
Abstract
BACKGROUND:
Resisted training of the trunk muscles improves outcomes in chronic low back pain (CLBP). The Itensic b-effect machine was designed to provide resisted training through posterior translation of the pelvis in a seated, forward-tilted position, in contrast with traditional machines that involve extension of the trunk.
OBJECTIVE:
To study the effectiveness of lumbopelvic training on the Itensic b-effect machine in individuals with CLBP.
METHODS:
Participants were allocated to 4 weeks of either progressive Itensic (I) training in addition to an education/exercise (EE) program (I
RESULTS:
RMDQ score improved more in the I
CONCLUSIONS:
Resisted posterior pelvic translation using the Itensic machine in addition to an education/exercise program improved disability, pain and mobility more than the education/exercise program alone.
Introduction
Low back pain (LBP) is a worldwide public health issue that affects 60–70% of adults in industrialised countries [1]. Chronic LBP (CLBP) can lead to physical deconditioning with a loss of muscle strength, cardiorespiratory endurance and mobility, all of which contribute to maintaining the cycle of chronic pain [2, 3]. Exercise therapy is the most common conservative treatment for CLBP, however the most appropriate and effective methods have not been determined [4].
Atrophy of the lumbar extensor muscles, in particular the multifidus muscle has been found in individuals with chronic LBP [5, 6, 7]. A systematic review found a negative relationship between the cross sectional area of the multifidus and LBP [7]. In consequence, rehabilitation frequently includes resistance training to strengthen the lumbar extensor muscles. A systematic review with meta-analysis of RCTs found that strength, endurance and electromyographic activity could be improved by specific training, although the quality of the evidence supporting these findings is low [8]. However, a review of 21 studies of isolated lumbar extension resistance training found that it improved clinical outcomes whether used as a stand-alone treatment or as part of a multimodal programme [9].
The Itensic series (Itensic, Dresden, Germany) of machines was developed specifically to strengthen the trunk muscles [10]. In contrast with other machines which involve movement of the trunk with a fixed pelvis, the Itensic machines fix the trunk to train pelvic translation against gravity by tilting the body. The Itensic b-effect device involves performing posterior pelvic translation in a seated, forward tilted position, and is thought to specifically target the lumbar extensor muscles. Furthermore, since the trunk and lower limbs are fixed, recruitment of other muscles such as the hip and lower limb muscles is expected to be minimal. The effects of training on this machine on outcomes in people with CLBP has not yet been evaluated.
The primary aim of this study was to test the hypothesis that resistance training on the Itensic b-effect machine in addition to an educational/exercise program would reduce disability more than the educational/exercise program alone. The secondary aim was to compare the effect of the Itensic training combined with the education/exercise program with the latter program alone on pain, lumbar muscle endurance, motor control and mobility in individuals with CLBP. We also wished to determine how well participants tolerated the progressive resistance Itensic program.
Materials and methods
This was a block-randomised, controlled parallel-group study conducted at the Clinique du dos (Spine clinic) (CHU-OA Esneux, Belgium) between November 2020 and March 2021.
Ethical approval was obtained from the Ethic Committee of the University Hospital of Liège (approval no. 2020-417, 12 November 2020). All participants signed an informed consent form for participation in the study.
Participants were assigned to either progressive Itensic (I) training in addition to a standard education/exercise (EE) program (I
Participants
Eligible participants were all adults between 18 and 70 years old who were registered in the multidisciplinary back rehabilitation program in our centre. Inclusion criteria were patients with non-specific CLBP (symptoms lasting for more than 12 weeks with or without referred symptoms) referred to a multidisciplinary back rehabilitation program.
All patients were examined by a physician, specialized in physical medicine and rehabilitation who conducted an interview and a physical evaluation to determine if they were eligible to start a functional multidisciplinary back rehabilitation program. In accordance with the Belgian clinical guidelines (KCE Report 287), patients were eligible if they suffered from non-specific CLBP pain defined as a pain in the back between the bottom of the rib cage and the buttock creases, not attributable to a recognizable, known specific pathology.
In addition, each patient underwent a baseline evaluation session including an assessment of pain intensity (Numeric Pain Rating Scale), disability (Oswestry Disability Index), and spinal function (trunk strength and endurance, mobility of the pelvis and lumbar spine). The content and effectiveness of this program in chronic low back pain has been reported previously [11].
Exclusion criteria were disorders that affected the lungs or thoracic cage (since use of the machine involved pressure over the ribs), spinal surgery less than 3 months previously, and pregnancy. Participants were also excluded if they started the reconditioning phase before the end of the educational/exercise phase (see below). Participants had to participate in at least 6 of the 9 education/exercise and Itensic training sessions, therefore those who participated in five or less were excluded.
Interventions
The multidisciplinary back rehabilitation program is composed of a total of 36 two-hour sessions. This study was conducted during the first part of the program which consisted, after the baseline session, of an educational and basic exercise phase (9 sessions).
Both groups (I
Participants in the I
The Itensic b-effect machine
As shown in Fig. 1, the participant sits on a seat that is tilted forwards. The seat slides backwards and forwards on a rail. The thorax is supported and the hands rest on two handles. The feet are not supported but a support is provided anteriorly to the ankles. The exercise consists of actively pushing the pelvis posteriorly by performing a translation movement (that is associated with an anterior pelvic tilt). The return (forward translation associated with a posterior pelvic tilt) is eccentric.
Illustration of the Itensic device and the 3 levels of inclination used for the study.
The exercise can be progressed by increasing the forward incline of the seat. Seven different inclines are possible, and the angle of the trunk and arm supports is changed with the incline of the seat. For this study, we used three forward inclines of the seat (10
Progression of the Itensic training
The primary endpoint was a between group difference in disability (measured by the: Roland Morris Disability Questionnaire, RMDQ) of at least the minimal clinically important difference of 3 points [12]. Secondary endpoints were between-group differences in instantaneous and maximal pain (on a 0–10 numeric rating scale, NRS), forward flexion (finger-floor distance), motor control of the back muscles (thoraco-lumbar dissociation test) and trunk extensor endurance (Sorensen test).
Outcomes for both groups were measured prior to beginning the program and after the final (ninth) session by the same therapist who performed the Itensic sessions (non-blinded).
The French version of the RMDQ (l’Echelled’Incapacité Fonctionnelle pour l’Evaluation des Lombalgiques chroniques: EIFEL [13]) was used to evaluate disability related to LBP [12]. It is composed of 24 questions (max
Pain intensity was evaluated using 0–10 NRS. Instantaneous (i.e. pain at the time of evaluation) and maximal pain during the past 7 days were rated. Participants were asked “How would you rate the pain that you feel now in your low back and/or in your leg?” and “How would you rate the maximal pain that you felt in your low back and/or in your leg during the last 7 days?”. The MCID difference for pain ratings on a NRS is 2 points [14].
The finger-to-floor test was used to evaluate spinal and pelvic mobility [15]. The participant performed trunk flexion in standing with the knees extended; the distance between the tip of the middle finger and the floor was measured (in cm).
Motor control was evaluated using the thoracolumbar dissociation test [16]. The participant sat on a stool adjusted to 110% of the height of the head of their fibula, hands resting on their thighs. They watched a video on a screen positioned in front of them. The video provided instructions and a demonstration of ten pelvic tilt movements. The participant then performed the movements simultaneously with the video. Performance was rated on a 5-point scale: quality of pelvic movement, control of adjacent segments, directional preference, breathing and repetitions. Maximum score is 10 points, and higher scores indicate better performances.
The Sorensen test was used to evaluate isometric endurance of the trunk extensors [17]. The subject lay in prone on a “roman chair” – a table on which the lower legs are fixed and the part on which the trunk lies can be lowered. Once the trunk rest was lowered, a stool was placed under the trunk and the participant was asked to maintain a horizontal position. Endurance time was measured from the moment they removed their hands from the stool until the moment they replaced them on the stool, or if the trunk dropped below the horizontal, using a stopwatch. This test has satisfactory reliability and is sensitive to change [18] however may be influenced by factors such as competitiveness, motivation and pain tolerance [19].
Pain was also evaluated before and after each Itensic session (with a pain NRS) and perceived effort was rated with the Borg scale at the end of each Itensic session. The latter is rated from 6: no effort to 20: maximal effort [20].
Participants were asked to report any adverse events at each evaluation session as well as at each training session.
Statistical analysis
The sample size was estimated using power-based sample size calculations. Based on an estimated standard deviation of 3 points on the RMDQ questionnaire, the planned sample size was estimated at 21 participants per group to detect a 3 points on the RMDQ questionnaire (
After the Shapiro-Wilk test, the variables are expressed as means (SD) (if the distribution was normal) or medians (interquartile ranges) (if the distribution was not normal).
We used the Student
Within groups changes from pre to post training and between group differences were compared with the Student
We used repeated measures ANOVA to compare pain and Borg ratings between the nine Itensic training sessions and the Wilcoxon signed rank test to compare pain between the start and end of each session (difference between mean pain rating at the start of the sessions and mean rating at the end of the sessions).
In addition, we reported the proportions of participants who achieved the MCID for the RMDQ and pain ratings.
We calculated effect sizes with Cohen
Statistical analysis was performed using R Commander for R statistical software, and
Subjects characteristics
Subjects characteristics
Flow diagram of inclusions.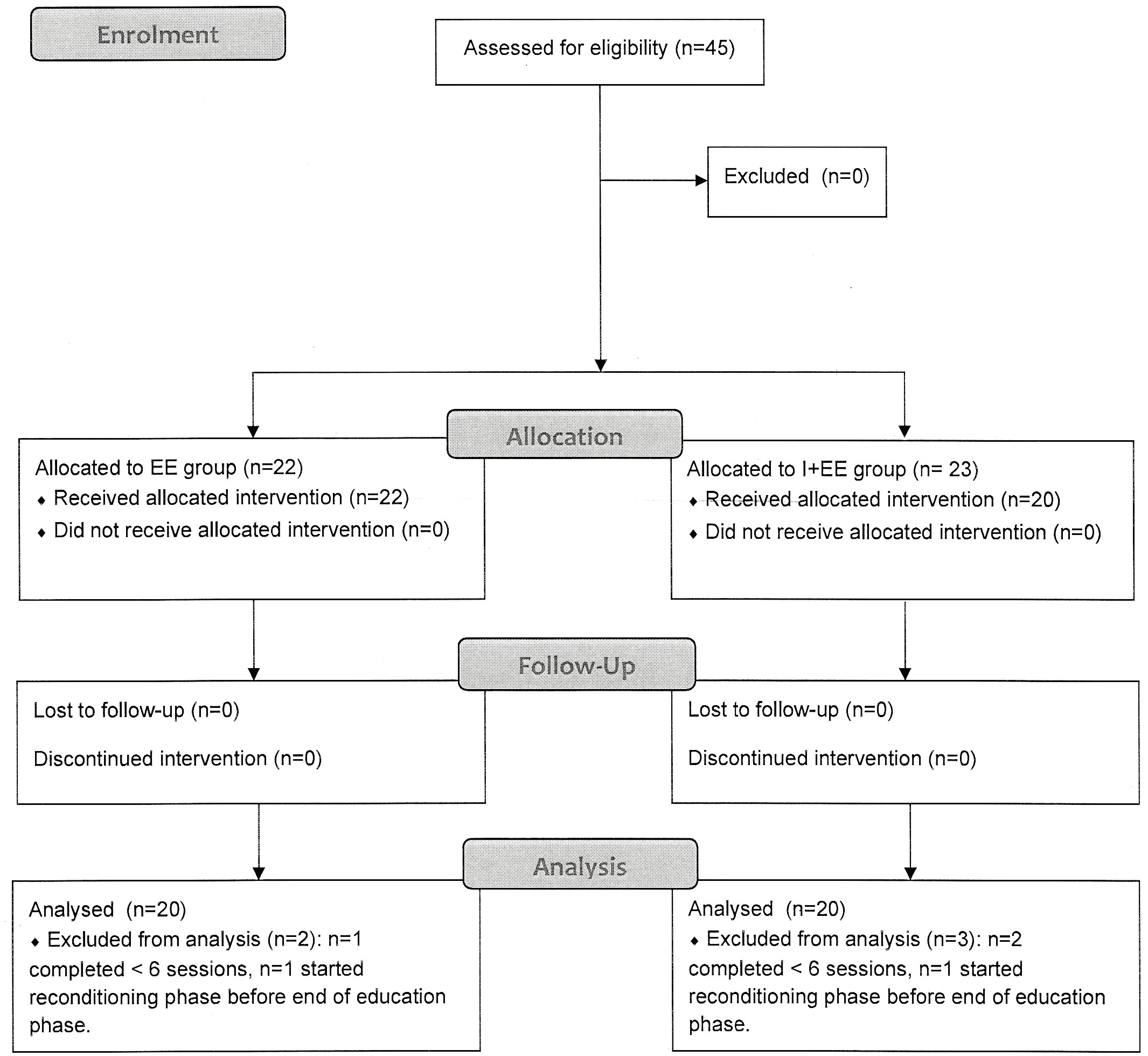
A total of 45 participants were included in the study, 22 were assigned to the EE group and 23 to the I
RMDQ improved significantly in both groups but was significantly more improved in the I
Instantaneous and maximal pain both improved only in the I
Finger-floor distance did not improve in either group, however, was significantly smaller in the I
Results of the outcome measures pre and post training for each group and between-groups comparison
Results of the outcome measures pre and post training for each group and between-groups comparison
Values in bold indicate statistically significant differences. RMDQ: Roland Morris Disability Questionnaire.
Pain at the start and end of each training session on the Itensic device. Data are means and standard deviations. NRS: numerical rating scale (range 0–10). 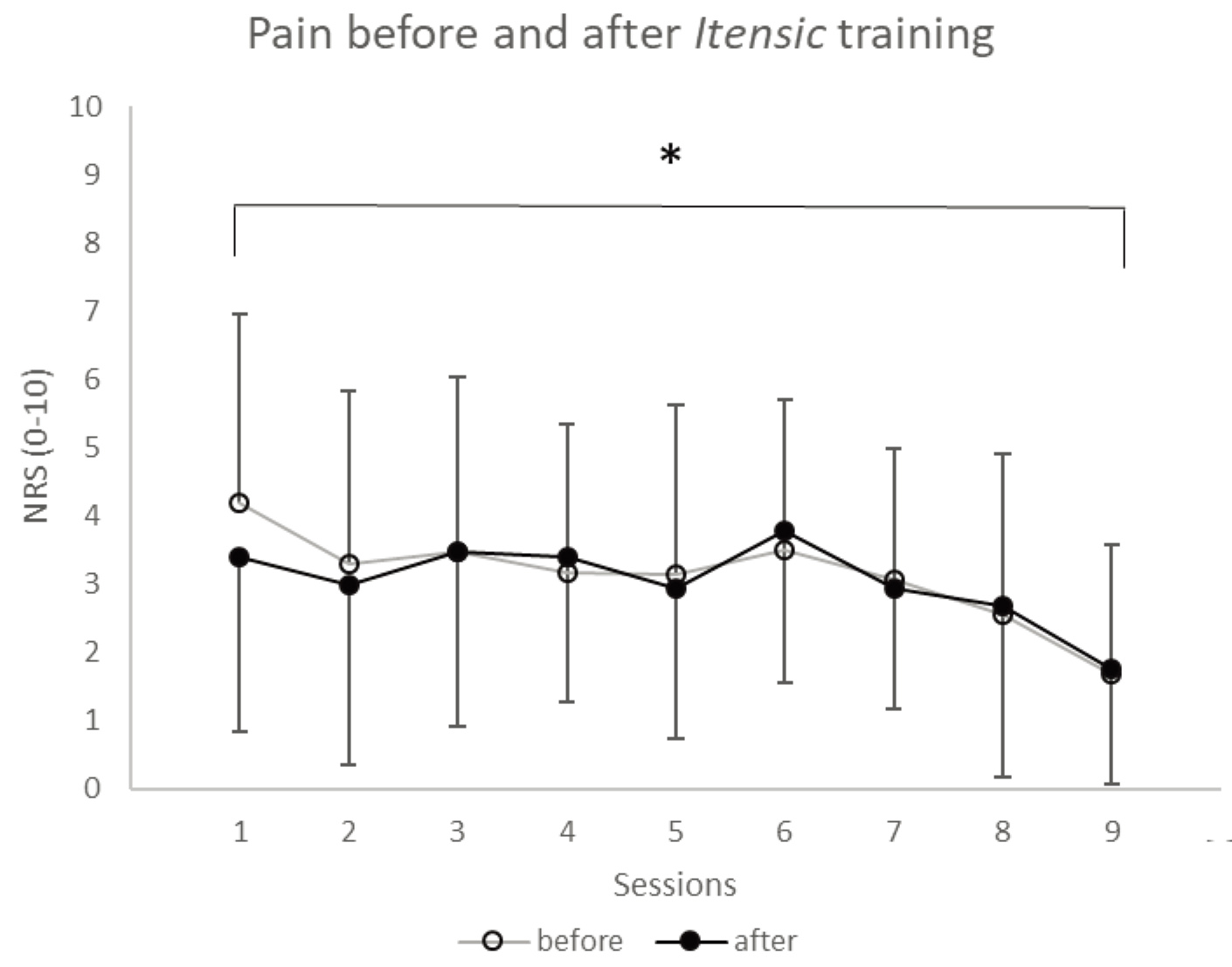
Borg scale ratings of perception of effort at the end of each training session on the Itensic device. Data are means and standard deviations. Borg scale range: 6–20. 
Mean pain intensity did not increase from the start to the end of any of the Itensic sessions, and decreased significantly from the first to the last session (Fig. 3). The perception of effort increased over the course of the Itensic sessions with significant increases between each phase (Fig. 4).
Adverse events. No participant reported any adverse events during the Itensic training sessions or at the evaluation sessions.
This study evaluated the impact of lumbopelvic translation training using an original machine (Itensic b-effect) on disability and pain. At the start of the program, none of the variables evaluated differed between groups. At the end of the 9-sessions training program, disability measured by the RMDQ was significantly lower in the I
The educational component of the program included some low-intensity motor control exercises that were mostly designed to reduce the fear of movement and exercise. In contrast, the exercises performed on the Itensic machine were specific and intensive, particularly towards the end of the program. Intensive exercise programs of various types have been shown to improve outcomes in CLBP [21] and appear to be more effective than programs of moderate intensity [22].
Comparison of the results of the present study with those of 23 other studies of isolated lumbar extension training provided in a review on this subject [9] showed that the improvements in pain and disability found in the present study were often larger and occurred over a shorter period of time; furthermore the drop-out rate was low (3/45 participants) in the present study. For example, a recent study found a reduction in pain of 27/100 points (VAS) and no change in disability after 20 sessions of extensor training over 10 weeks [23].
Comparison of the results of the present study with those of a previous study that evaluated the effects of the full program usually provided in our department showed a similar improvement in disability and a similar reduction in pain after only 9 sessions of education/basic exercise
Although many differences exist between these studies, a difference which we believe to be important is the method of performance of lumbar training. In many studies, lumbar extension is trained by upper trunk extension over a fixed pelvis [23, 24, 25]. In contrast, on the Itensic machine, the upper trunk is fixed, and participants specifically perform large lumbopelvic translations and tilts of the pelvis via alternate concentric (for the movement against gravity) and eccentric (for the return movement) contractions of the lumbar muscles. This large amplitude movement in the lumbar region may improve confidence and reduce kinesiophobia, which is related to disability [2, 26]. It may also serve to retrain proprioceptive function. Indeed, this type of exercise is used in motor control training to improve awareness of the lumbar area, posture and motion [27]. Furthermore, mobility (finger-floor distance) only improved in the Itensic group, which suggests that the large amplitude movement mobilised the lumbar spine and relaxed muscles resulting in an increased forward bending capacity. Reduction in fear of movement may also have played a role in this increased mobility.
The effects of resisted lumbar exercises on lumbar muscle health vary in the literature. To date, there is no conclusive evidence that such exercises result in muscle hypertrophy (or reduction of atrophy) or that they reverse changes such as fatty infiltration [23, 28]. Low quality evidence suggests that resisted exercise improves lumbar muscle strength and endurance [8]. Correlations between increased lumbar muscle strength and clinical outcomes are not as strong as might be expected [29]. Despite this, resisted exercise has been found to reduce pain and disability. A systematic review and meta-analysis found a greater effect of resistance training of the extensor muscles (with no specific resisted lumbar extension exercises) than for general exercise, particularly for programs of longer duration (12–16 weeks) on pain and disability [30]. A reduction in neuromuscular inhibition is therefore the most likely explanation for the algofunctional effect of our training program. This is supported by the fact that endurance measured by performance on Sorensen test did not improve significantly.
Factors such as strength and erector spinae size appear poorly related to disability: only changes in pain, psychological distress and fear avoidance behaviour explain improvements in disability following an active exercise program [31]. We found a significant reduction in both maximal and instantaneous pain in the I
The improvement in motor control likely resulted from the education and basic exercise component of the program since improvements occurred in both groups with no between-group differences. The Itensic exercise trains dissociation by constraining trunk movement while the pelvis moves; the dissociation is therefore not performed consciously as is the case for motor control exercises. This may explain why the between-group difference was not significant.
We measured pain at the beginning and end of each Itensic training session, as well as the perception of effort produced during the session with the Borg scale to evaluate how well participants tolerated the program. The program involved progressively increasing resistance over the course of the sessions. The results showed that participants were able to increase their level of effort as the resistance increased and that this did not lead to an increase in pain; this suggests that participants tolerated the program well. Furthermore, anecdotal comments from participants suggested that they enjoyed training on the Itensic machine, and felt their back muscles working, although some found the thoracic support uncomfortable. These results show that it is possible to begin a program rapidly with intensive exercise, rather than begin with gentle exercise and add resisted exercise at a later stage, which is how our full program is currently designed.
Limitations
The fact that the evaluator was not blinded to group allocation constitutes a limitation of this study. Furthermore we did not use EMG to evaluate the specific recruitment of the lumbar extensor muscles during the exercises realized on the Itensic machine.
Testing the directional preference would have been relevant to classify subjects into subgroups and see if subjects preferring lumbar extension would have obtained better results.
Conclusions
Current guidelines recommend the provision of multimodal, multidisciplinary programs that include exercise therapy and psychosocial/education interventions [35, 36, 37, 38, 39]. The results of the present study suggest that the inclusion of resisted lumbopelvic translations could enhance outcomes when included in such programs.
Perspectives
Future studies should use EMG to determine if training on the Itensic machine specifically targets the lumbar extensor muscles and longitudinal studies should also be performed to determine the long-term effects of such training. Studies should also compare the effects of trainng on this device with training on more traditional trunk extensor training devices.
The training duration was quite short – only 9 sessions over one month. Future studies should evaluate the effects of longer training durations.
Footnotes
Acknowledgments
The authors thank Johanna Robertson for writing assistance.
Conflict of interest
The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript: there is no relationship between this article (and its authors) and anyone who has created or promoted the Itensic device.
Funding
This research received no funding.