
Abstract
BACKGROUND:
Pole vaulting involves trunk flexion, extension, and rotation, which may place the lumbar spine under stress. Repeated pole vaulting may cause lumbar disc degeneration (DD) and lumbar spondylolysis (LS); however, this phenomenon is yet to be established.
OBJECTIVE:
This study aimed to determine the difference in the maximum joint angles of the shoulder, hip, and trunk during pole vaulting between male pole vaulters with and without lumbar DD or LS.
METHODS:
This retrospective study included 17 male pole vaulters. Four high-speed cameras were used to record the pole vaulters at 240 Hz. Radiography and magnetic resonance imaging were used to examine the lumbar spine in all athletes. Differences in the data between two sets of groups were analyzed using the unpaired t-test or the Mann-Whitney U test.
RESULTS:
There was a significant difference in the maximum joint angle of hip flexion between pole vaulters with and without lumbar DD (
CONCLUSION:
Pole vaulters with lumbar DD may use lumbar flexion instead of hip flexion during the rock-back movement. Moreover, LS may occur due to repeated failed vaulting. Therefore, trunk stability and functional movements should be prioritized to prevent organic changes in the lower back.
Introduction
Pole vaulting is a track and field event. Pole vaulters are more likely to sustain injuries among jumpers [1]. Pole vaulting involves trunk flexion, extension, and rotation movements, which may place high stress on the lower back. In particular, factors causing low back pain (LBP) have been studied in pole vaulters. Rebella [2] reported that the lower back was the most common location for injury among collegiate pole vaulters and 83% of low back injuries and 100% of cases of lumbar spondylolysis (LS) occurred during the plant/take-off phase of the vault. Further, this study suggested that LS was caused during the plant/take-off phase and that the spine is forcefully hyperextended as the athlete drives forward off the ground. Moreover, the prevalence of LS and lumbar disc degeneration (DD) in male pole vaulters were reported to be 28.6% and 38.1%, respectively [3].
Two previous studies have examined the relationship between pole vaulting motions and injuries. Gainor et al. [4] reported an association between pole vaulting motions and LS in three pole vaulters and indicated that the maximum angular acceleration of the hyperextended spine occurred during take-off. In addition, Edouard et al. [5] reported that some biomechanical parameters such as the lower height of the gripping hand from the ground at take-off, higher approach speed, contact time on the floor, last stride adjustment, and stride length validity in the approach phase were associated with higher proportion of all injuries. However, Gainor et al. [4] only examined pole vaulters with LS. Therefore, it is unclear whether these findings are related to both lumbar DD and LS. Moreover, to our knowledge, the relationship of lumbar DD and LS with repetitive pole vaulting has not been studied previously.
Therefore, this study aimed to determine the difference in the maximum joint angles of the shoulder, hip, and trunk during pole vaulting between male pole vaulters with and without lumbar DD or LS. We hypothesized that pole vaulters with lumbar DD or LS would have smaller shoulder or hip joint angles during pole vaulting. In addition, we theorized that if the joint angles are small in the joints adjacent to the lumbar region (such as the shoulder and hip joints) during pole vaulting, the joint angles of the trunk during flexion or extension will be large, resulting in a difference in the flexion and extension strategies of the body.
Methods
Participants
This retrospective study included 17 male pole vaulters (mean
Questionnaire
A self-reported questionnaire was used to obtain information regarding participants’ demographics, such as age, height, body weight, personal best record, and history of competing in pole vaulting. The take-off leg (defined as the leg used during vaulting) was also examined using the same questionnaire. The opposite leg was defined as the lead leg.
Range of motion
The active and/or passive range of motion (ROM) and muscle flexibility of participants lying on a bed (passive shoulder flexion, active/passive straight leg raise [SLR], and passive hip flexion and extension) in the sagittal plane were measured as described previously [6, 7]. The participants wore compression garments at the time of measurements, and a reference point was attached to these garments by an athletic trainer. All measurements were recorded using a camera (EX-F1, CASIO, Tokyo, Japan) placed 3 m to the side of the bed and were analyzed using an image analysis software (NIH ImageJ ver.14.4; National Institutes of Health). The ROM was measured as described below.
Passive shoulder flexion: The angle formed between the line connecting the two landmarks on the humerus and a line parallel to the trunk. Active/passive SLR: The angle between the line connecting the greater trochanter and the lateral malleolus and a line parallel to the trunk. Active/passive hip flexion and extension: The angle between a line connecting the greater trochanter and the lateral epicondyle of the femur and a line parallel to the trunk.
Pole vault model, event definition, and the definition of the global coordinate system. TD, touchdown; TO, take-off; MPB, maximum pole bending; PS, pole straight; ⟀, rockback movement.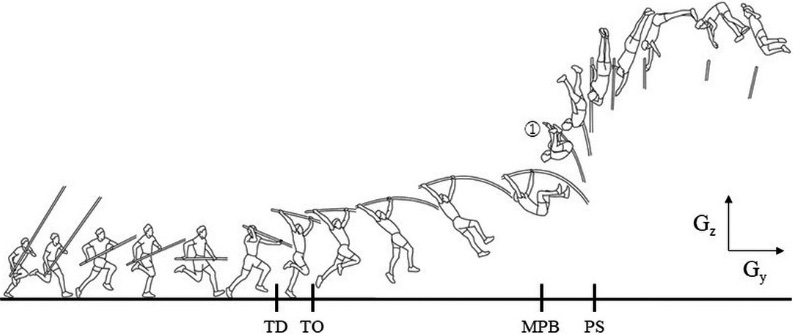
The procedure described in a previous study [3] was adapted to evaluate LS and DD in this study. Radiography and magnetic resonance imaging (MRI) were used to analyze the lumbar spine of each athlete. We obtained a radiograph of the lumbar spine from the anterior-posterior, lateral, and oblique planes at 45
Experimental setup and data analyses
The video for motion analysis was recorded from four directions with the planting box at the center, using four high-speed cameras (GC-LJ20B, JVC, Kanagawa, Japan) recording at a frequency of 240 Hz. All the videos were synchronized by switching on the light-emitting diodes during the experimental trials. The calibration area was set based on the left edge at 0 m in the direction of the run-up on the runway with a depth of 5 m on the runway side and 2.5 m on the mat side, a width of 1.25 m on the left side and 2.5 m on the right side of the runway, and a height of 5 m. Calibration poles, 5 m in height (0.5 m between marks), were set up at 10 points in the range and projected on video. For the experimental trials, the participants vaulted over bungee bars that were set at a height that was 90% of the athlete’s personal best record, until they achieved these three times. The three trials were included in the analysis. The pole vaulter selected the poles and the number of steps for the aforementioned trials.
The video was analyzed from the moment of touchdown of the last step of the run-up to the moment of pole straightening (Fig. 1) [10]. Digitization of body marks was performed manually at the frequency of 240 Hz using a motion analysis system (Frame-DIAS V, DKH Inc., Tokyo, Japan) for the knee and hip joints in both lower extremities, the shoulder and 12th rib in both upper extremities, and the elbow on the side of the lead leg. The global coordination system was constructed using
Proportions (%) of lumbar spondylolysis
Proportions (%) of lumbar spondylolysis
This result includes 1 athlete with both lumbar spondylolysis and lumbar disc degeneration.
Definition of each segment moving coordinate system.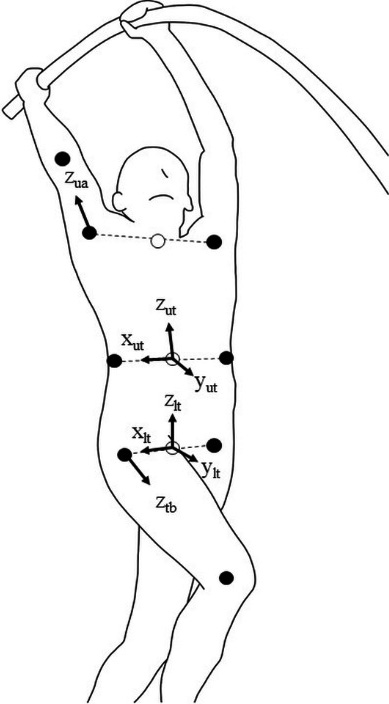
(1) Shoulder joint angle (lead leg side)
For the upper trunk segment moving coordinate system,
(2) Hip joint angle (both legs)
For the moving coordinate system of the lower torso segment, the unit vector from the left to the right great trochanter was defined as
(3) Trunk angle
Projection of the unit vector
All data analyses were performed using SPSS version 23 (IBM Corp., Armonk, NY, USA). A
Proportions (%) of lumbar disk degeneration
Proportions (%) of lumbar disk degeneration
DDPs, participants who had disk degeneration at one or more disk levels. This result includes 1 athlete with both lumbar spondylolysis and lumbar disc degeneration.
Comparison of the population statistics and each ROM between vaulters with and without lumbar spondylolysis
LS, Lumbar spondylolysis; SD, Standard deviation; CI, confidence interval; SLR, straight leg raise; The Mann-Whitney U test was used to analysis.
Comparison of each maximum joint angle between vaulters with and without lumbar spondylolysis
SD, standard deviation; CI, confidence interval; LS, lumbar spondylolysis; Positive values indicate flexion and negative values indicate extension from the anatomical position; The Mann-Whitney U test was used to analysis.
Comparison of the population statistics and each ROM between vaulters with and without lumbar disc degeneration
DD, disc degeneration; SD, Standard deviation; CI, confidence interval; SLR, straight leg raise; The unpaired
Comparison of each maximum joint angle between vaulters with and without lumbar disc degeneration
SD, standard deviation; CI, confidence interval; DD, disk degeneration;
Prevalence of LS and lumbar DD
The assessment of participants for lumbar DD and LS showed that six and five pole vaulters had lumbar DD and LS, respectively (Tables 1 and 2). In addition, both lumbar DD and LS were observed in one pole vaulter, and this vaulter was included in both groups with LS and with lumbar DD.
Comparison of ROM and maximum joint angles during pole vaulting
Lumbar spondylolysis
The Mann-Whitney U test was used for comparison between the groups because the normality of the data was not confirmed by the Shapiro-Wilk test and there were six pole vaulters with LS. There were no significant differences in the population statistics and ROM between the groups (Table 3). There were no significant differences in maximum joint angles between the groups (Table 4).
Lumbar disc degeneration
The unpaired
Discussion
This retrospective study is the first to determine the difference in maximum joint angles of the shoulder, hip, and trunk during pole vaulting between male pole vaulters with and without lumbar DD or LS. We hypothesized that lumbar DD and LS were associated with small hip and shoulder joint angles that affected trunk motion during pole vaulting. The results demonstrate that the maximum hip flexion angle on the take-off leg of pole vaulters with lumbar DD was significantly smaller than that on the take-off leg of pole vaulters without lumbar DD.
Hangai et al. [13] evaluated the proportion of participants with lumbar DD among college students and found it to be highest among baseball players (59.6%) and swimmers (57.5%). They explained that sport-specific movements of baseball players and swimmers, including frequent rotation of the trunk, were considered risk factors for lumbar DD. Another study reported an increase in the prevalence of lumbar DD, from 16.7% to 83.3%, in a two-year follow-up study involving weightlifters [14]. Yanagisawa et al. [15] reported that high-load deadlift exercise imposes mechanical stress on all lumbar intervertebral discs, particularly the L5/S1 disc. These studies show that motions, such as deadlifting, wherein forces are exerted in a hip flexion posture or a hip flexion posture is forced, and frequent trunk rotation may be related to lumbar DD. Our results showed a significant difference in maximum hip flexion angle on the take-off leg between vaulters with lumbar DD and those without lumbar DD. Trunk flexion angle also showed a high effect size, although there was no significant difference in trunk flexion angle between vaulters with lumbar DD and those without lumbar DD. Considering previous studies and this study, we inferred that pole vaulters with lumbar DD used lumbar flexion instead of hip flexion during the rock-back movement (Fig. 1-⟀). The pole vaulter’s take-off leg is flexed after the hip joint has reached maximum extension. The iliopsoas muscle, which acts in hip flexion, is attached to the femur and lumbar spine. Therefore, we considered that the lumbar spine (trunk) needs to be stable to flex the hip joint rapidly at a sufficient angle. However, if an athlete who does not have trunk stability is instructed to flex the hip joint rapidly at a sufficient angle, there is a possibility that the athlete will flex the trunk instead as a compensatory movement. Thus, we recommend that coaches ensure that the athlete is not achieving a rock-back position with compensatory movements of the lumbar spine and have the athlete undergo training to gain trunk stability. Previous studies on the general population reported that exercises targeting the deep muscles are effective in alleviating chronic LBP [16], suggesting that instructions on trunk stability are necessary. Therefore, trunk stability and functional movements should be achieved to prevent LBP and organic changes in the lower back. In addition, vaulters with lumbar DD may not be able to flex their hip joints sufficiently due to the effects of lumbar DD. Therefore, we believe that athletes need to know if they have lumbar DD to improve their performance and prevent LBP. However, hip flexion could decrease after the onset of lumbar DD to prevent pain or anxiety from abnormal lumbar symptoms. Therefore, further research is needed to clarify these cause-and-effect relationships.
Spondylolysis is a stress fracture that is frequently reported in adolescent athletes. Movements requiring lumbar hyperextension and/or rotation are considered risk factors for the development of this lesion. The prevalence of LS has been previously reported in American footballers [17], beach volleyball athletes [18], and Spanish elite athletes [19], in whom the lower spinal levels (L4 and L5) were more frequently affected. In our study, we analyzed trials wherein athletes could jump over the bungee bar (which was set at 90% of the height of their personal best record). However, there were no significant differences in the maximum joint angles between pole vaulters with and without LS. A possible explanation for this could be the exclusion of trial motions that did not result in successful vaulting above the aforementioned height from the analysis. The study by Rebella [2] supports this explanation as it reported that repeated failed vaulting, wherein the athlete drives forward off the ground in the plank/take-off phase, may result in the development of LS. Therefore, it is likely that reducing failed vaulting is necessary to prevent LS; however, additional prospective studies are needed to clarify this.
Limitations
This study has some limitations. First, we could not demonstrate a cause-and-effect relationship between lumbar DD and the maximum joint angle in hip flexion during pole vaulting in this retrospective study. Second, this study had a limited sample size of 17 participants. However, the effect size was calculated considering the effect of the small sample size on the results. Third, because there were few healthy participants (those with neither LS nor lumbar DD), we could not compare them with a complete control group. In addition, the fact that athlete with both LS and lumbar DD was included in the analysis may influence the results. Finally, to avoid the effects of male and female sexual characteristics on the performance of pole vaulting and consequently the results, only male pole vaulters were recruited for assessment in this study. Therefore, the study findings may not be entirely applicable to female pole vaulters. Despite these limitations, it is worth noting that, to our knowledge, this is the first study to examine the relationship between lumbar DD or LS and maximum joint angles during pole vaulting.
Conclusion
There was a significant difference in the maximum joint angle of hip flexion between vaulters with lumbar DD and those without lumbar DD. This suggests that lumbar DD in pole vaulters was caused by the use of lumbar flexion instead of hip flexion during the rock-back movement or the change in movement due to pain associated with the occurrence of lumbar DD. In addition, there were no differences in maximum joint angles between those with LS and those without LS. Thus, LS may occur due to repeated failed vaulting. Nevertheless, future prospective studies are required to examine movement-related factors for the occurrence of lumbar DD and LS and the detailed behavior of the lumbar spine during pole vaulting.
Funding
This study was funded by a grant from the Chukyo University Research Institute in 2018 and 2019.
Informed consent
All participants provided written informed consent.
Author contributions
SE: Conception and Design, Acquisition of Data, Analysis and Interpretation of Data, Drafting the Article, Critically Revising the Article, Final Approval of the Article; RK: Conception and Design, Critically Revising the Article, Final Approval of the Article; HT: Conception and Design, Acquisition of Data, Analysis and Interpretation of Data, Critically Revising the Article, Final Approval of the Article; KN: Conception and Design, Acquisition of Data, Analysis and Interpretation of Data, Critically Revising the Article, Final Approval of the Article; HM: Conception and Design, Acquisition of Data, Analysis and Interpretation of Data, Critically Revising the Article, Final Approval of the Article.
Footnotes
Acknowledgments
The authors appreciate the education and assistance provided by the Graduate School of Chukyo University and the Yoshida Orthopedic Hospital.
Conflict of interest
The authors declare that they have no conflict of interest.