
Abstract
BACKGROUND:
Body composition decline, lower limb impairments, and mobility deficits affect independence of older people. The exploration for a practical measure involving upper extremities may offer an alternative tool to be used by primary healthcare (PHC) providers for these individuals.
OBJECTIVE:
To explore reliability and validity of seated push-up tests (SPUTs) among older participants when used by PHC providers.
METHODS:
Older participants (
RESULTS:
The SPUTs demonstrated very good agreement, with excellent rater and test-retest reliability (kappa values
CONCLUSION:
SPUTs are reliable and valid for older adults when used by PHC members. The incorporation of such practical measures is particularly important during this COVID-19 pandemic with limited people’s hospital access.
Introduction
Older people frequently experience body composition decline, lower limb impairments, and mobility deficits that reduce their independence [1, 2, 3]. The limit hospital services due to healthcare uncertainties – for example, those caused by the ongoing coronavirus disease (COVID-19) pandemic – also have facilitated a healthcare paradigm shift towards increased demand for standard home- and community-based healthcare services for these individuals [4]. Such services are usually distributed through a primary healthcare (PHC) system (i.e., a practical, scientifically sound, and socially acceptable strategy) to enable universal access to individuals’ homes and communities with the aim of providing essential community-based healthcare services [5, 6]. The PHC systems need community health workers (or village health volunteers [VHVs] in Thailand), community residents or caregivers (CGs), and healthcare professionals, as the so-called the PHC providers, working cooperatively to deliver equitable healthcare services and facilitate community participation through multi-sectoral approaches [7]. Nevertheless, the involvement of lay people (e.g., VHVs and CGs) within a healthcare system requires appropriate, simple and practical tools that enable the execution of effective health-related activities in various settings [7, 8].
Existing evidence suggests the use of a hand grip test (HG), which involves the intrinsic muscles of the tested hand that are susceptible to decline with aging, to early detect many aspects relating to independence of older people (e.g., muscle weakness, mobility impairments and health problems) [9, 10]. However, the HG requires a specialized machine that limits clinical application in general community- and home-based settings [1, 10]. Moreover, the HG is performed in an open-kinetic chain, i.e., the tested arm is free in space without the need to overcome the bodyweight, that may reduce the challenging effects of the test [10].
Previous outcome studies and a review article reported the use of a seated push-up test (SPUT) as a practical and demanding measure that can be completed in a small area over a hard and even surface, such as a bed or chair [11, 12, 13]. The ability to complete the test requires the upper limb and upper trunk muscles working cooperatively to increase muscle force, joint torques, and upper limb loading to lift the body from the floor against the bodyweight while maintaining the body balance at the shoulder joints [11, 12]. A recent study found the moderate correlation between upper limb loading during a seated push up test (ULL-SPUT) and skeletal muscle mass (SMM) of older adults, whereby a pass in an SPUT, i.e., the ability of successful lifting the body from the floor, could indicate individuals with optimal SMM (nearly 30% of the bodyweight) [14]. However, that study assessed only the simplest form of SPUT, namely a single time SPUT (1SPUT) along with its ULL-SPUT, to reflect SMM of older people as measured using the Bioelectrical Impedance Analysis (BIA). The findings from BIA are susceptible to errors due to many factors such as electrode placements, skin conductibility, body temperature, and participant preparation (position, overnight fast, bladder voiding) [12, 13, 14]. With their simplicity, the present researchers hypothesised that SPUTs can be used by PHC providers. Furthermore, with their demanding, closed-association of the musculoskeletal system, and global physiological changes throughout the body systems [1, 2, 3], the researchers further hypothesized that the SPUT outcomes would be able to reflect muscle strength, body composition, and mobility relating to independence of older adults variously depending upon the specific characteristics of SPUTs. Therefore, this study examined the reliability (rater and test-retest reliability) and other related psychometric properties of the SPUTs, including the standard error of measurement (SEM) and minimum detectable change (MDC), when used by PHC providers, including health professionals, VHVs and CGs. Moreover, this study assessed the concurrent validity of the SPUT outcomes as verified using standard measures that have already been proven for their validity to reflect muscle strength, body composition, and mobility of older people.
Methods
Study design and participants
This observational study was conducted among participants who were PHC raters and older adults from many rural communities in a developing country. The recruitment criteria are outlined below.
PHC raters
The test-retest and rater reliability was assessed using nine PHC raters who had various working experience as the suggestion from a previous study [15], including health professionals, VHVs, and CGs (three assessors per group). The health professionals included an expert and two health professionals, whereby an expert was a health professional who had experience in using the SPUTs more than three years, and the other two health professional raters were novice and experience health professionals – 1 and 10 years working experience, respectively – both rarely used the SPUTs. The three VHVs graduated from secondary school and had 2 to 11 years of working experience. The three CGs were relatives or caretakers of older adults for more than 10 years [7].
Older participants
Community-dwelling adults aged 65 years and over with a body mass index (BMI) between 18.5 and 29.9 kg/m
Research protocols
Reliability study
Prior to the SPUT measurements, all raters were trained regarding the measurement protocols, instructions and outcome recording of the SPUTs by the expert. Then, they practiced the SPUT assessments using the video data of five non-participants. Subsequently, the PHC raters assessed the participants’ SPUT outcomes from the video data for two times with a seven-day interval. The data from the expert of both assessment periods were used to represent test-retest reliability. The SPUT data of all raters from the first measurement were used to report the inter-rater reliability of the SPUTs, and the data of the first and second assessments of each rater was analysed for intra-rater reliability [7, 15].
Outcomes measures
Older participants were interviewed and assessed for their demographics. Then, they were assessed for the outcomes of the study, including the SPUTs, as well as standard measures to reflect body composition, muscle strength and mobility needed for the independence and safety of older individuals [18, 19]. Details of the measurements are outlined below.
Seated push-up tests
Many forms of SPUTs are clinically available, including untimed and timed SPUTs [11, 12, 13]. This study applied simple with increasingly demanding forms of SPUTs, including 1SPUT along with its ULL-SPUT, a five-time (5SPUT), a 10-time (10SPUT), and 1-minute SPUT (1minSPUT), were applied according to the participants’ abilities, with no pressure to complete all the tests if they were unable to demonstrate feasibility of the tests. A recent study [14] reported the optimal outcomes of SPUT when performed in a ring sitting position (
1SPUT: The test was executed using push-up loading devices with the size of standard clinical push-up boards (18 cm in height) to quantify ULL-SPUT while completing a 1SPUT (Fig. 1) [12]. The devices were developed from digital load cells (Model L6E3-C, 50-kg 3G, with the standard calibration method based on UKAS LAB 14: 2006 mini-patent application No. 2103001612), with the outcome’s accuracy up to
Protocols of a seated push up test. (A) Starting position with push-up loading devices. (B) Position indicates “Pass” with push-up loading devices. (C) Starting position with push-up broads. (D) Position while lifting the body up from the floor. The participants who passed a 1SPUT proceeded to be assessed using the 5SPUT, 10SPUT and 1minSPUT, while the participants who failed terminated the SPUT and continued with the standard measures.
5SPUT: This test was modified from the five times sit-to-stand test (FTSST) [20]and completed using standard clinical push-up boards (Fig. 1C and D). The participants were in a starting position similar to that in a 1SPUT. Then, they were instructed to complete the five push-up repetitions at their fastest and safest speed. The time was recorded from the command ‘start’ until the participant’s buttocks touched the floor on the fifth repetition. The mean duration over the three trials was recorded.
10SPUT: Participants were in a starting position and performed the test similarly to that of the 5SPUT; however, they were required to complete 10 push-up repetitions, and the average duration over the three trials was recorded.
1minSPUT: The participants were in a starting position similar to that of the 1SPUT. Then, they were assessed for the maximum number of push-up repetitions in a minute over one trial [21]. During the test, the participants could take a period of rest as needed and continue the test as soon as they could or terminate it if they were unable to continue.

Subsequently, older participants were assessed using standard measures for muscle strength, including the HG and the back and leg strength test. Furthermore, they were assessed using mobility measures, consisting of the FTSST, the timed up-and-go test (TUG), the 10-meter walk test (10MWT), and the 2-minute step test (Table 1) to represent lower limb muscle strength, dynamic balance control and walking ability that are the ability needed for independent living [18, 19, 20]. These measures were performed in a random order by an experienced assessor. Participants wore a lightweight safety belt around their waist so that the assessor could provide assistance as needed. The participants could take a period of rest between the tests and trials as required (or at least 30 s) to minimise learning effects and fatigue that might occur due to sequences of the tests. Within seven days, the participants were at a hospital for the assessments of their body composition, including lean body mass (LBM), bone mineral content (BMC), and fat mass (FM), using dual-energy X-ray absorptiometry (Table 1).
Details of the standard measures used to report muscle strength, mobility, and body compositions
Note: ICC, intraclass correlation coefficient; SEM, standard error of measurement; MDC, minimal detectable change.
Descriptive statistics were used to explain the participants’ characteristics and study findings. Cohen’s kappa coefficient was used to analyse the agreement of the 1SPUT outcomes that provides dichotomous data, i.e., pass and fail. The kappa strength of agreement was interpreted as poor (
Demographics and outcomes for reliability and concurrent validity study
Demographics and outcomes for reliability and concurrent validity study
Note:
One hundred forty-six older participants, with a mean age of
All forms of SPUT demonstrated very good agreement, or excellent rater and test-retest reliability (kappa values for 1SPUT
Bland-Altman plot of seated push up test (SPUT) outcomes between test and retest sessions. (A) five-time SPUT (5SPUT). (B) 10-time SPUT (10SPUT). (C) 1-minute SPUT (1minSPUT).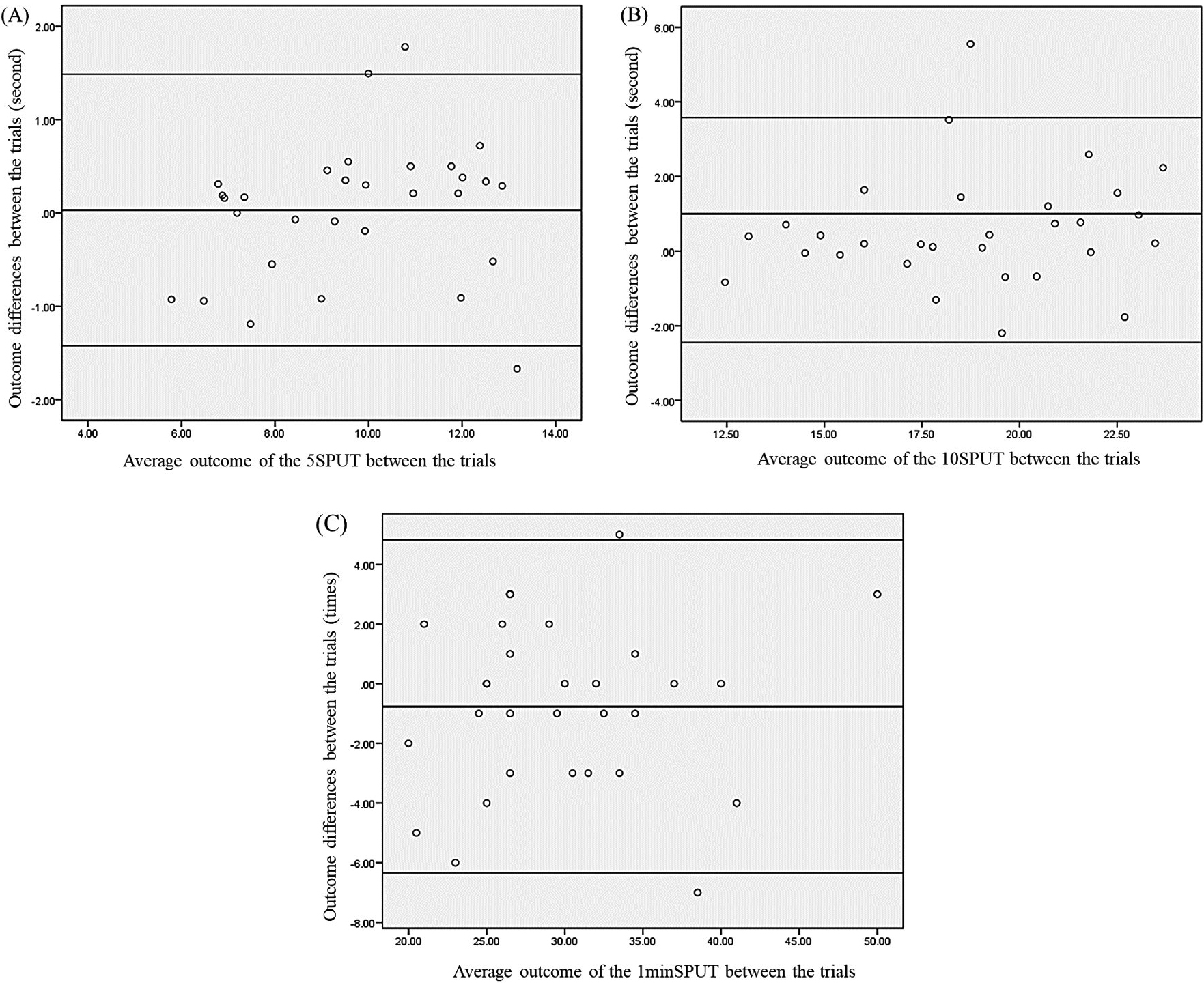
Table 3 presents the correlation between the SPUT data and the standard measures (concurrent validity). All SPUT forms demonstrated low-to-moderate correlations to muscle strength and mobility measures (
Older people face with many system decline and lower limb deficits affecting their independence. The ongoing COVID-19 pandemic also facilitates the need for the distribution of standard and effective community-based and home healthcare services for older adults. The present study examined the rater and test-retest reliability of the SPUTs when used by PHC providers, as well as their benefit. After training and practicing with a few older adults, the SPUT outcomes of PHC raters showed excellent agreement and intra- and inter-rater reliability compared to the expert (kappa and ICC values of
The excellent test-retest reliability of the SPUTs, with the small SEM and MDC found in the present study, suggest the internal validity of the SPUTs and ensure that the outcome obtained are representative and stable over time. The excellent rater reliability lies in the fact that the outcomes indicate the extent to which the data collected correctly represents the real ability not by any possible extraneous variables [37]. Therefore, these findings suggest the use of SPUTs among PHC providers for older people.
The present findings further confirmed the association between outcomes of the SPUTs and standard measures for the muscle strength of the upper limbs, trunk,
Rater reliability of the seated push up tests (SPUTs)
Rater reliability of the seated push up tests (SPUTs)
Note: ICC
and lower limbs; mobility; and body composition (
The significant correlation with LBM also suggests the benefit of the ULL-SPUT because the LBM is associated with protection against frailty and physical dysfunction, as well as with favourable cardiometabolic profiles driven mainly by increased insulin sensitivity in older adults [40, 41, 42]. The SMM is the largest reservoir of protein in the body and a source of amino acids for protein synthesis in other vital tissues during periods of stress, disease, malnutrition, or starvation. A low SMM is also associated with sarcopenia, frailty, risk of underlying diseases, and dependence of older people [3, 40, 41]. Therefore, the findings may suggest the use of low ULL-SPUT for the early detection of older adults at risk for sarcopenia, frailty, and metabolic syndromes. Moreover, mechanical loading while attempting to complete the SPUTs attributes compressive force to the bones and cardiovascular functions [3, 12, 14]. Thus, the 1SPUT and ULL-SPUT outcomes were also significantly associated with BMC (
However, in those who passed a 1SPUT, the data may face a ceiling effect – that is, scenarios where older participants obtained the upper limit of the ULL-SPUT and 1SPUT outcomes [43]. Thus, the outcomes cannot represent alterations over time. In such situations, the timed-based SPUT measures (5SPUT, 10SPUT, and 1minSPUT) are needed to inform further changes. However, the findings from these timed-based SPUTs showed similar weak-to-moderate correlation with the standard measures (
Nevertheless, no significant association between the outcomes of the SPUTs and body FM (
The present findings confirmed the reliability and validity of the SPUTs to be used by PHC providers for older people. VHVs are community members who are trained as lay health workers and considered to be the backbone of healthcare providers. Caregivers are people who provide direct care to older people [5, 7]. The present findings suggest the use of SPUTs as simple quantitative measures to promote the two cornerstones of PHC – namely community participation in the healthcare system and empowerment that leads to self-determination [36]. The ULL-SPUT and 1SPUT could be applied with all participants in the present study, whereas the time-based measures (5SPUT, 10SPUT, and 1minSPUT) could be completed by only those who passed a 1SPUT. None of the participants experienced adverse events after the tests. These findings suggest the clinical applicability of SPUTs in older people.
However, the findings have some limitations. The data were cross-sectionally collected from mostly well-functioning older adults with normal BMI. The generalisability of the findings might be limited to use in frail and obese older people. Furthermore, more than half of older participants were females, and the convenient sampling may contain selection bias. Nonetheless, the gender proportion was coherent with an existing study from the same country [44]. In addition, this study applied the standard clinical protocols of SPUTs [9, 15], whilst many factors could influence outcomes of the tests, such as elbow flexion angle, position of push-up devices, and size of the individuals. Therefore, a further prospective study with systemic sampling should be conducted in both healthy and frail older people with a wide range of BMIs to assess the factors affecting the outcomes of SPUTs, as well as their responsiveness when used by novice and experience raters to extend the clinical utility of SPUTs in older adults.
Demands for effective community-based rehabilitation and home healthcare services, particularly during the ongoing COVID-19 pandemic, have increased the need for a standard practical measure that can be performed in various settings. The present findings suggest the use of SPUTs by PHC providers to reflect muscle strength, mobility, LBM, and BMC in well-functioning older people. The ULL-SPUT and 1SPUT could be applied in all older adults, whereas the 5SPUT, 10SPUT and 1minSPUT could be used to increase the difficulty of the test for older people with good physical ability. The incorporation of such tests may promote standard screening, monitoring, and data transfer among PHC providers in various clinical, community, and home-based settings.
Ethics statement
The research protocols of this study were approved by the Institutional Ethics Committee for Human Research (HE 622255). Participants needed to sign a written informed consent form prior to participation in the study.
Funding
This study was supported by funding from the National Research Council of Thailand (NRCT) (5/2564 KKU-NRCT) and the Fundamental Fund (2023), Khon Kaen University, Thailand.
Author contributions
All authors were responsible for the research conceptualization, study design, and final approval of the manuscript. PC, PP and RI were involved in the data collection. PC and PP were engaged in the statistical analysis, data interpretation, and drafting of the the manuscript. SA was responsible for the funding application, research management, data interpretation, and finalized the manuscript.
Footnotes
Acknowledgments
The authors sincerely thank the National Research Council of Thailand and Fundamental Fund for the funding support.
Conflict of interest
The authors declare no potential conflicts of interest.