
Abstract
BACKGROUND:
When a patient with a prior history of malignancy and radiotherapy develops progressive weakness as a presentation of plexus involvement, the differential diagnosis usually rests between radiation-induced plexopathy and invasion from recurrent tumor. The presence of myokymic discharges is helpful in differentiating radiation-induced from neoplastic plexopathy.
OBJECTIVE:
To present a case report of a patient with chordoma, a locally aggressive tumor, who was diagnosed with recurrent tumor accompanied by the occurrence of myokymia in needle electromyographic examination.
METHOD:
A 55-year-old male patient with a history of chordoma and radiotherapy presented to our outpatient clinic with complaints of foot drop, and impaired walking for two months. His latest magnetic resonance imaging (MRI) which was performed three months earlier did not show recurrence. Upon electromyographic evaluation, myokymia, the pathognomic electromyography abnormal wave for radiation plexopathy was detected supporting a diagnosis of radiation plexitis rather than recurrent neoplastic invasion. One month later he presented with more severe pain and was re-evaluated by an MRI, on which a mass was detected indicating relapse.
CONCLUSION:
With this case report, we would like to emphasize that the behaviour of the tumor should be considered and imaging should be repeated when tumors display aggressive or recurrent behaviour.
Introduction
The lumbosacral plexus is formed by a network of nerves including the anterior rami of the lumbar and sacral spinal cord. Lumbosacral plexopathy is an injury to the nerves in the lumbar and/or sacral plexus [1]. Involvement of the lumbosacral plexus can result from many causes ranging from tumors to trauma. While trauma is more common in the etiology of brachial plexopathies, neoplastic invasion of involving adjacent pelvic organ cancers is more commonly encountered in lumbosacral plexopathies. Lumbosacral plexopathy is an extremely serious complication of cancer and the clinical course might be associated with severe bilateral lower leg pain, reduced sensation, different degrees of weakness, paresis or paralysis, and sometimes also urinary or faecal incontinence [2]. Neoplasms are the most common cause of lumbar plexopathy. In a patient with a remote or recent cancer and a history of radiation therapy, lumbosacral plexopathy can be due to either neoplastic invasion or radiation-induced injury. Plexus involvement in cancers is seen in about 1% of the cancers. Neoplasm as the cause for lumbosacral plexopathy should be higher on the differential, especially in patients with a history of cancer [3]. Radiation-induced lumbosacral plexopathy is a rare but so severe and debilitating complication with a significant impact on quality of life; its frequency ranges from 0.3 to 1.3% [4]. Although its occurrence is rare, it increases with increased long-term cancer survival. For the clinician, the important clinical dilemma encountered is distinguishing radiation-induced plexopathy from the recurrent tumor [3]. Also, neoplastic lumbosacral plexopathy should be differentiated from radiation-induced lumbosacral plexopathy because the management of neoplastic plexopathy usually needs radiotherapy. This may increase symptoms in radiation-induced lumbosacral plexopathy if radiation-induced lumbosacral plexopathy is misdiagnosed as neoplastic lumbosacral plexopathy. These two conditions can coexist in the same patient, further complicating the situation. Therefore, it is necessary to recognize these complications for accurate diagnosis and treatment [3].
Myokymic discharges are one of the abnormal spontaneous activity types seen in electromyographic examinations. Myokymia stems from areas of axonal demyelination. The main clinical feature of myokymia is undulating, continuous vermicular or worm-like involuntary rippling movements of muscle [5]. In needle electromyographic examination, they are groups of recurring spontaneously firing motor unit action potentials (MUAPs) that fire in a repetitive burst pattern [6]. Between bursts there is electrical silence [7]. They are easily identified by an experienced electromyographer with their typical visual and auditory pattern. Myokymic discharges sound like “marching soldiers.” They are pathognomonic for radiation-induced plexopathy and it is unusual to find myokymia in neoplastic plexopathy [1, 6, 8, 9]. Detection of characteristic myokymic discharges during spontaneous activity examination on electromyography helps to differentiate radiation plexopathy from plexopathy due to infiltration of the plexus by malignancy [8]. Herein, we present a case of tumoral recurrence in a patient despite the occurrence of myokymia in needle electromyographic evaluation.
Case presentation
A 55-year-old male patient presented to our outpatient clinic with complaints of increased pain in his legs, foot drop, and impaired walking for 2 months. He also had paresthesia, tingling and pins and needles sensation in his legs for one year that recently worsened. The patient’s complains of leg pain had started six years earlier with the diagnosis of chordoma. He had felt pain in his waist that was spreading to the perianal region and urinary incontinence symptoms emerged. At that time, after evaluation by a neurosurgeon, the sacral tumour was detected on lumbosacral magnetic resonance imaging (MRI) and he was referred to an orthopaedic surgeon for surgery. He had a history of thirty sessions of radiotherapy following surgery for sacral chordoma five years earlier. However, local recurrence of sacral chordoma occurred four times and from that time the patient has undergone five surgical operations for the recurrences. He was performing intermittent catheterization six times a day for seven years. Before admission to our outpatient clinic, the patient had visited an orthopaedic surgeon due to complaints of foot drop, leg pain and difficulty in walking and he had been undergone a recent MRI exam three months earlier which revealed no recurrence of sacral chordoma. Also, his latest PET scan, which was also performed three months earlier, was negative for any cancer recurrence. The patient was referred to our department for rehabilitation.
He had a past medical history of cardiac arrhythmia, gastric cancer surgery and the following chemotherapy eighteen years earlier. In addition, three years earlier, he had undergone total gastrocolectomy and ileostomy surgery due to gastric cancer recurrence. The medications that he was taking were digoxin and metoprolol for heart failure and arrhythmia, pregabalin, fentanyl and tramadol for pain management and imatinib for chordoma.
The patient reported his leg pain severity as 40 on a 100 mm visual analogue scale (VAS) but he declared that his pain intensity used to be 60 before starting pain medicines. On physical examination hip flexion muscle strength was detected as grade 4 on the right side, grade 3 on the left side, quadriceps muscle strength was grade 4 bilaterally, ankle dorsiflexion muscle strength was grade 4 on the right side and grade 0 on left side and ankle plantar flexor muscle strength was grade 5 bilaterally. Upper extremity muscle strength was within normal limits. Bilateral patellar reflexes were found to be hypoactive. The plantar response has been found to be bilateral unresponsive. Sensory testing revealed hypoesthesia over the skin of the lateral feet.
Plexopathy, radiculopathy and polyneuropathy were considered as differential diagnoses and electromyography was performed. His electrophysiologic studies showed decreased conduction velocities in compound motor action potentials (CMAP) of the left tibial and right peroneal nerves. There were no responses in CMAP of the left peroneal nerve. In sensory nerve action potentials, there were no responses bilaterally in sural nerves. These changes indicated that the lesion is distal to the dorsal root ganglion and helped exclude the presence of radiculopathies. Other conduction studies did not show any abnormalities, decreasing the likelihood of polyneuropathy. In needle EMG, there were widespread spontaneous activities in the form of positive sharp waves and fibrillation potentials on the left lower extremity. The intensity of these changes was less on the right side, but still present in the adductor longus and gastrocnemius muscles. EMG examination showed myokymic discharges in the right gluteus medius muscle (Fig. 1;
Myokymia waves detected in the gluteus medius muscle.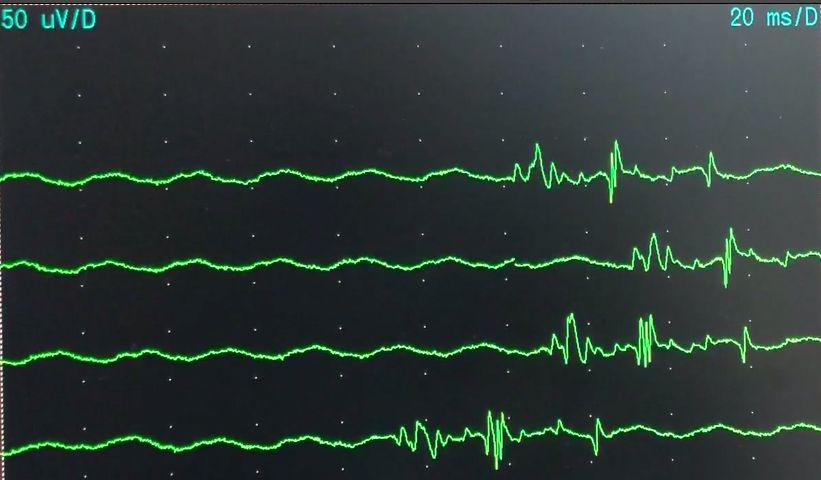
Motor nerve studies
R: right, L: left, APB: Abductor pollicis brevis, ADM: Abductor digiti minimi.
Sensory nerve studies
R: right, L: left.
Needle EMG findings
PSW: Positive sharp wave; Fib: Fibrillation; CRD: Complex repetitive discharges.
Clinical distinction of radiation plexopathy from neoplastic plexopathy and comparison of patient’s clinical findings with neoplastic and radiation plexopathy characteristics
EMG, electromyography; BP, Brachial plexopathy; LSP, lumbosacral plexopathy; MRI, magnetic resonance imaging; PET, positron emission tomography.
A low-density mass is seen in the T1-weighted axial image on the right side of the spinous process at the L5 level (marked by a star).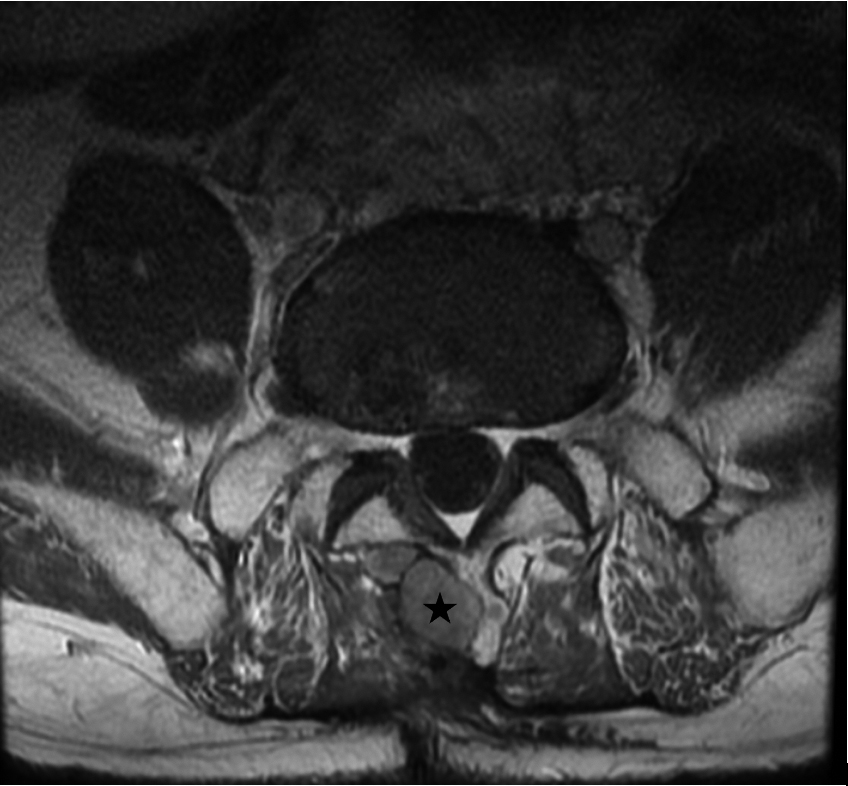
The presence of conduction abnormalities combined with the widespread abnormalities in spontaneous discharges and voluntary MUAPs were evaluated as bilateral subacute involvement of the lumbosacral plexus. He was prescribed ankle-foot orthosis and started a rehabilitation programme including electrical stimulation of tibialis anterior and quadriceps muscles, strengthening upper and lower extremities and improving walking balance. The clinical and EMG findings supported the diagnosis of radiation plexopathy (Table 4) [10]. However, one month later he presented with more severe pain and was re-evaluated by an MRI. A mass indicating relapse was detected on the MRI (Fig. 2).
Lumbosacral plexus is found close to abdominal and pelvic structures. Various pathologies and injuries associated with these anatomical structures may cause lumbosacral plexopathy [1]. These include direct trauma (sacral fracture, posterior hip dislocation etc.), metabolic, inflammatory and autoimmune causes (diabetic amyotrophy, amyloidosis, sarcoidosis), infections and local abscess (vertebral osteomyelitis, psoas abscess, vertebral osteomyelitis, herpes zoster), pregnancy-related (idiopathic in the third trimester and after delivery due to birth trauma), damage to the vasculature which innervates the plexus (femoral vessel catheterization, ischemia from direct compression due to arterial pseudoaneurysms, aortic dissection, retroperitoneal hematoma, etc.), postoperative plexopathy (scar tissue formation and hematomas after gynaecological and other pelvic surgeries), radiotherapy of the abdominal and pelvic malignancies and neoplastic [1]. The lumbosacral plexus is generally occupied by primary pelvic neoplasms but occasionally is invaded by metastases to regional lymph nodes or bony structures. Colorectal adenocarcinomas, uterine or cervical malignancies, lymphomas, and retroperitoneal sarcomas are the most common tumors reported to affect the lumbosacral plexus [11, 12]. Lumbosacral plexopathies may develop from direct tumoral invasion or direct extension from neighbouring tumors (tumors originating from the bladder, colon, ovaries, and cervix), distant metastasis (the lung, the breast, and lymphomas are the most common), compression of lumbar plexus from enlarged metastatic lymph nodes and epineural spread or intraneural lymphomatosis. Neoplasm as the cause for lumbosacral plexopathy should be considered for differential diagnosis, especially in patients with a history of cancer [12].
Chordoma is a rare bone tumor that arises from undifferentiated notochordal remnants in the axial skeleton. It generally exhibits slow-growing but locally aggressive behaviour [13]. Chordomas constitute 1–4% of all bone tumors and are predominant in men in their 50th to 60th. The clinical manifestations of chordoma vary depending on the location and invasion of the tumor and typically include deeply localized pain, neurological deficits including lumbosacral plexopathy, radiculopathy and bladder-bowel dysfunction [14, 15, 16]. Surgery is the mainstay of the treatment of chordoma. Radiotherapy is often combined with surgery to improve local control [14]. Systemic therapy including targeted immunotherapy with agents such as imatinib in combination with chemotherapy is useful but is often used in case of tumor recurrence or metastatic disease. The local recurrence rate of chordoma after treatment has been reported be as high as 43–90% [14].
If a patient with a previous history of malignancy and having received radiation therapy presents with a slowly progressive plexus lesion, the differential diagnosis often lies between radiation-induced plexopathy and plexus invasion and tumor recurrence. Some clinical and electrophysiological findings can help to differentiate between the two. A detailed history and a thorough physical exam and diagnostic studies including MRI, positron emission tomography (PET) and electromyographic studies complement each other in differential diagnosis [3]. In case of direct neoplastic invasion, pain occurs earlier and more prominently. Radiation plexopathy often presents with dysesthesias and numbness, and often there is lymphedema. Unlike neoplastic lumbosacral plexopathy, lumbosacral radiation plexopathy usually presents with less pain and has a slowly progressive course [3]. Supporting the clinical course of radiation-induced plexopathy, our patient showed a slowly progressive course of weakness and presented with mild pain and neuropathic complaints. Periods of quiescence between periods of exacerbation can be seen in radiation-induced plexopathy [3]. But our patient did show neither ameliorations and exacerbations nor lymphedema. Depending on the radiation port, different parts of the plexus may be involved in radiation plexopathy. In neoplastic lesions the lower lumbosacral plexus is usually involved [6, 17]. Also, bilateral involvement of the plexus is more common in radiation plexopathy [3]. Involvement of the lumbosacral plexus was bilateral in our patient. Considering (1) the appearance of myokymic discharges, which has special diagnostic significance for radiation-induced plexopathy in the gluteus medius muscle, which is innervated by the superior gluteal nerve formed from posterior divisions of L4, L5 and S1 nerve roots of the lumbosacral plexus and (2) accompanying active denervation or reinnervation in muscles supplied by the same root level but by different nerves including sciatic, peroneal, tibial femoral and obturator nerves on needle electromyography, and (3) the patient’s remarkable history, we were able to make the diagnosis of radiation-induced plexopathy. Although the presence of characteristic myokymic discharges on needle EMG and absence of tumoral recurrence at the time of evaluation pointed out radiation-induced plexopathy but later on, patient’s pain and weakness got worse and an MRI revealed tumoral recurrence. As happened in our patient, these two conditions including neoplastic and radiation induced plexopathy can coexist in the same patient, further complicating the differential diagnosis.
The diagnosis of metastatic plexopathy is usually supported by imaging modalities. MRI is the best sensitive imaging technique to provide anatomic details and is usually a preferred imaging modality [6]. Enhancement of nerve roots and T2-weighted hyperintensity usually support tumors. Unfortunately, it remains difficult to distinguish from tumor recurrence. Generally, radiation plexopathy does not cause nerve enhancement, although an increase in T2 signal may be present [11]. Diagnosis can be difficult if the scan initially does not show a mass lesion, but repeating the scan, usually within 4 to 6 weeks, will reveal a tumor that is not apparent on initial scans [11]. PET scanning with 2-[fluorine-18]-fluoro-2-deoxy-D-glucose (FDG) may aid in diagnosing recurrent tumor. Although PET/CT scanning may be helpful in distinguishing tumor recurrence from radiation plexitis in cancer patients, it discloses only limited resolution of the brachial or lumbosacral plexus [17]. Also, F-FDG activity can be variable depending on grade. A broad spectrum of metabolic activity, from minimal intake to intense activity, can be seen in the ranges seen with high-grade malignancy. In cases of minimal uptake, F-FDG PET/CT would be less helpful in detecting metastatic disease or potentially assessing treatment response [18].
The presence of characteristic myokymic discharges on needle EMG is an important diagnostic finding in favor of a diagnosis of radiation plexitis rather than recurrent neoplastic invasion [19]. While this classic scenario is generally valid, the case we report here shows that the type of tumor that causes plexopathy is also important for the evaluation, diagnosis and treatment. The strength of this report is increasing the awareness of physicians that tumor recurrence should still be considered in patients with chordoma which is a frequent relapsing tumor, despite detecting myokymia, a characteristic abnormal wave for radiation induced plexopathy, on electromyographic examination. Just before his admission to our outpatient clinic and electromyography laboratory, the patient had undergone a PET-CT and pelvic MRI which was not compatible with relapse, and this caused a challenge in the diagnosis of the patient. Diagnosis can be difficult when a mass lesion is not found on the MRI. To the best of our knowledge, MRI should be repeated in case of frequent relapsing tumors that were not detected on initial imaging. The present case had dual diagnosis including both radiation-induced and neoplastic tumor invasion plexopathy. Lumbosacral plexopathy due to tumoral recurrence usually is treated with radiotherapy. Because this patient was also diagnosed with radiation-induced plexopathy, his medical oncology doctor was informed about the diagnosis and he did not again receive radiotherapy. Electromyography in radiation-induced plexopathy typically shows myokymic discharges, seen in up to 60% of the patients. However, we suggest that this might not rule out tumor recurrence[3].
Conclusion
In case of a patient with a history of neoplasm and radiation therapy and symptoms of lumbosacral plexopathy, despite the presence of myokymia, the pathognomic electromyography abnormal wave for radiation plexopathy, behaviour of the tumor should be considered and imaging should be repeated.
Funding
The authors received no financial support for the research and/or authorship of this article.
Ethics approval
Not applicable.
Informed consent
Both written and oral informed consent was obtained from the patient prior to publication.
Author contributions
Concept: EG, OA, OKC, IY, HG; Design: EG, OA, OKC, IY, HG; Supervision: EG, OKC, IY, HG; Materials: EG, OA, OKC, IY, HG; Data Collection and/or Processing: EG, OA, OKC; Analysis and/or Interpretation: EG, OA, OKC, IY, HG; Literature Review: EG, OA, OKC; Writing: EG, OA, OKC; Critical Review: EG, OA, OKC, IY, HG.
Footnotes
Acknowledgments
None to report.
Conflict of interest
The authors declare no conflicts of interest with respect to the authorship and/or publication of this article.