was found between lateral bridge, prone bridge, Biering-Sorenson, trunk flexion tests, and age (
The comparisons of the fat infiltration values of the paraspinal muscles according to groups are shown in Table 6. Right and left L.MF fat infiltrations differed according to the groups (
In the comparison of age, BMI, duration of pain, and fat infiltration values, a correlation was found between right L.MF and BMI (
The results of this study demonstrated that the endurance level of the trunk muscles was better in the control group compared to the mechanical and discopathy groups, while the fat infiltration of the paraspinal muscles and related muscle atrophy was higher in the mechanical and discopathy groups compared to the control group. The chronic period in LBP is a period of conduction loss and failure in the muscle. Atrophy in the muscle and muscle fibres, fibrosis, increased fat infiltration, reduced muscle strength and resistance, and muscle failure have been reported to be seen in this period. It has been stated that this creates a permanent repetitive circular vicious cycle with each triggering the other [2, 7, 21, 45]. These determinations can be explained by the results of the study as stated above.
In all the groups, no significant difference was determined between the CSA and endurance values of the L.MF and L.ES. This was thought to be due to the pseudohypertrophy mechanism of the muscles. The real muscle mass (functional muscle mass
Spinal muscles are designed for activity throughout the day. However, since inactivity and pain change the functions of the spinal muscles, they become tired in the normal position and protective activities are impaired [66]. Fatigue is associated with endurance, and individuals with acute and chronic low back pain have a shorter endurance time than healthy individuals [67]. Noonan et al. stated that there was paraspinal muscle dysfunction and failure in patients with chronic low back pain [6]. Studies have also shown that LBP patients have back muscles that tire in a shorter time than those of healthy control subjects [68, 69, 70, 71]. In a one-year retrospective study, Sorensen stated that good isometric endurance of the back muscles reduces the risk of low back pain [63].
Studies examining the relationship between trunk muscle endurance and paraspinal muscle degeneration in LBP patients are limited. Hutman et al. reported that in individuals with chronic low back pain, the muscle density of the erector spinae decreased significantly and the duration of trunk muscle endurance was shortened in individuals with chronic low back pain compared to healthy individuals, but there was no significant difference between the groups in terms of L.ES CSA and body composition [32]. In a study on healthy males by Gibbons et al., no relationship was determined between the CSA and the endurance level of the erector spinae muscle [72]. Sung et al. stated that L.ES muscle endurance was lower in LBP patients than in healthy control subjects [73]. Danneels et al. reported that gentle lordosis coordination exercises showed low activity of the L.MF, and during high-load exercises, lower activity was seen in all the back muscles [52]. In a study by Newton et al., patients with chronic low back pain were reported to have higher levels of pain and disability and lower trunk strength [46]. These findings in previous studies are similar to the current study results that the mean endurance values were highest in the healthy individuals and lowest in those with discopathy.
In obese individuals, body fat normally accumulates in the muscles along the back musculature, but not at the level of the last two lumbar vertebrae where most spinal problems are common. The presence of fat infiltration in this area, where most of the spine problems are common, suggests that it is the back pain that initiates the muscle changes [62]. In a 15-year follow-up study, Fortin et al. showed that fat infiltration was mostly seen at the L5-S1 level, and that greater fat infiltration was associated with muscle weakness and functional level [10]. Similarly, the current study results showed that most fat infiltration was detected at the L5-S1 level in patients with herniated disc and mechanical back pain.
It was observed in the current study that the endurance level in the discopathy group was lower than that of the mechanical group. Although there is no similar study in the literature for comparison, this result can be considered to be due to prolonged non-use resulting from the longer pain duration in the discopathy group.
Males in all the current study groups had longer muscle endurance times and less fat infiltration than females. It has also been previously stated in the literature that the paraspinal muscles of males have less fat infiltration than in females [8, 62].
The lower level of fat infiltration of the paraspinal muscles of males is thought to cause fewer back problems than in females. The fact that individuals with mechanical and discopathy groups have more fat infiltration compared to the control group suggests that the degeneration of the paraspinal muscles is associated with low back pain [9, 17, 20, 27]. The treatment strategies seen to be required in chronic LBP are those which increase the activation of decreased L.MF deep fibres and decrease the activation of increased superficial L.MF and L.ES. In individuals with low back pain, the level of muscle endurance is related to degeneration of the paraspinal muscles, and to be able to reverse this situation, patients should be treated with an appropriate exercise program (motor control exercises, specific motor control exercises, general exercises) by adjusting the exercises to the individual (because of interpersonal differences in the structure and functions of the back muscles) [2, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84].
Conclusion
The results of this study demonstrated that fat infiltration of the paraspinal muscles and associated muscle atrophy were related to chronic low back pain and lumbar herniated disc. This relationship seems to be based on degeneration of the paraspinal muscles related to a decrease in muscle endurance. Evaluation of endurance measurements of LBP patients is clinically important in respect of providing infomation about regional muscle morphological changes and the level of disease. Increasing the level of endurance and providing follow up may be effective in preventing or reducing the level of degeneration of the paraspinal muscles. While a sufficient level of endurance may protect healthy individuals against LBP, it can also improve and prevent the progression of the disease in individuals with LBP.
Footnotes
Acknowledgments
The authors would like to thank Radiology Specialist, Doctor Kerim Temiz for his contributions to the interpretation of patient MRI scans, technician Halil İbrahim Efe, who performed the MRI scans, and application specialist İbrahim Yesilyurt who helped adapt the MRI device for the study.
Conflict of interest
None to report.