
Abstract
BACKGROUND:
Shoulder disability is a common problem following neck dissection. Even if nerve structures are preserved, this may occur after the surgery.
OBJECTIVE:
The primary aim was to research changes in rotator cuff and scapular muscles strength, and scapular muscle endurance after neck dissection in patients with head and neck cancer. The secondary aim was to investigate the relationship between these changes and postoperative shoulder function.
METHODS:
This cross-sectional and prospective follow-up study included 14 patients who underwent neck dissection (9 unilateral and 5 bilateral). Evaluations were performed preoperatively and at 3 months postoperatively. Muscle strength measurements, including trapezius, serratus anterior, and rotator cuff muscles, were obtained using a handheld dynamometer. The scapular muscle endurance test was used for muscle endurance assessment. Postoperative shoulder function was evaluated using Constant-Murley shoulder score.
RESULTS:
A decrease in muscle strength and the scapular muscle endurance test was found at 3 months postoperatively, except for the subscapularis muscle strength (
CONCLUSIONS:
Muscle strength and scapular muscle endurance may reduce following neck dissection. These reductions are associated with postoperative shoulder function. Thus, muscle strength and endurance training may be beneficial for early postoperative rehabilitation in patients with head and neck cancer.
Introduction
Head and neck cancer (HNC) occurs in several anatomic sites including the larynx, pharynx, oral cavity, nasal cavity, paranasal sinuses and thyroid [1]. Incidence rates of HNC, excluding thyroid malignancies, range from 0.34–3.81/100,000 for females and 2.32–23.15/100,000 for males in different countries [2]. Long term survival can be achieved in about two-thirds of patients with multidisciplinary treatment approaches, including surgery, radiotherapy and chemotherapy [1, 3].
Neck metastasis is the primary factor in determining HNC prognosis and, currently, neck dissection (ND) is the best method for control of cervical metastasis [4]. ND is a surgery where dissection of the anterior and lateral neck is done to remove the tumor and cervical lymph nodes. Applied dissection types are radical, modified radical and selective ND [4]. In radical ND, cervical lymph nodes, the spinal accessory nerve, the internal jugular vein and the sternocleidomastoid muscle are removed. In modified radical ND, cervical lymph nodes are removed sparing at least one of the non-lymphatic structures including the spinal accessory nerve, the internal jugular vein and the sternocleidomastoid muscle. In selective ND, all non-lymphatic structures including the spinal accessory nerve, the internal jugular vein and the sternocleidomastoid muscle are spared [5].
However, various complications resulting from ND may occur due to many vital structures located in the neck. Nerve injuries are among possible complications. One of the structures that may be affected is the spinal accessory nerve (SAN) [6].
SAN may be damaged by manipulation, traction, thermal injury due to electrocautery, and even more rarely by division of the nerve during surgery [7]. Disruption of the trapezius muscle innervation provided by SAN results in shoulder disability which is described as “shoulder syndrome” on the affected side. Common characteristics are shoulder pain, limitation of shoulder abduction range, full passive shoulder range of motion, shoulder drop, protruding scapula, prominence of other shoulder muscles except for the trapezius muscle, abnormal electromyographic signals and lack of radiographic abnormalities [8]. The prevalence of shoulder pain in the radical ND was higher than the modified radical and selective ND. The incidence of reduced shoulder active range of motion depends on the type of surgery and varies between 5% and 20%. Shoulder dysfunction is observed in more than 70% of patients after ND [9]. Shoulder morbidity associated with ND is substantial for patients with HNC [10]. This dysfunction may lead to difficulties in activities of daily living and may negatively impact on quality of life [11].
The cervical plexus also supports motor innervation of the trapezius muscle apart from SAN, but it may be sacrificed during the surgery [12]. However, patients with preserved nerve structures may have different levels of shoulder disability [13]. This is thought to occur due to the indirect trauma rather than direct SAN damage during ND. Affected trapezius and scapulohumeral muscles lead to deteriorated biomechanical relationship between glenohumeral and scapulothoracic joints [12] which are normally regulated by active control of these muscles [14]. Altered muscular strength and endurance may affect shoulder functions. Impairment of shoulder function can lead to decreased performance of activities of daily living and deteriorated quality of life in patients with HNC [15].
Most studies in the literature focused on the trapezius muscle for evaluation of shoulder dysfunction after ND [16, 17, 18]. Due to the biomechanical interaction of the shoulder girdle, weakness of the trapezius muscle may affect serratus anterior muscle activation [19]. This is because these two muscles, which support scapular stability and mobility, interact as the force couple [20]. Changes in scapular stabilizers reflect on glenohumeral muscles, including rotator cuff, in that these synergistic muscles contribute coordinated movement between scapula and humerus. The scapula constituting a stable basis for rotator cuff muscles supports glenohumeral mobility for proper shoulder function [20]. However, there are few studies focusing on muscles other than the trapezius after ND [21, 22]. Moreover, most of the studies in this population focused on muscle strength, and information regarding assessment of muscle endurance is insufficient. To the best of our knowledge, no published research has looked at the relationship between scapular and rotator cuff muscles strength and scapular endurance measures, and shoulder dysfunction level after ND in patients with HNC. Therefore, the primary aim of this study was to determine the changes in rotator cuff and scapular muscle strength, and scapular muscle endurance following ND. The secondary aim was to investigate the relationship between these changes and postoperative shoulder function.
Methods
Study design and data collection
This cross-sectional and prospective follow-up study was conducted from December 2018 to January 2020 at the School of Physical Therapy and Rehabilitation, Dokuz Eylül University. Data of the patients with HNC who received planned ND was collected preoperatively and at 3 months postoperatively [23] by the same physiotherapist. Since it was reported in a study that spinal accessory nerve dysfunction may occur in the first 3 months after ND, regardless of the type of dissection [24, 25, 26], this period was chosen as the earliest time for postoperative evaluation. In addition, this period was selected to preserve the integrity of the musculoskeletal structures after ND, and to enable the patients to provide adequate function in muscle strength and endurance tests.
The study was approved by the Clinical Research Ethics Committee of Dokuz Eylül University (Protocol number: 306-SBKAEK, Approval number: 2018/13-06).
Participants
Patients were recruited from the Department of Otorhinolaryngology, Dokuz Eylül University Hospital into the study. A study flowchart is summarized in Fig. 1. Fourteen patients who underwent ND (9 unilateral and 5 bilateral) were included, nine with unilateral shoulder affection and five with bilateral shoulder affection. All participants were informed about the study and a written informed consent form was obtained from all of them. The inclusion criteria were (1) the decision to perform ND with diagnosis of HNC; (2) age
Study flowchart.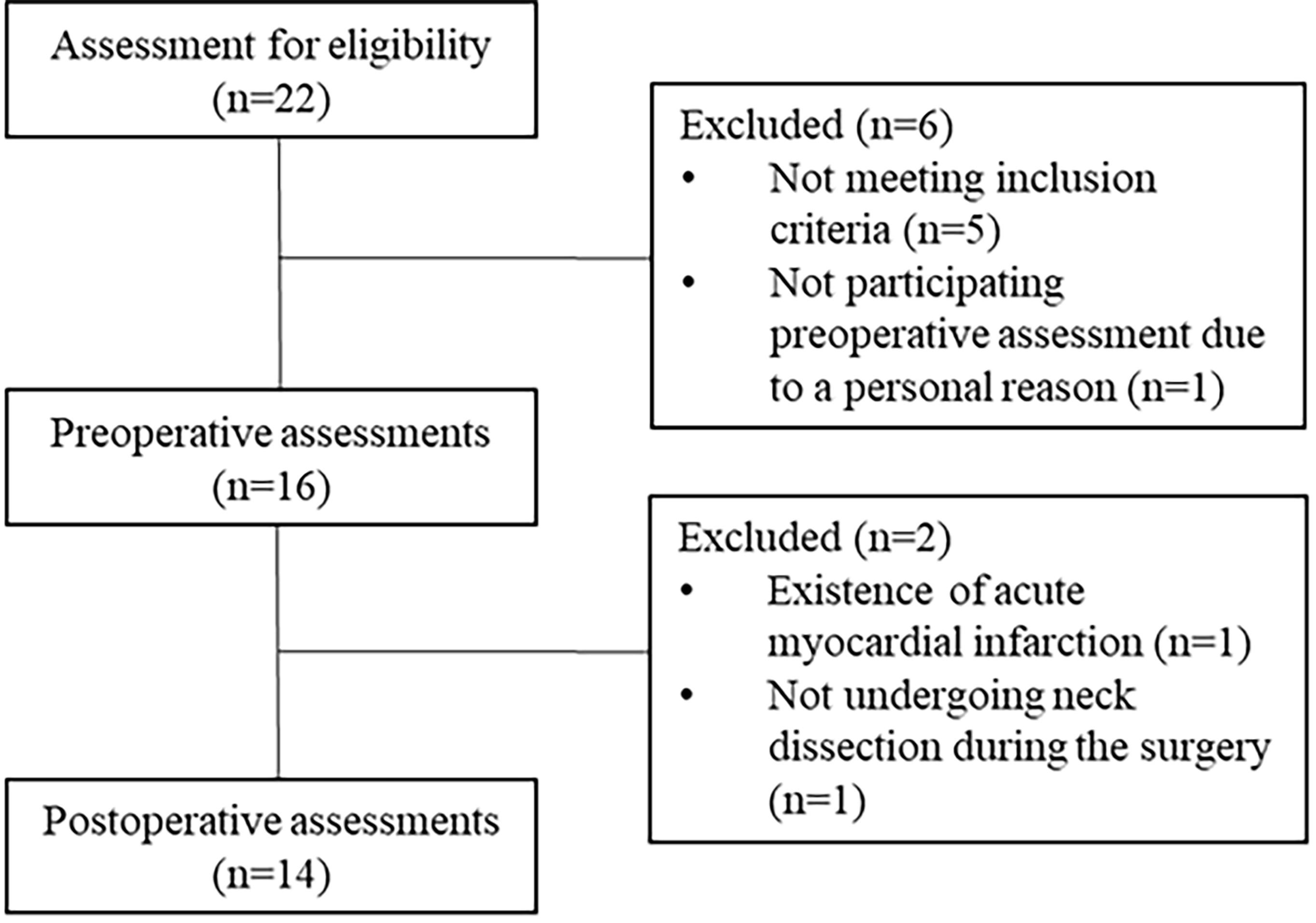
Muscle strength
Isometric strength of the trapezius, serratus anterior and rotator cuff muscles composed of infraspinatus/teres minor, subscapularis and supraspinatus muscles were assessed using a handheld dynamometer (Lafayette Instrument, Lafayette, IN, USA). Participants were asked to exert maximum effort against resistance of the dynamometer during the test. While a 30-second rest period was given between each trial of the same muscle group, an approximate one-minute rest period was given between different muscle groups. Each muscle group was tested three times. The average of three trials was used for data analysis and the results were recorded in kilograms [28]. The results were recorded as 0 kilograms for muscle groups that did not achieve the test position and were not able to withstand force against resistance of the dynamometer. While the upper trapezius, serratus anterior, infraspinatus/teres minor, subscapularis, and supraspinatus muscles were evaluated in a seated position on a chair without back support, the middle and lower trapezius muscles were tested in prone position.
Upper trapezius muscle
The head of the participant was positioned in lateral flexion to the same side, rotation to opposite side, and extension. The dynamometer was placed on top of the shoulder. While the resistance was applied to the head with one hand, inferiorly directed resistance was applied to the shoulder with the dynamometer [29].
Middle trapezius muscle
The shoulder of the participant was positioned in horizontal abduction, full extension and external rotation. The dynamometer was placed on the spina scapula about one third of the distance from the acromion to the root of the spina. Anterolateral directed resistance was applied [28].
Lower trapezius muscle
The shoulder was positioned in 140
Serratus anterior muscle
The shoulder was positioned in 125
Infraspinatus/teres minor and subscapularis muscles
After the shoulder was placed in 30
Supraspinatus muscle
There is no difference between “full can” test described as 90
Scapular muscle endurance
The scapular muscle endurance test (SMET) was used to evaluate the isometric endurance of the scapular muscle as described by Edmondston et al. [32]. After shoulders and elbows were positioned in 90
The position of the participant for the scapular muscle endurance test.
Constant-Murley shoulder score (CMSS) was used to evaluate shoulder function. CMSS consists of subjective parameters, including pain (15 points) and activities of daily living (20 points), and objective parameters, including range of motion (40 points) and strength (25 points). Total score ranges from 0 to 100 and lower scores state worse shoulder function [33].
Statistical analysis
SPSS software version 24.0 (IBM Corp., Armonk, NY, USA) was used for all statistical analysis. Descriptive statistics were presented as median and interquartile range for continuous variables, and frequency and percentage for discrete variables. The results of muscle strength and endurance before and after ND were compared by the Wilcoxon signed-rank test. The Spearman rank correlation coefficient was used to analyze the relationship between postoperative shoulder function and the percentage changes in muscle strength and endurance. The level of correlation was interpreted as: 0.00–0.19 – “very weak”; 0.20–0.39 – “weak”; 0.40–0.59 – “moderate”; 0.60–0.79 – “strong”; 0.80–1.0 as “very strong” [34]. Post-hoc power analysis was performed using G*Power (version 3.1.9.7) to determine whether the study had adequate power. The significance level was set as
Results
A total of 14 patients, nine with unilateral shoulder affection and five with bilateral shoulder affection, were enrolled and evaluated. Demographic and clinical characteristics of the participants are presented in Table 1. There were no patients whose SAN was sacrificed. There were decreased muscle strength and scapular muscle endurance in the postoperative period, except for the subscapularis muscle strength (Table 2). Postoperative CMSS was strongly correlated with percentage decline in middle trapezius, lower trapezius, serratus anterior muscle strength and SMET. It was also moderately correlated with percentage decline in infraspinatus/teres minor, subscapularis, and supraspinatus muscle strength (Table 3). A post-hoc analysis for the current study showed a power of 93.6% for the scapular muscle endurance and 80.2% for the shoulder function data (primary outcomes). The effect sizes were 0.84 (large) and 0.68 (medium), respectively.
Demographic and clinical data of participants
Demographic and clinical data of participants
IQR: Interquartile range.
Comparison of muscle strength, scapular muscle endurance, and shoulder function before and after neck dissection
Wilcoxon signed-rank test, IQR: Interquartile range,
Correlation between the shoulder function and percentage changes in muscle strength and scapular muscle endurance
rho: Spearman rank correlation coefficient,
To our knowledge, this is the first study to investigate changes in scapular and rotator cuff muscle characteristics (strength and endurance) at three months after ND, and the relationship between these changes and postoperative shoulder function in patients with HNC. The findings suggest that therapists should consider not only changes in rotator cuff and scapular muscle strengths, but also scapular muscle endurance parameters that may be related to shoulder function after ND in this population.
Decreased muscle strength and muscle endurance were determined after the ND, except for subscapularis muscle strength. Furthermore, moderate to strong correlations between changes in muscle performance and shoulder function were found.
Impairment of shoulder function is related to shoulder disability following ND [15]. The maintenance of normal shoulder functions is provided by proper interactions of active, passive and control subsystem structures in patients with HNC. Instability of the control subsystem - consisting of the nervous system - reflects on both active subsystem structures consisting of muscles, and passive subsystem structures consisting of joints, fascia and spine. One of the control subsystem structures is SAN [35]. Even though shoulder disability may occur after the surgeries where SAN is sacrificed, it may also appear when the nerve is preserved [13]. Even if the nerve is not directly damaged, it may be affected due to different degrees of traction stress during surgery. In these patients, trapezius muscle activity may decrease [25]. Thus, assessment of shoulder function is important for all patients undergoing ND even if the nerve is preserved during the operation.
Studies which investigated shoulder function in patients with HNC have focused on muscle strength, especially the trapezius muscle [16, 17, 18], with rotator cuff muscles rarely being examined [21, 22]. Many studies found weakness of the upper, middle and lower trapezius muscles, as well as shoulder abductors and external rotators in a case series mostly including patients with SAN palsy after ND [16]. Patients evaluated by manual muscle testing had decreased shoulder elevation and abduction strength at least 6 months after ND [36]. The study of Remmler et al. found reduced upper and middle trapezius muscle strength in patients with and without preservation of the SAN, who were given a physical therapy program to maintain shoulder range of motion after ND. In this study, muscle strength was evaluated by manual muscle testing [17]. In another study, 34–39% decline in isometric shoulder flexion strength, as evaluated by a dynamometer, was determined following ND [37]. Exercise programs focused on the range of motion might be insufficient to preserve the muscle strength. A different study did not observe changes in muscle strength, including scapular elevation (the upper trapezius muscle), scapular adduction (the middle trapezius muscle), scapular depression and adduction (the lower trapezius muscle) in spite of affected electromyography results at 21 days and 6 months after level 2b-preserving selective ND [18]. Electromyography results indicated moderate and mild injuries, respectively, in the early and late postoperative period. These results may have been due to the fact that the clinical picture did not settle completely in the early postoperative period and disappeared in the late period. Participants undergoing three different ND types, consisting of radical (
Decreased muscle strength may result in rapid fatigue, and muscle fatigue may affect scapular stabilization [38] which may lead to a change in scapular muscle endurance in the current study. However, it is not known whether the scapular muscle endurance changes occur after ND in the current literature. The median of SMET was determined as 95.0 (70.0–124.0) seconds in a study that examined the normative values for scapular muscle endurance in healthy individuals with a median age of 21.5 years [39]. However, SMET scores were lower than normative values in both preoperative and postoperative periods in the current study. This may be explained by high median ages of study participants. In the literature, it was emphasized that progressive resistance exercise training may improve muscle endurance in patients with HNC [40]. In a study, patients who had an anastomosis between the subfascial branch of the deep cervical plexus and the SAN after reinnervation of the trapezius muscle, were examined following radical ND. The endurance, which was assessed as the number of repeated arm abductions without fatigue, started to increase at five months after the surgery in these patients [41]. In a different study, patients undergoing selective ND with and without level 2b dissection were compared in terms of shoulder function. Although better shoulder endurance performance was stated in the group without level 2b dissection, an intragroup comparison was not examined during the postoperative period [42]. To our knowledge, the current study is the first study comparing performance of scapular muscle endurance before and after the surgery in patients with HNC. Our results revealed a decrease in scapular muscle endurance. Both loss of scapulohumeral and scapulothoracic muscle strength and scapular endurance may explain the reduced functional shoulder outcomes after ND.
Active muscle control provides both stability and mobility of the shoulder to maintain normal function [14]. The coordinated movement of scapular and rotator cuff muscles supports normal scapulohumeral rhythm. Muscle weakness may cause shoulder disability by changing the scapulohumeral rhythm [38]. It was demonstrated that early physiotherapy interventions, including facilitation of peripheral nerve recovery and strengthening scapular muscles might enhance shoulder functions in patients with HNC [43]. Both hospital and home-based exercise programs comprising strengthening of the trapezius, sternocleidomastoid, rhomboid, supraspinatus, infraspinatus, subscapularis, deltoid, biceps and triceps muscles improved shoulder functions in HNC survivors [44]. In a study examining the effect of progressive resistance exercise training, the increase of upper extremity muscle strength and muscle endurance was correlated with the decrease in Shoulder Pain and Disability Index total score and pain subscale score. While muscle strength was evaluated by 1-repetition maximum test for the seated row and the chest press, muscle endurance was evaluated by submaximal seated row test in the study. Because increasing muscle strength and endurance may decrease shoulder dysfunction, it may support the relationship between these variables [40]. In the current study, there are moderate to strong correlations between postoperative shoulder function and changes in muscle endurance and muscle strength, except for the upper trapezius muscle. As CMSS contains items that investigated flexion, abduction and rotation of the shoulder, the relationship between shoulder functions and the serratus anterior and rotator cuff muscles, including the infraspinatus/teres minor, subscapularis and supraspinatus muscles, may be detected. Shoulder dynamic stability must be provided to maintain shoulder functions properly. The middle and lower trapezius muscles are among the main stabilizers. Although changes in these muscles’ strength may relate to CMSS, the upper trapezius muscle strength may not completely reflect shoulder functions.
The strengths of the current study include its prospective follow-up design and its focus on determining the muscle strength and scapular endurance changes after ND and its relationship with postoperative shoulder function. The majority of the studies in this population are emphasized on shoulder muscle or scapular muscle strength, especially trapezius muscle, rather than muscle endurance. In this study, we investigated many of the scapulohumeral and scapulothoracic muscles’ strength in addition to the trapezius muscle strength. To our knowledge, there are no published studies that have taken these issues into consideration, and this is the first study to investigate scapular muscle endurance in a population of patients with HNC. Furthermore, the methodology of previous studies does not include follow-up evaluations [37, 45]. Therefore, this study overcomes many of the important limitations of previous studies.
There are some limitations associated with the current study as all research faces. Firstly, although our post-hoc analysis based on scapular endurance and shoulder function values provided adequate power for the study, we think that sample size was the major limitation. Secondly, participants were not classified according to the features, such as dissection type or adjuvant therapy that may affect shoulder functions because the sample size was small. Thirdly, the gold standard isokinetic dynamometer was not used for evaluation of muscle strength due to its high cost. Fourthly, blind assessment and long-term follow-up were not performed. Observing clinical course of functional decline in the postoperative late period will be important for the determination of proper treatment. Lastly, we could not use more precise methods of measurement, such as electromyography, ultrasound imaging and isokinetic muscle strength evaluation as in other studies [18, 24, 45] which are less subjective measurements that can be used to assess more parameters regarding the muscle function. Despite these limitations, considering that the shoulder is a complex structure, it was important to assess both scapular muscles and rotator cuff muscles in the current study. In addition, using a handheld dynamometer, instead of manual muscle testing which was commonly used in the literature, may help determine minor differences in muscle strength.
Conclusion
The current study highlights decrease of both scapular and rotator cuff muscle strength, and scapular muscle endurance three months after ND. Declines in muscle strength and endurance may be correlated with postoperative deteriorated shoulder function in patients with HNC. Early postoperative management aimed to improve muscle strength and endurance may help to maintain shoulder functions in patients with HNC. Further studies investigating changes in muscle performance for relatively long periods (six months and one year) after surgery may further contribute to our understanding of shoulder function.
Footnotes
Acknowledgments
The authors would like to thank Dokuz Eylül University Department of Scientific Research Projects for the financial support (Project number: 2017.KB.SAG.053).
Conflict of interest
None to report.