
Abstract
BACKGROUND:
In recent years, percutaneous kyphoplasty (PKP) has been increasingly used in clinical settings.
OBJECTIVE:
In this study, we aimed to determine the analgesic effect of intravertebral lidocaine injections in PKP.
METHODS:
A total of 60 patients who were treated with PKP were enrolled in this study. Lidocaine hydrochloride was chosen as the medication for the experimental group. Patients were randomly assigned into three groups using a double-blind study design: In group A (20 cases), no drugs were injected into the vertebral body during surgery; group B (20 cases) received intravertebral injection of normal saline; and in group C (20 cases), lidocaine hydrochloride was administered into the vertebral body during surgery. The age of patients, operation time, balloon dilatation pressure, balloon dilatation volume, and amount of bone cement injected were compared across the three groups. A pain visual analog scale (VAS) was used to assess pain suffered by the patients before, during, and 24 hours after the surgery.
RESULTS:
Age, operation time, balloon dilatation pressure, balloon dilatation volume, and amount of bone cement injected did not differ significantly among the three groups (
CONCLUSION:
Intravertebral injections of lidocaine during PKP can successfully reduce intraoperative pain.
Introduction
In an ageing population, osteoporotic vertebral compression fracture (OVCF) is a common complication that causes severe physical pain [1, 2]. The advantage of percutaneous kyphoplasty (PKP) over conventional vertebroplasty is that it is more conducive to restoring the height of the anterior edge of the vertebral body, relieves pain symptoms, and has a lower leakage rate [3]. In recent years, PKP has been increasingly used in clinical settings, particularly in line with the notion of rapid rehabilitation surgery [4]. It is clinically recommended that patients with OVCF who meet the surgical criteria get early intensive vertebral treatment in order to improve their quality of life, reduce the incidence of complications, and increase their survival rate [5]. Generally, local infiltration anesthesia or general anesthesia are employed for surgical anesthesia [6, 7]. These two anesthetic techniques have their own advantages and disadvantages. A relevant literature search revealed few publications on the use of local anesthetics to alleviate intraoperative and postoperative PKP discomfort [8, 9]. In a prospective controlled trial designed to reduce intraoperative discomfort and improve the surgical experience, lidocaine was injected intravertebrally during PKP to give patients with a more satisfying analgesic effect and an overall better surgical outcome.
Data and methods
General information
Inclusion criteria: Age
We enrolled 30 males and 30 females who underwent PKP in the Orthopedics Department of The 967th Hospital of Joint Logistic Support Force of PLA between July 2017 and December 2020 and met the inclusion criteria. Their ages ranged from 60 to 88 years old, with an average of 74.36
Surgical methods
All patients received bilateral double-balloon dilatation PKP. During the operation, blood pressure, heart rate, and blood oxygen saturation were monitored. The patients were in a prone position, with the chest and abdomen suspended. Under C-arm fluoroscopy, the body surface projection and puncture location of the pedicles on both sides of the affected vertebra were identified. The periosteal surface was anesthetized with lidocaine hydrochloride at a concentration of 1% by means of a shallow-to-deep injection of the drug via the skin. A 5 mm incision was created along the dermatoglyphic on the skin at the entry point of the needle. Under the perspective of a C-arm X-ray, the working channel was positioned along the pedicles of both sides of the afflicted vertebra, approximately 0.5–1 cm in front of the posterior edge of the vertebra. At this time, patients in group A received no medication, patients in group B were injected with 1.5 ml of normal saline on each side (3 ml total) of the vertebral body through the working channels on both sides, and patients in group C were injected with 1% lidocaine hydrochloride (1.5 ml total) into the vertebral body through the working channels on both sides. After observing for 0.5–1 minute, a balloon was inserted into the vertebral canal via the working channel, and the contrast medium (iohexol) was administered into the balloon using a pressure pump in order to open the damaged vertebra. The contrast medium was expelled, and the balloon was withdrawn. Under the guidance of a C-arm X-ray, polymethyl methacrylate (PMMA OSTEOPAL
The PKP simple process. a: Vertebral height is reduced. b: Bilateral needle placement (side of the slice). c: Bilateral needle placement (orthostatic position film). d: Balloon expansion. e: The cement is filled (side of the slice). f: The cement is filled (orthostatic position film).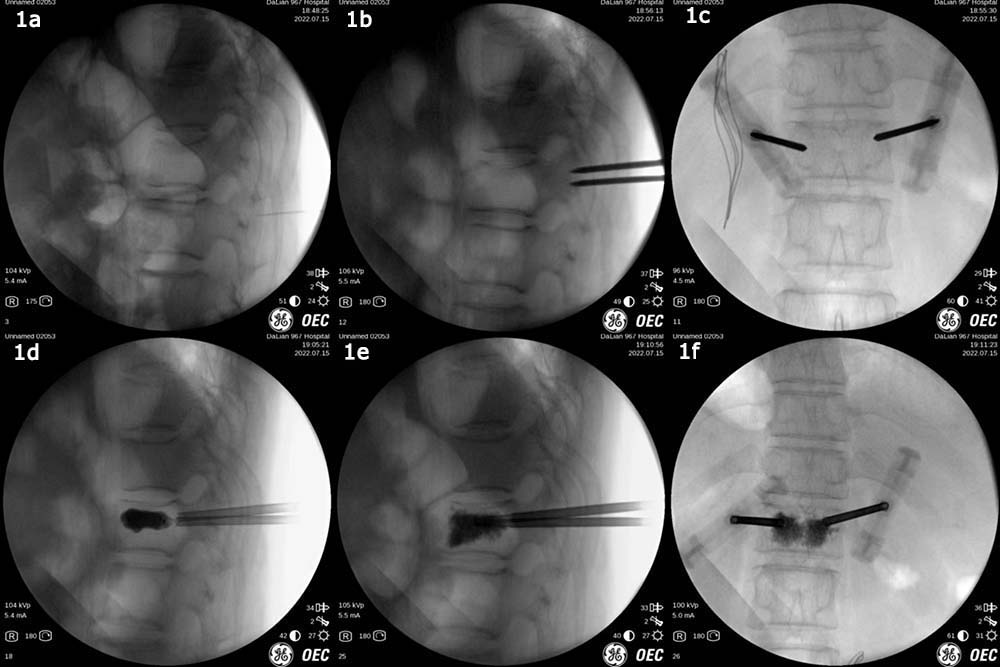
A pain visual analog scale (VAS) was used to assess patient discomfort before, during, and 24 hours after surgery [10]. The scores for intraoperative balloon dilatation and bone cement injection were examined repeatedly, with the highest score retained as statistical data. All pain scores of the patients were calculated by personnel who were blinded to the study.
Statistics analysis
Data were statistically analyzed using the SPSS 20.0 software. Measurement data were expressed as the mean
Results
Age, weight, and height did not differ significantly among the three groups. The average operation time in group A was 6.6 minutes less than that in group B, but there was no statistically significant difference between the three groups. The balloon dilatation pressure was greater in group C than in group B, and the difference was statistically significant (
Comparison of general data among three groups of patients
Comparison of general data among three groups of patients
Notes:
Comparison of VAS scores among three groups of patients
Notes:
There was no significant difference between the preoperative and postoperative VAS scores of the three groups 24 hours after the surgery. Group C had a lower intraoperative VAS score than groups A and B, and the difference was statistically significant (
Thoracolumbar compression fractures are highly prevalent among the elderly [11]. Due to the likelihood of elderly patients having greater complications, such as one or more medical conditions, the surgical risk is high [12]. Therefore, patients are typically provided conservative treatment. Long-term bed rest increases the risk of complications including hypostatic pneumonia, bedsores, and even pulmonary embolism [13]. PKP is often used to treat thoracolumbar compression fractures in elderly patients due to its satisfactory curative result, relatively simple and safe operation, and lower trauma [14, 15]. In a study by Salvatore et al., all 16 patients treated with PKP saw considerable and long-term reduction in symptoms, and the strength of the vertical body increased, while maintaining its natural shape [16]. Commonly, local infiltration anesthesia or general anesthesia is applied in PKP [17]. Although general anesthesia has a strong analgesic effect, it raises the risk of nerve damage [18], increases the risk of anesthetic and respiratory problems, hinders early rehabilitation, and raises costs [19]. Local anesthesia is safe and rarely causes complications [6]. In our experience, however, local anesthetics are typically injected into the soft tissue and periosteum outside the afflicted vertebrae. When the operation channel is inserted through the pedicle, the balloon is expanded in the vertebral body, and bone cement is poured into the vertebral body, the patient suffers severe pain, according to our experience. Due to stress, pain response, and other incentives, some patients are unable to collaborate well with doctors during operations. These factors increase operation risk and operation time while leading to a poor operation experience. Notably, cement leakage did not occur during any of the surgeries included in our study.
The analgesic mechanism of PKP can be summarized in three points [20, 21]: 1. Following the injection of PMMA cement into the vertebral body for coagulation, the microfracture is fixed, which improves the strength and stiffness of the vertebral body and decreases the stimulation of nerve endings caused by spinal instability. 2. The heat generated during PMMA polymerization can promote degeneration and necrosis of painful nerve endings surrounding the bone cement, thereby reducing pain. 3. The cytotoxicity of PMMA may reduce the pain sensitivity of nerve-ending cells. Sesay et al. studied venous blood samples taken from patients at multiple time intervals after 5 ml of 1% lidocaine was injected into the vertebral body, to measure the lidocaine concentration [22]; the highest plasma concentration was still considerably lower than the toxicity-producing value. To ensure the safety of anesthesia in this study, we selected 3 ml of 1% lidocaine hydrochloride.
These are the limitations of this study: First, no study power calculation performed, and each group included only 20 patients. Second, the study population included patients with both acute and chronic pain, however the duration of pain was not employed as an indicator in the observation, nor were Roland-Morris Disability Questionnaire or Oswestry Disability Index feature scores used in this research. In the future, we shall evaluate this as an observational indicator. The primary objective of this study was to analyze the analgesic effect during surgery. In the future, we will examine radiological and functional assessment.
According to the study results, the patients suffered the most excruciating pain during the operation when the balloon dilated the vertebral body and restored its height. The results of this study revealed that the approach of injecting lidocaine into the vertebral body to reduce patient discomfort during balloon dilatation and bone cement injection has obvious analgesic effects, is easy to use, and is extremely safe.
Conclusion
There has been a lot of progress and new ideas brought forth by the widespread use of PKP. However, this study has limitations. More research is needed to determine the effects of PMMA temperature and the concentration and dosage of lidocaine used for intravertebral injection on analgesic efficacy. In conclusion, an intravertebral injection of lidocaine during PKP can successfully minimize intraoperative pain, improve the surgical experience of patients and increase their confidence in surgery without changing the clinical impact of surgery.
Ethics statement
The present study was approved by the ethics committee of The 967th Hospital of Joint Logistic Support Force of PLA (PLA210-GC2017-008). The study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
Funding
The study was supported by the Science and Technology Project of Liaoning Province (2019-ZD-1080) and Dalian Medical Science Research Program (1712052).
Author contributions
Conception and design of the research: Chang XH, Wang JS, Yin JS. Acquisition of data: Zhao XM, Yin JS, Yan H, Liu J. Analysis and interpretation of the data: Yin JS, Zhang YZ, Wang JS. Statistical analysis: Chang XH, Yin JS. Obtaining financing: Chang XH, Wang JS. Writing of the manuscript: Yin JS. Critical revision of the manuscript for intellectual content: Chang XH, Wang JS. All authors read and approved the final draft.
Footnotes
Acknowledgments
The authors would like to acknowledge the hard and dedicated work of all staff that implemented the intervention and evaluation components of the study.
Conflict of interest
The authors declare that they have no competing interests.