
Abstract
BACKGROUND:
Adhesive capsulitis (AC) is a common musculoskeletal disease characterized with shoulder pain, limitation of range of motion (ROM) and disability. Although physical therapy is used in the treatment of AC, studies on its effectiveness are continuing.
OBJECTIVE:
This study aimed to assess the effectiveness of ultrasound (US) and high-intensity laser therapy (HILT) in the treatment of AC.
METHODS:
Sixty patients were randomized into two groups. Group I received US (15 sessions) and Group II received HILT (9 sessions) for 3 weeks. In addition, all patients received physical therapy program (hot pack, TENS and exercises). Assessments were made using VAS-pain, Shoulder Pain and Disability Index (SPADI), range of motion (ROM) at baseline and in post-treatment 3
RESULTS:
There was no statistically significant difference between the groups in terms of all pre-treatment values. In intragroup assessment, statistically significant difference was identified in all the values of Groups 1 and 2 in all assessment periods compared with the pre-treatment values (
CONCLUSION:
According to results, US therapy and HILT were effective on the improvement of pain, ROM and functional conditions of patients in the treatment of AC.
Keywords
Introduction
Adhesive capsulitis (AC) (also termed frozen shoulder) is a common condition characterized by spontaneous onset of pain, progressive restriction of movement of shoulder and disability that restricts activities of daily living, work and leisure [1]. The prevalence of AC is between 2–5% in general population and higher between the ages of 40 and 60 and among women [2].
The etiopathogenesis of AC has not clearly been explained. AC is divided into two as primary AC (idiopathic) which develops without any specific reason and secondary AC which develops due to predisposing factors (systemic, intrinsic and extrinsic) [3]. Synovitis, fibrosis and contracture of shoulder joint capsule are the characteristic findings of AC [4].
The aim in the treatment of AC is to relieve pain and increase joint range of motion (ROM) and functioning [5]. The treatment of AC remains controversial because the level of evidence for various treatment methods is limited [6]. Randomized, controlled and prospective studies are difficult to design and perform because of controversies in definition, classification, diagnosis, and stages of AC [6]. Many different treatment methods such as medical treatment, physical therapy, exercises, intraarticular steroid injections, suprascapular nerve block, manipulation under anesthesia, and surgical interventions are used in the treatment of AC [7]. Although many different treatment methods are used in treatment of AC there is no consensus on the standard method. It has been shown that physical therapy practices have positive effects on AC in the short and long term [8].
Among physical therapy practices, electrotherapy modalities (e.g. Transcutaneous Electrical Nerve Stimulation (TENS), ultrasound (US), low-density laser therapy, high-intensity laser therapy (HILT), shortwave diathermy, diadinamic and galvanic current), hot pack and exercises are used alone or in combination in the treatment of AC [9].
Electrotherapy modalities, which aim to reduce pain and improve function through an energy increase (electrical, sound, light, thermal) in the body, are often delivered as components of a physical therapy intervention [10]. Among electrotherapy modalities, US therapy and HILT are used to increase energy in deeper tissue areas in body [10]. Therefore, US has frequently been used in physical therapy practices for a long time, and the interest in HILT has recently been increasing [11]. It was reported that deep heating agents used in physical therapy practices were effective in relieving pain and improving ROM and functioning of patients with AC [12].
US provides energy for deep tissue areas through ultrasonic waves by using a crystal sound head [13]. Therapeutic effects of US are classified as thermal and non-thermal. In thermal effects of US, ultrasonic energy reaching the deep tissue sites elevates tissue temperature by increasing molecular mobility. Elevation in the tissue temperature affects the tissue in different ways such as changing nerve conduction velocity, increasing local blood flow, pain threshold and collagen extensibility and reducing muscle spasm. Non-thermal or mechanic effects of US are the result of cavitation and micro streaming that can change cell membrane permeability, thereby facilitating the recovery of soft tissue [14, 15].
Logic behind the use of US in AC is that US can affect pain of the patients and particularly collagen viscosity of the shoulder joint capsule thanks to its thermal and non-thermal effects [10]. In a systematic review assessing the effectiveness of physical therapy practices in AC, US is recommended alone or in combination with conventional physical therapy methods for pain relief and improvement of ROM and functional conditions of patients [16].
HILT is a non-invasive physical therapy method which delivers energy into deep tissues via a device providing laser emission and the incidence rate of side effects is low in HILT [17]. HILT penetrates into joints and muscles in depth and can heal them with its analgesic, anti-inflammatory and anti-edematous effects on these tissues [18]. According to studies, HILT contributes to regeneration of tissues, new cartilage matrix synthesis and recovery processes of tendon and ligament lesions and inhibits the development of fibrosis [19, 20]. Because of these effects, use of HILT in the treatment of AC may be effective in relieving patients’ pain and improving their ROM and functioning [18]. In the randomized controlled study by Atan et al. on the effectiveness of HILT on AC, statistically more significant improvements were observed in pain, ROM and functional conditions of the group receiving HILT compared with the other groups [21].
This study aimed to investigate the effectiveness and superiority of US therapy and HILT, which are among deep heating agents and still being studied and recommended in the treatment of AC.
Materials and methods
Study design
The study was designed as a prospective, single-blind and randomized controlled trial. All procedures performed in studies involving human participants were in compliance with the ethical standards of the Institutional Research Ethics Committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The study protocol was approved by the Clinical Research Ethics Committee of Abant Izzet Baysal (approval number 2015/98).
Participants
A total of 60 patients who were admitted to physical therapy and rehabilitation outpatient clinic with pain and movement restriction in their shoulder and who signed the patient information consent form were included in the study. The patients who were clinically diagnosed with primary AC, those who were between the ages of 18 and 70, those who had had pain and movement restriction in his or her shoulder for at least 3 months, those who had restriction of passive external rotation in the involved shoulder restricted with less than 50% of the contralateral shoulder, and those who had normal radiography findings were included in the study. Patients in whom both shoulders were involved, patients who had other shoulder pathologies (e.g. glenohumeral osteoarthritis, calcific tendinitis, rotator cuff tear), patients who had cervical radiculopathy, brachial plexus lesion, neuromuscular disorders, inflammatory rheumatic disorders, malignancy, or acute trauma, patients who had fracture affecting the involved shoulder joint, patients who underwent a surgical intervention, patients who underwent intraarticular injection for the involved shoulder within the last 6 months, patients who received physical therapy for the glenohumeral joint within the last 1 year, and patients who had photoallergy were not included in the study.
Randomization and blinding
A total of 60 patients who met the inclusion criteria of the study were divided into 2 groups (30 patients in each group) with simple randomization method by using a table of random numbers created on computer. Researchers who made the assessment measurements were unaware of which patient was in which group. Statistical analysis of the results was performed by a biostatistician who had no information about therapies the patient groups received.
Interventions
All patients included in the study received a total of 15 sessions of physical therapy program five times a week for 3 weeks. In the first treatment intervention for all patients, HP and TENS were used together. All patients received hot pack at 60
Group 1
Group 2
US therapy
Patients in group 1 received US with BTL 4710 ultrasound device (BTL Industries Ltd., Hertfordshire, UK). US was administered at the frequency of 3 MHz, intensity of 1.5 w/cm
HILT
Patients in group 2 received HILT with BTL 6000 high-intensity laser device (BTL Industries Ltd., Hertfordshire, UK), which provided emission of neody-mium-doped yttrium aluminum garnet (Nd: YAG) laser with a wavelength of 1064 nm and 12 W maximum power output. The therapy consisted of 2 stages in each session. The first stage was performed in analgesic mode for analgesic effect at the frequency of 25 Hz, in the wavelength of 1064 nm, power of 8 watt, dose of 12 j/cm
During the study, patients were asked not to use any oral or topical analgesic drug for pain, to use a drug from simple analgesic group (paracetamol) if they had to and to inform the researcher following up the therapy about the name and amount of drugs they used.
Assessment and results
Patients were assessed with measurements of visual analogue scale (VAS)-pain, Shoulder Pain and Disability Index (SPADI) and ROM with goniometer before and at the end of the treatment and in the post-treatment 1
VAS-pain has proven to be reliable and valid method in determining the degree of pain. It is a 100 mm straight line in horizontal axis. Distance from the lowest VAS level to point that the patient marked was measured in mm (0–100) and numerical values of patient’s pain severity were determined [22].
SPADI developed to assess the shoulder pain and disability consists of two parts. In part 1, a total of 5 questions in pain subgroup assess pain of the patient within the last week (VAS, 0: no pain and 10: worst possible pain) and in part 2, a total of 8 questions in disability subgroup assess the degree of difficulty in movement of the patient within the last 1 week (VAS; 0: no difficulty and 10: needs help). A total score of 0 means maximum well-being while the score of 130 means maximum sickness in SPADI consisting of 13 questions in total. In our study, SPADI was assessed separately as Shoulder Pain Index (SPI), Shoulder Disability Index (SDI) and total SPADI. Turkish validity and reliability testing of SPADI was performed by Bicer et al. in 2010 [23].
Shoulder ROMs (flexion, extension, abduction, adduction, and internal and external rotation) were measured as active and passive ROM with goniometer by the same researcher.
Sample size
The number of patients included in the study was determined according to the study results in literature review [24]. Minimum number of patients required was calculated as 26 per group by using
Statistical analysis
All statistical analyses were performed using SPSS software package (Statistical Package Social Sciences, version 22.0). Comparison of demographic data of the groups was performed using Student’s t-test and chi-square (
Comparison of the demographic characteristics, affected size and duration of pain between groups
Comparison of the demographic characteristics, affected size and duration of pain between groups
A total of 74 patients diagnosed with AC between November 2015 and December 2016 were assessed in terms of compliance to the study. Fourteen patients (5 patients who had major trauma or who underwent a surgical operation, 4 patients who underwent glenohumeral injection, 1 patient who was receiving malignancy therapy, and 4 patients who did not accept to participate in the study) assessed in the study were excluded. A total of 60 patients were included in the study. Both groups completed the study with 28 patients since infection developed in 1 patient in group 1 and 1 patient was lost to follow-up and 2 patients in group 2 were lost to follow-up in the 6
Flow diagram of participants in the study.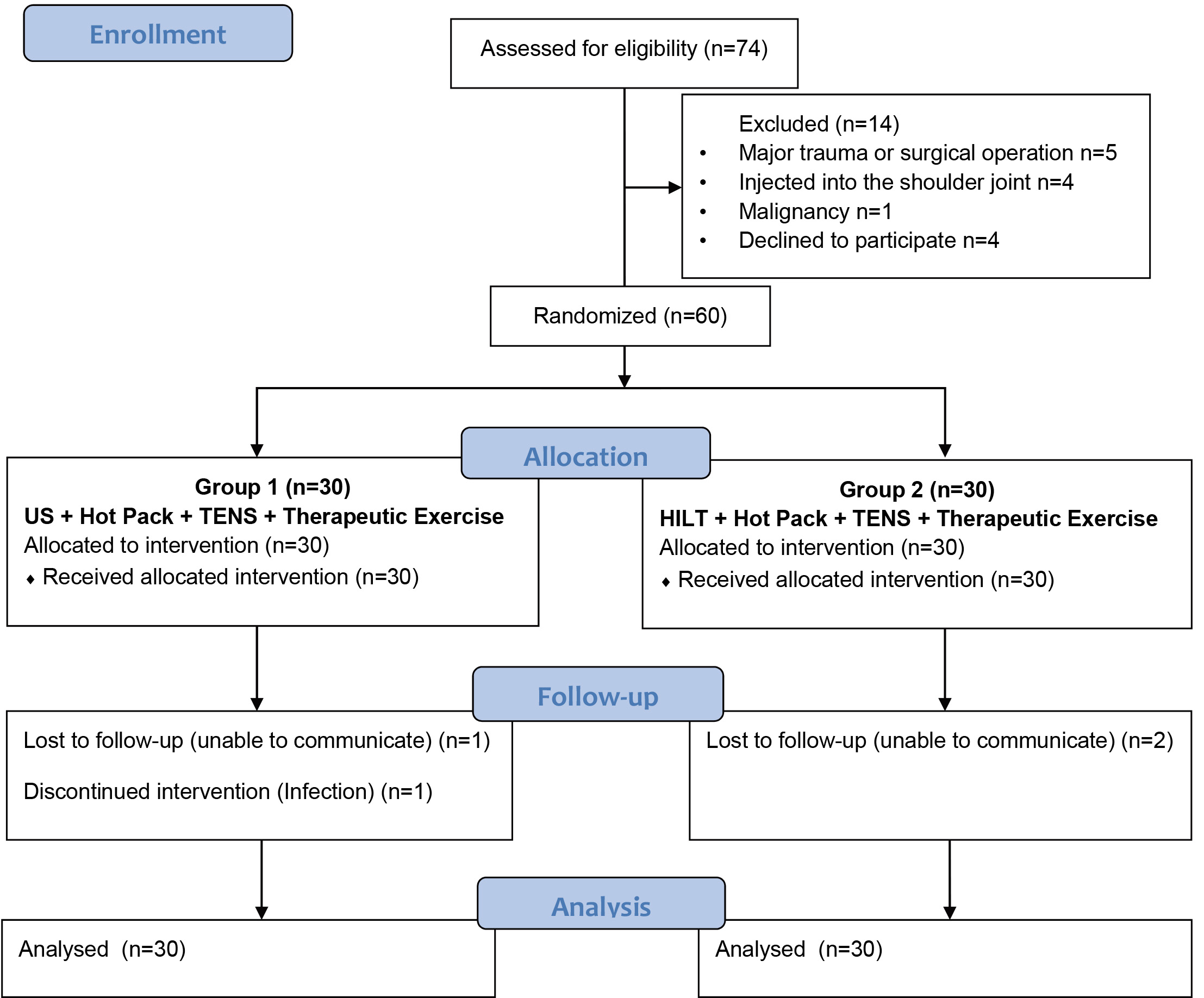
A total of 38 patients (67%) including 20 patients from group 1 and 18 patients from group 2 were female and mean age was 58. A total of 37 patients (66%) including 19 patients from group 1 and 18 from group 2 had left shoulder involvement. Mean duration of shoulder pain in patients was about 8 months. According to demographic characteristics of the patients, there was no statistically significant difference between the groups in terms of gender distribution, mean age, involved side, comorbidity, and pain durations (
There was no statistically significant difference between the two groups in terms of pre-treatment VAS-pain, SPADI and ROM values (
Comparison of the VAS-pain, SPADI, SPI, SDI and shoulder joint ROM values in pre-treatment between the groups
In intragroup assessment of the patients in group 1 and group 2, statistically significant improvements were observed in assessment parameters of VAS-pain, SPADI and ROM values measured at the end of the therapy and in the post-treatment 1
Comparison of the VAS-pain, SPADI, SPI, SDI and shoulder joint ROM values in T0, T1, T2 and T3 with in the groups
In intergroup assessment, there was no statistically significant difference in all parameters at the end of the treatment and in the post-treatment 1
Comparison of the change scores in VAS-pain, SPADI, SPI, SDI and shoulder joint ROM values between the groups
In this study, effectiveness of US therapy and HILT was compared in patients with AC. All patients in the study received a combined physical therapy program including hot pack, TENS and therapeutic exercises. One group received US therapy and the other group received HILT in addition to combined physical therapy program. We found a statistically significant difference in pain, ROM and functional condition evaluation parameters of both groups at the end of the treatment and in the 1
Many different treatment methods are used in treatment of musculoskeletal diseases such as medical therapy, physical therapy (Hot Pack, TENS, US, HILT, ESWT and exercise vb.), manipulation, local nerve blockades (with radiofrequency method or injections), and surgical interventions [16, 25, 26, 27]. Although many of these treatment methods are used in the treatment of AC, there is no definite consensus on the standard treatment [16]. Studies evaluating effectiveness of physical therapy practices in AC and recently published systematic reviews have indicated that there is strong evidence for ESWT and laser therapy, and moderate evidence for US therapy [16, 25, 26, 27]. However, the number of studies evaluating the efficacy of these electrotherapy modalities against each other in the treatment of AC is very few [16].
It was reported that deep heating agents used in the physical therapy practices were effective in relieving pain and improving ROM and functioning of the patients with AC [12]. Among deep heating agents, US and laser (HILT and low-intensity laser) therapies are used in the treatment of AC as well [10, 28]. In this study, we investigated the efficacy and superiority of two different electrotherapy modalities, US and HILT, which are among the deep heating agents in AC treatment.
Although US is commonly used as a part of physical therapy practices in the treatment of AC there are a limited number of studies assessing its effectiveness [29]. It is reported in systematic reviews that further high-quality studies are needed in this subject [16].
In the placebo controlled study in which the effectiveness of US on AC was assessed by Ebadi et al. [29], all patients received therapeutic exercises while one group additionally received real US and the other group received placebo US for a total of 10 sessions three times a week for 3 weeks. VAS-pain, ROM and SPADI measurements as the assessment parameters were assessed before and at the end of the treatment and in the post-treatment 3
In most of the other studies including our study, US therapy was used in combination with the other thermal or electrical agents in the treatment of AC [10, 30, 31, 32, 33]. In placebo controlled study by Dogru et al., one group received real US
Although there are differences between those studies and our study in terms of the US therapy’s length and number and frequency of sessions they are similar in terms of statistically significant improvements in the pain, SPADI and ROM values at the end of the treatment and in the post-treatment 1
In a systematic review assessing the effectiveness of US on AC, its use is recommended alone or in combination with conventional physical therapy methods to relieve pain, improve ROM and functional condition with moderate level of evidences [14]. Significant improvements observed in the short and long-term assessment parameters of the group receiving US therapy in our study support the recommendation in the systemic review.
Laser therapy in 2 different types including HILT and low-intensity laser used as another deep heating agent in physical therapy practices is used in the treatment of musculoskeletal diseases [16]. In systematic reviews, there are low evidences supporting the use of laser therapy with the other conservative therapies in AC to improve functional condition of the patients and high evidences for pain relief and improvement in ROM [16]. Recently, it is considered that HILT stimulates a larger area and deeper muscles and joints, thereby provides more improvement in pain and functional conditions compared with the low-intensity laser therapy [17]. Although HILT has been used in the treatment of musculoskeletal diseases recently there are a limited number of studies on HILT in the treatment of shoulder lesions and different results on its effectiveness have been reported. It has been stated that further studies are needed in this field [16].
In the study by Kim et al. [34], 66 patients with AC were divided into 2 groups. The patients in one group received real HILT and therapeutic exercises and those in the other group received sham HILT and therapeutic exercises three times a week for 3 weeks, 9 sessions in total. VAS-pain, VAS-satisfaction and ROM measurements of the patients in the pre-treatment period and post-treatment 3
In the randomized controlled study by Atan et al. [21], a total 36 patients were divided into 3 groups. In the study, group 1 received HILT
While short-term effects of HILT on AC were assessed in these two studies we also assessed long-term effects in our study. We found in our study that significant improvements in assessment parameters of the group receiving HILT continued in the long term.
The number of studies assessing the effectiveness of US and HILT on shoulder lesions is very low in literature. In our study, we compared the effectiveness of US therapy and HILT on adhesive capsulitis which is a shoulder lesion. Santamato et al. compared the effectiveness of US therapy and HILT on subacromial impingement syndrome which is another shoulder lesion. In that study, 70 patients were divided into two groups and one group received HILT while the other group received US therapy (a total of 10 sessions, five times a week for 2 weeks for both therapy groups). Patients were assessed with VAS-pain, Constant-Murley Scale and Simple Shoulder Test before and after the treatment. Although there was an improvement in the post-treatment VAS-pain, Constant-Murley Scale and Simple Shoulder Test values in both groups a statistically higher improvement was reported in the group receiving HILT [35].
In our study, while significant improvements were observed in both groups receiving HILT and US therapy there was no significant difference between the groups. Both studies compared the effectiveness of US therapy and HILT on different shoulder lesions. According to studies results, significant improvements were observed in groups receiving US therapy and HILT. While the group receiving HILT in the study by Santamato et al. exhibited more significant improvements there was no significant difference between the groups in our study. More effective results of HILT in the study by Santamato et al. may have resulted from disease diagnosis, patient selection and duration and number of sessions of HILT practice.
In our study, one group received US therapy and the other group received HILT in addition to combined physical therapy program consisting of hot pack, TENS and therapeutic exercises. While a significant improvement was observed in pain, ROM and functional conditions of both groups in the short and long-term follow-ups compared with the pre-treatment period no significant difference was found between the groups.
Limitations
This study had some limitations. The first one was that we had no control group. However, due to ethical reasoning, it was not possible to create a real control group who did not undergo any intervention. There is no effective standard treatment protocol accepted by everyone in the treatment of AC. Physical therapy modalities and therapeutic exercises together are used as a part of treatment.
Conclusion
US therapy and HILT were effective in relieving pain and improving ROM and functional conditions of patients in the treatment of AC and both therapy modalities had similar effects. We consider that addition of US therapy and HILT to combined therapies will be helpful in presenting variability and alternatives to physical therapy practices when their long term effects are taken into account; however, this should be supported with further randomized controlled studies in this subject.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
None of the authors declare any conflict of interest. All authors contributed equally to the manuscript and read and approved the final version.
Funding
This study was not funded.