
Abstract
BACKGROUND:
In the motor rehabilitation of individuals with neurological disorders, including cerebral palsy (CP), Neurodevelopmental treatment (NDT) one of the most used approaches worldwide.
OBJECTIVE:
To verify muscle activation in NDT handling in individuals with severe CP using electromyography.
METHODS:
This was a controlled, cross-sectional, quantitative clinical trial. The individuals were evaluated using electromyography to analyze the muscular activation of the spinal erector, gluteus medius, rectus abdominis and multifidus during different NDT handling. We evaluated 59 individuals: 39 with spastic quadriparesis CP (Gross Motor Function Classification System, level IV–V) and 20 typically-developing individuals (control group). These groups were homogeneous with respect to age and gender.
RESULTS:
There was a significant difference in muscle activation of the spinal erector, gluteus medius, rectus abdominis and multifidus in the six NDT handling used in this study: side-sitting for kneeling; supine for lateral decubitus, prone position for lateral decubitus, “sitting on horseback”, sitting on the roll, and proprioceptive stimulation sitting on the ball.
CONCLUSION:
The results show that all NDT handling analyzed in this study were effective for muscle activation of the spinal erector, gluteus medius, rectus abdominis and multifidus in individuals with severe spastic quadriparetic CP.
Introduction
Cerebral palsy (CP) is a major cause of motor impairment in children [1], with spastic quadriparesis being its most severe presentation, where all limbs are affected. This condition is present in 10–20% of all individuals with CP [1, 2], and is related to prematurity and low socioeconomic status in prenatal care [3]. These patients present greater motor impairment, and changes in voluntary mobility, function and motor learning [1, 2], with significant functional limitations [3].
One of the main characteristics of individuals with spastic quadriparesis is poor trunk control, which directly interferes with body alignment, postural control and voluntary mobility [3, 4]. Furthermore, studies show that individuals with spastic quadriparesis also present atypical motor development due to issues such as deficit in muscle synergy and poor trunk control [3]. Therefore, it is known that the decrease in trunk control in individuals with severe CP is associated with a series of changes, such as worse postural alignment [5]. Thus, the children evaluated in this study are more severe (higher level on the GMFCS scale) and have a greater trunk control deficit [6], which justifies the choice of muscles analyzed in this study, since these muscles help control posture.
This deficit is mainly related to decreased trunk muscle activation, lack of acquisition of balance reactions, and poor positioning of the pelvis and femur [3, 4]. Thus, these disorders affect the capacity for exploring and learning, leading to consequences in multiple areas: behavioral, independence, motor, social and functional [3, 4]. Individuals with the most severe cases of CP, classified as levels IV and V according to the Gross Motor Function Classification System (GMFCS), present these impairments more eminently [3, 7].
Currently, there is a variety of therapeutic options proposed within the context of motor rehabilitation in cerebral palsy [8]. The Bobath Concept or Neurodevelopmental Treatment (NDT) [9] is one of the most widely used approaches worldwide in the rehabilitation of individuals with neurological disorders [9, 10, 11], and is among the most traditional therapy approaches used for motor intervention in CP [11, 12, 13, 14]. The positive effect of NDT on muscle activation is well established through practice bases evidence. It is aimed at solving problems with function, movement and postural control disorders originating from a lesion in the central nervous system [15], based on an integrative systems model, optimizing activity and participation [15, 16]. The current approach through contemporary Neurodevelopmental Treatment argues that the examination, assessment and intervention depend on knowledge of the human movement system, in addition to the understanding of postural control and typical and atypical development and is geared towards activity and participation. significant [17]. Thus, the concept is currently based on an integrative systems model, and is based on contemporary theories: Motor Control Theory, Motor Learning Theory and neuroplasticity, optimizing activity and participation and promoting quality of life [9]. In addition, it should be noted that, during NDT therapy, it is possible to measure muscle activation in individuals who have CP non-invasively using electromyography (EMG) [18].
However, the lack of evidence on the muscle activation during NDT handling is still a challenge for therapists. To date, among the limited studies found in the literature, most include only individuals who have milder motor impairment [8], with a lack of studies of muscle activation in this approach, especially in individuals with severe CP (GMFCS IV and V). However, despite the evidence of its efficacy being scarce, the use of NDT has been increasing [18, 19, 20, 21, 22].
Thus, EMG can be an important ally in the assessment of muscle activation during NDT handling in individuals who have severe cerebral palsy, in addition to contributing to the construction of evidence-based practices. In view of this, the main objective of this study was to analyze the muscle activation of the spinal erector (longissimu), gluteus medius, multifidus and rectus abdominis through EMG during NDT management in individuals who have severe cerebral palsy.
Material and methods
Design
A controlled, cross-sectional, quantitative clinical trial was conducted between September 2018 and September 2020 in rehabilitation and home institutions in the south of Brazil. This study was approved by the Human Research Ethics Committee of the Universidade Federal de Ciências da Súde de Porto Alegre (UFCSPA), under opinion no. 2.923.422. This study followed the STROBE checklist and was conducted in compliance with the current revision of the Declaration of Helsinki.
Participant
Our sample included 39 individuals with CP, selected for convenience according to the following inclusion criteria: (a) diagnosis ofspastic quadriparesis; (b) age between three and eighteen years old; and (c) motor level classified as level IV or V by GMFCS [7]. The exclusion criteria were: (a) orthopedic surgeries, tendon transposition, tendon stretching or rhizotomy in the six months prior to entering the study; and (b) application of botulinum toxin in the six months prior to entering the study. The control group consisted of 20 typically developing (TD) individuals, who did not present any musculoskeletal or orthopedic alterations, in the same age range as the CP group. The TD group went through the same process as the CP group.
Three assessment instruments were used before the start of electromyography. Initially, anamnesis was performed, where an evaluation form was applied to collect data such as age, and history of tracheostomy, gastrostomy, application of botulinum toxin and orthopedic surgeries. GMFCS was then used to evaluate gross motor function and classify the functionality of individuals with CP. This classification is based on the following aspects: trunk stability in the sitting posture, transfer between the sitting position and other postures, and forms of locomotion of the individual with CP. The GMFCS is divided into five levels (I–V): (Level I, walks without limitation; Level II, walking with limitation (no mobility aid in the first 4 years; Level III, walks using a manual mobility device; Level IV, self-mobility with limitations, can use mobility through a motorized wheelchair; Level V, transported in a manual wheelchair). This study included individuals with more severe impairments, classified as levels IV or V [7].
Finally, the most spastic muscle was evaluated using the Modified Ashworth Scale (MAS), which measures the movement resistance in a passive manner. The scale is divided into six scores ranging from 0–4 (0, No increase in muscle tone; 1, a slight increase in muscle tone, manifested by minimal resistance at the end of the range of motion, when the affected part(s) is (are) moved in flexion or extension;
Intervention
For the experimental trial, the sizes of the equipment used were selected according to the height of each individual, in order to favor the biomechanical alignment during the handling. For the therapeutic handling, balls (material: polyvinyl chloride; diameters: 55 cm, 65 cm, 75 cm) and rolls (material: foam with density 60 kg/m
Muscle activation was assessed during six NDT handling, shown in Fig. 1.
Flow diagram of interventions and illustration in the six Neurodevelopmental Treatment handling. 1:1: initial position of the handling; 2: final position of the handling; F: initial and final position of the handling; (A1–A2) Handling starts with the subject sitting on the floor in side-sitting with a roll in front of him, transfer to kneeling, key points on the hip and elbow; (B1–B2) Handling starts on the floor with subject in dorsal decubitus, transference to lateral decubitus is performed, keeping lower limbs in abduction, key points on knees; (C1–C2) Handling begins with the subject in prone on the roll, transfer to lateral decubitus, key points on knees; (D1–D2) Handling starts with the subject sitting on the roller with lower limbs forward and knees at 90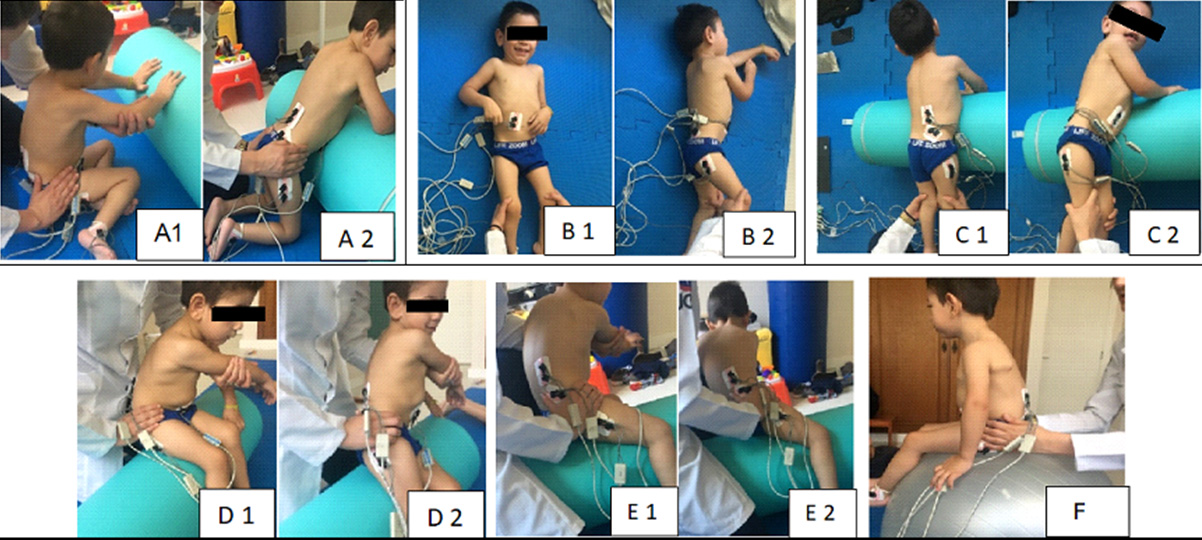
These handling were chosen because they are widely used in clinical practice. The execution was performed in a standardized manner, always performed by the same professional, an experienced therapist trained in NDT, as well as a second professional, who was responsible for collecting the electromyographic measurements. The handling sequence was randomized by an independent research assistant, to avoid any influence of the order of acquisition. Each block of randomization was composed of three participants, and the handling was performed on the same day. The key control points were used based on the Bobath Concept, with the aim of facilitating weight transfer and muscle activation [15]. Visual and verbal stimulation was performed in a standardized manner during handling for all children.
A USB port connection device was used for data collection (Miote
Four channels were used. The electrodes were placed on the right side of the body, positioned longitudinally in the direction of the muscle fibers over the muscle mass. For the spinal erector (longissimus), the electrodes were placed at two finger widths lateral from the process spin of L1; for thegluteus medius, they were placed halfway along the line from the iliac crest to the trochante; for the multifidus, they were aligned with a line from the caudaltip posterior spina iliac superior to the interspace between the L1 and L2 interspace, at the level of L5 spinous process, as described by SENIAM [24]; and they were placed on the rectus abdominis muscle mass. A reference electrode was placed on the lateral malleolus of fibula [24].
EMG processing
The processing of the collected data was performed using the MiotecSuite 1.0 software (Miotec, Brazil). A Dell
Sample characterization individuals with cerebral palsy quadriparetic spastic and typically developin
Sample characterization individuals with cerebral palsy quadriparetic spastic and typically developin
CP: cerebral palsy; TD: typically developin; SD: standard deviatio; F: female; M: male; GMFCS: Gross Motor Function Classification Scale.
Electromyography activation at rest vs handling in the cerebral palsy group and in the typically developing group
Abreviation: CP: cerebral pals; TD: typically developin; P25: percentis 25; P75: percentis 75.
To detect an average effect size (Cohen’s
Qualitative results were presented as a frequency and percentage, age as a mean and standard deviation, and activations as a median and 25
The effectiveness of handling in terms of muscle activation was assessed using the Wilcoxon test. To compare the magnitude of muscle activation between the six handling and the controls, relative activation was used, measuring the percentage of activation during handling compared to the activation observed at rest: (handling activation – resting activation)/resting activation. The statistical tests used to analyze these data were Friedman (with Dunn’s test for multiple comparisons), and Mann-Whitney, respectively. These analyses were performed using SPSS software version 25 and results with
Results
The general characteristics of the research participants are described in Table 1. The sample is homogeneous, since the groups do not show a statistically significant difference in age (
Comparison of relative muscle activation between handling in the cerebral palsy group and in the typically developing group
Comparison of relative muscle activation between handling in the cerebral palsy group and in the typically developing group
CP: cerebral palsy; TD: typically developing; P25: percentis 25; P75: percentis 75.
When comparing muscle activation at rest vs. activation during handling, the difference in electromyographic signal was statistically significant (
Comparisons of eletromyographic signal in diferent Handling in the cerebral palsy group
Comparisons of eletromyographic signal in diferent Handling in the cerebral palsy group
P25: percentis 25; P75: percentis 75. No significant difference in muscle activation of erector spinal and rectus abdominis between the six handling (
Table 3 compares the relative muscle activation between the CP and TD groups, where it was observed that, in most cases, the EMG signal was significantly higher in the TD group than in the CP group.
Comparison of relative muscle activation between handling in the CP group
In the analysis of the differences in relative muscle activation between the six NDT handling in the CP group, no difference was observed for the activation of the rectus abdominis (
Discussion
The main objective of this study was to use EMG to analyze the muscular activation of the spinal erector (longissimus), gluteus medius, rectus abdominis and multifidus during NDT handling in individuals with severe spastic quadriparetic CP. In addition, we evaluated which proposed handling are more effective, and whether muscle activation differs between them. The main finding was that all the handling analyzed were effective for the activation of the evaluated muscles. The results showed that the gluteus medius and multifidus were the most active muscles in the side-sitting for kneeling handling and in handling sitting on the ball.
We chose to analyze muscle activation in individuals with more severe CP due to the limited number of studies [8] and the complexity of this intervention in this population, who clearly present with more severe impairments. Deficit in trunk control and alteration of tone are commonly present [3], as demonstrated in this study, where spasticity was present in all individuals evaluated. The changes found in this population reflect the muscles we chose to evaluate in this study, which are important for trunk control and postural alignment [28]. Hence, more effective activation of these muscles can promote gain of function and improved quality of life in this population. The analyzed procedures were chosen because they are widely used in clinical practice during the rehabilitation of individuals with CP, and because, in general, the literature lacks evidence concerning muscle activation during rehabilitation with NDT, especially in individuals with more severe cerebral palsy (GMFCS IV and V) [8].
Regarding muscle activation in individuals with spastic quadriparesis, it was observed that, during the chosen handling, the analysis of muscle activation at rest compared to during handling showed a significant difference for all evaluated handling. Therefore, this study demonstrated that all the proposed handling are effective for muscle activation of the spinal erector (longissimus), gluteus medius, rectus abdominis and multifidus, even in this population with more severe impairments. This agrees with the findings of other studies that analyzed the activation of different muscles during other NDT handling in populations with severe CP [18, 20, 21]. Our findings contribute to addressing the gap found in a recent systematic literature review, which analyzed the influence of NDT treatment on CP, and identified a lack of information on this approach. This review identified a limited number of studies and an insufficient amount of solid information concerning the effect of NDT on different types of cerebral palsy, including spastic quadriparesis [8].
An increase in the amplitude of movement in the trunk is a marker of decreased dynamic instability [29]. Thus, improving dynamic stability and maintaining general mobility should be an important goal of therapy with individuals with spastic CP [29]. Another point to be considered is that the imbalance between the agonist and antagonist commonly found in CP progresses to muscle contracture, joint and bone deformities over time [29]. In this way, NDT can be an important method in the rehabilitation of this population, since it aims to improve function using postural adjustments that contribute to better body alignment and more effective muscle activation, for example, by encouraging movement through facilitation [15].
Individuals with spastic quadriparesis also present atypical motor development due to issues such as deficit in muscle synergy, alteration in tone, spasticity and poor trunk control [3]. Providing exploration in different postures can be important for the acquisition of motor skills. NDT can be a valuable tool in these objectives, since it is possible to assist in these gains through facilitation, improving postural stability and gross motor function in individuals with CP [30]. In view of this, we also evaluated whether any handling tecnhiques were more effective than the others, to aid the therapeutic planning during the interventions. Our study showed that, among the six NDT handling, the gluteus medius and multifidus muscles presented more effective activation during the side-sitting for kneeling and in sitting on the ball. This is in line with the results of a study that evaluated motor acquisitions in individuals with CP, including those with quadriparesis, and observed that, after three months of intervention with NDT, the individuals showed significant improvement in their ability to kneel [30], which supports the superior result during the handling technique side-sitting for kneeling found in our study.
Another handling technique that showed greater relative activation of the medius and multifidus gluteus was sitting on the ball through proprioceptive stimuli. Due to the characteristics of the evaluated population, handling on the ball was performed slowly through proprioceptive stimuli, using the properties of the ball and the patient’s weight. This was done without moving the patient’s body away from the surface, in order to promote greater stability, since patients with increased muscle tone may find this is exacerbated during sudden movement. There are already known therapies in which patients with severe impairment are subjected to slight body sway movements in order to promote muscle activation, alignment and body adjustment. An example of this is hippo therapy, the results of which were evaluated in a meta-analysis [31], showing positive results in individuals with CP. Thus, our findings demonstrate that providing small body oscillations with stabilization and minimizing compensatory strategies during sitting on the ball can be used as a form of muscle activation in individuals with more severe CP cases. Thus, it was observed that slow oscillations can lead to increased activation of the medius and multifidus gluteus, the latter having an important role as a spinal stabilizer [28].
The other two muscles evaluated, the rectus abdominis and spinal erector, showed no significant difference in activation between the handling. The authors suggest that perhaps other muscles not evaluated in this study may be more activated during the studied handling. Marques [32] mentions that the stability of the spine is not achieved by a single group of trunk muscles, but depends on the joint action of all of the muscles in that region, with the directions of the destabilizing forces determining which muscles are more activated. Nevertheless, the significant difference in muscle activation (
One limitation of this work was the heterogeneity of the sample and the methods used to normalize the EMG signal in individuals with atypical development, especially those with more severe affections, which the normalization method is not totally reliable. In addition, some of the changes found in the patients, such as orthopedic deformities, muscle spasticity, tone pattern, cognitive alteration and restlessness, can interfere with the EMG signal and need to be considered when interpreting the results. This study aimed to contribute to the literature on this topic, and to facilitate evidence-based clinical practice during the rehabilitation of individuals with severe cerebral palsy.
Conclusion
According to the results presented, we conclude that the six NDT handling evaluated in this study: side-sitting for kneeling; dorsal decubitus to lateral decubitus on the ground with abduction of lower limbs; ventral decubitus to lateral decubitus on the roll with abduction and lower limbs; “sitting on horseback” with trunk rotation and weight transfer to hi; sitting on the roll with lower limbs to front associated with trunk rotation and weight transfer to the hip; and proprioceptive stimulation sitting on the ball, are effective for activation of the spinal erector (longissimus), gluteus medius, rectus abdominis and multifidus in individuals with severe spastic quadriparetic CP. When comparing the handling with each other, it was seen that side-sitting for kneeling and sitting on the ball were more effective for the activation of the gluteus medius and multifidus.
Future research regarding muscle activation during NDT handling inindividuals with severe spastic quadriparetic cerebral palsy is recommended to reinforce the data found in this study and assist in addressing other gaps found in the literature, to improve the translation of scientific evidence into clinical practice.
Ethical approval
The study was approved by the Universidade Federal de Ciências da Saúde de Porto Alegre (number 2.923.422).
Funding
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior-Brasil (CAPES) (finance code 001).
Author contributions
TP provided the creation of the research planning and support in the field data collection, as well in the data analysis and in the writing of the paper. FZ provided support in the field data collection, as well in the data analysis and in the writing of the article. BTPM provided support in the field data collection, as well in the data analysis and in the writing of the article. BF provided support in the field data collection, as well in the data analysis and in the writing of the article. CCL provided support in the field data collection, as well in the data analysis and in the writing of the article. GCB provided support in the field data collection, as well in the data analysis and in the writing of the article. FC was the paper advisor, supported the research planning, guided the field data collection and part of the data analyses, as well supported the data analysis and writing of the article.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors declare that they have no conflict of interest.