
Abstract
BACKGROUND:
Although millions of people with osteoarthritis (OA) have altered biomechanical alignment, movement, and knee joint pain during gait, there are no effective and sustainable interventions. To mitigate such impairments, we developed an untacted self-automated robotic and electromyography (EMG)-augmented upper-trunk-lower reciprocal locomotor training (SRGT) intervention.
OBJECTIVE:
To compare the effects of SRGT and conventional treadmill gait training (CTGT) on the medial knee joint space width (JSW), hip adduction moment (HAM), knee varus deformity, pain, and physical function in community-dwelling older adults with OA.
METHODS:
Older adults diagnosed with medial compartment knee OA (5 men, 35 women; mean age
RESULTS:
Analysis of covariance (ANCOVA) showed that SRGT ed to greater changes in medial knee JSW (
CONCLUSION:
This study provides the first evidence for the long-term clinical and biomechanical effects of SRGT on JSW, knee joint kinematics, kinetics, and WOMAC scores in older adults with OA. Most importantly, self-automatic robotic gait training may be an alternative, effective, and sustainable treatment for the upper-trunk-lower reciprocal locomotor training in older adults with OA.
Introduction
Knee osteoarthritis (OA) is common and characterized by genu varum deformity, medial joint space narrowing, altered gait kinematics (excessive joint varus angle), altered gait kinetics (decreased hip adduction moment), joint pain, and imbalanced muscle activation. Specifically, patients with OA demonstrated: a 1.0
Accumulative evidence suggests that robotic-assisted gait training (RAGT) in older adults with altered gait biomechanics after neurological impairments (e.g., stroke and spinal cord injury) showed promising improvements in EMG muscle control (10%), kinematics angle (10%), and kinetic force (5%) during gait [13, 14, 15]. However, extensive review of the current literature showed no previous clinical research that examined the effects of robotic gait training on clinical and biomechanical changes in older adults with OA.
We have recently developed an untacted self-automated and EMG-augmented robotic upper-trunk-lower reciprocal locomotor training system (SRGT, WalkRite, Yu Gwang Precision, Daegu, Republic of Korea) based on the “bottom-up inverted pendulum or inverse kinematic model” used in other end-effector robot-assisted gait systems (Fig. 1), such as the G-EO (Reha Technologies, Olten, Switzerland) and Morning walk (Curexo, Seoul, Republic of Korea) [16, 17]. In essence, the SRGT system is designed to help users independently achieve efficient, pain-free, and biomechanically aligned walking during upper-trunk-lower reciprocal locomotor training while integrating real-time EMG feedback regarding the correct muscle activation pattern with an ample number of repetitions (1500 steps/session). The control computer activates the actuator using empirical biomechanical stepping gait analysis data to improve the timing symmetry of each leg flexion and extension, reciprocally synchronizing them with trunk-upper limb movements.
Self-automated and EMG-augmented robotic upper-trunk-lower reciprocal locomotor training system.
Despite the potential clinical and therapeutic advantages of SRGT in older adults with knee OA, these benefits have not been investigated in previous studies. Therefore, the purpose of this study was to compare the effects of SRGT and conventional treadmill gait training (CTGT) on the knee joint space, hip adduction moment (HAM), knee varus angle (VA), pain, and physical function in older adults with OA. Our primary hypothesis was that the knee joint space, HAM, deformity, pain, and functional activities would be different between the SRGT and CTGT groups.
Study design
Forty community-dwelling older adults with OA (35 women; mean age
Precepts of the consort.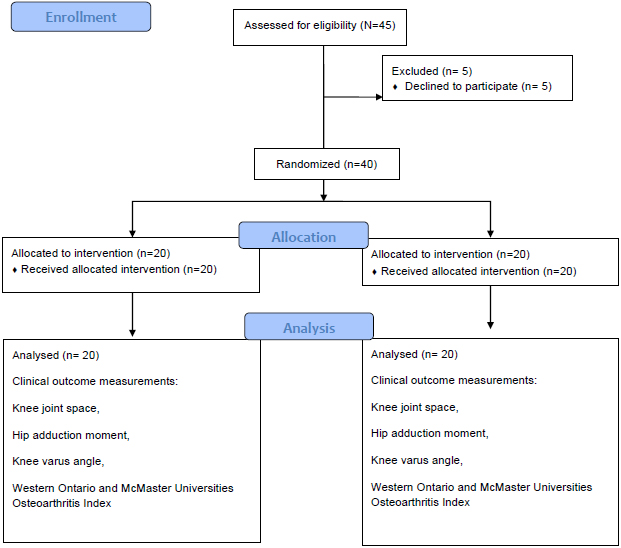
The inclusion criteria were: (1) age 55–85 years; (2) ability to walk upstairs and for 30 min in a reciprocal manner; (3) no history of knee surgical interventions for either of the lower limbs; (4) no previous robotic interventions for ambulation training; (5) knee pain while performing normal daily activities, such as walking, squatting, or kneeling; (6) mild to moderate knee OA (radiographic measurement of Kellgren and Lawrence grades II or III) in one or both knees; (7) medial compartment knee OA diagnosed by a physician; and (8) knee pain with numeric pain rating scale
The study used a randomized, single-blinded experimental design in which the participants were randomly assigned to either the control or experimental group using a random allocation sequence method. To reduce or eliminate experimental biases associated with participants’ expectations, experimental information that may affect the participants was masked until after the experiment. Randomization allocation was conducted by guiding according to the precepts of the consort (Fig. 2). Since BMI can also affect the results of the intervention, group assignment was performed using a matched-pair design to ensure matching for BMI and sex [18]. The pre-and post-tests included clinical tests (WOMAC), radiographic measurement of medial/lateral knee-joint space, and biomechanical measurements (kinematics and kinetics) of the more involved (painful) limb.
REX-525RF X-ray System (Listem, Incheon, Republic of Korea) was used to measure the medial/lateral knee joint space according to standardized radiographic methods [19]. Each participant was positioned on the table in supine position, with both lower extremities in neutral extension and without any rotation. An anteroposterior image was obtained from a standard projection to assess the knee joint, distal femur, proximal tibia and fibula, and patella as the beam was in the superior-inferior direction. The detector was kept distal to the knee [19]. A software analysis system (PacsPlusCV, Medicalstandard Co., Ltd., Republic of Korea) was used by a certified radiographer to determine the minimum JSW. The minimum JSW was quantified by visually determining the location of the minimum distance while viewing the film. In healthy older adults, the JSW is approximately 4.5 mm [20]. The test-retest reliability of the radiographic measurements was excellent (
Biomechanical measurements (kinematics and kinetics)
A 3D motion VICON analysis system with six infrared cameras (VICON MX system, Oxford Metrics, Oxford, UK) and two synchronized force plates (AMTI-OR6-7-7200 model, Advanced Mechanical Technology Inc., Watertown, MA, USA) was used to provide the knee joint kinematics (valgus and varus angle) and kinetics (HAM) during the self-selected walking speed. Passive reflective markers were attached to the skin according to the standard Plug-In-Gait marker set. Kinematic and kinetic data were then acquired at 120 Hz as the older adults with knee OA walked barefoot on a 7-m elevated walkway [21]. The participants performed a static position for calibration purposes, followed by gait familiarization, then walking (1 m/s), fast and walking (1.5 m/s) for 30 s (3600 frames). The raw dataset contained the data with marker errors and dropout directly streamed from Vicon; this was used in conjunction with Vicon Virtual System software to recreate the same real-time conditions in the laboratory, including marker reconstruction and auto-labeling steps.
Kinetic and kinematic data were analyzed using Nexus software (version 1.8; Oxford Metrics Groups, UK). The ground reaction force (GRF) and lever arm values were normalized to body weight (BW) and height (% ht). The HAM values were normalized % BW
Within the real-time code, the methods for reading input data, such as marker trajectories and ground reaction forces, have also been modified to operate on single time frames available in memory buffers. The normalized HAM values of the more involved limbs were averaged across three trials for further statistical analysis.
Clinical test
WOMAC is a standardized measurement of pain and physical function in OA that examines joint pain, stiffness, and physical function (e.g., rising from sitting and taking off socks). The WOMAC questionnaire comprises 24 items divided into 3 subscales, and scoring for each item ranges from 0 (none) to 4 (extreme). The reliability (intraclass correlation coefficient, 0.80–0.98) and validity (
Radiographic imaging data with and without the load gait training. EMG, electromyography.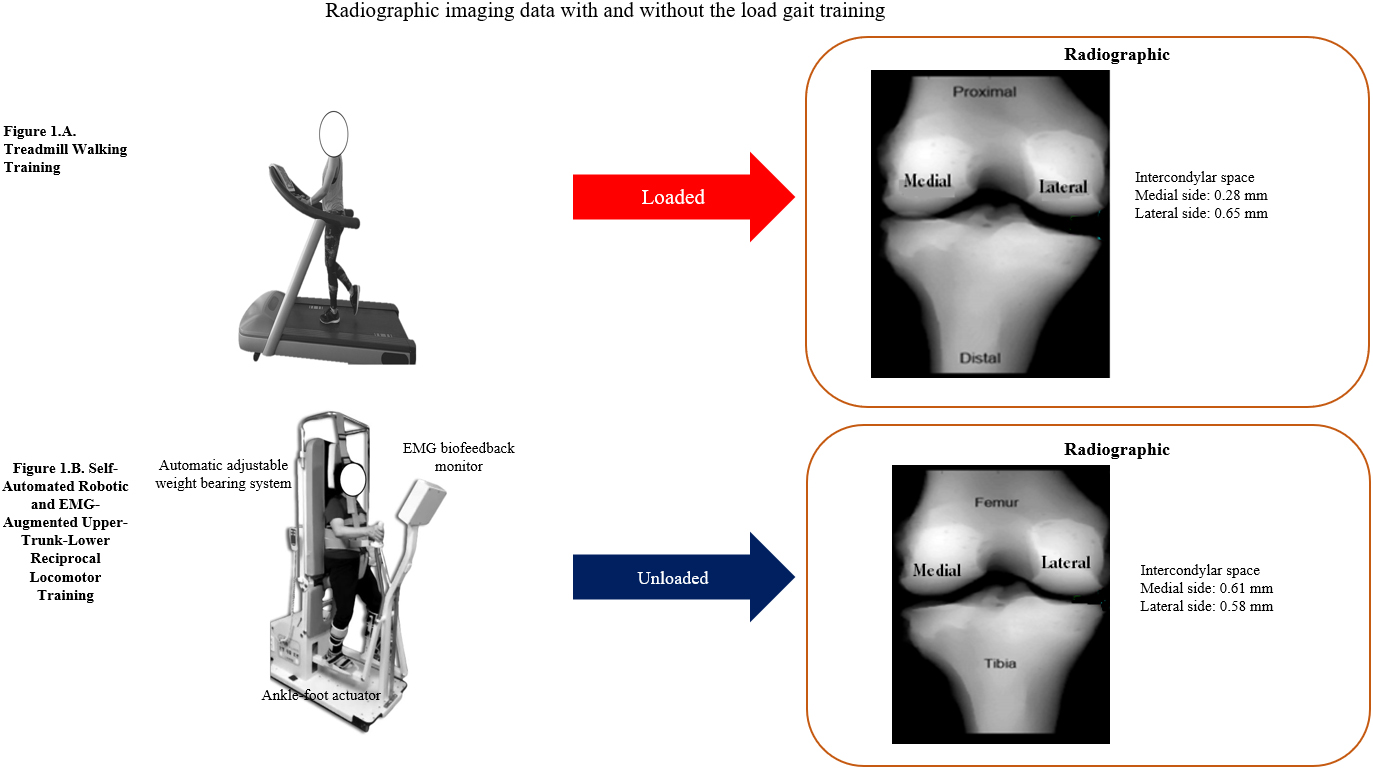
All participants were randomly assigned to either the standardized SRGT or CTGT intervention. Each session lasted 30 min (excluding set-up) and was conducted 3 times per week for 4 weeks. Resting time was provided when necessary; however, the treatment time lasted for at least 30 min. The SRGT protocol involved a combination of robotic gait training and EMG biofeedback (first week). The SRGT system enabled accurate robotic kinematic guidance force, while real-time EMG feedback helped restore the muscle balance ratio between the VMO and VL (1:1) for optimal gait [24]. The SRGT body weight support (BWS) was initially set at 70% and gradually decreased until the knee started to collapse into flexion during the stance phase. A physical therapist monitored the knee condition and controlled the BWS throughout the sessions. The walking speed was initially set at 1.0 km/h and gradually increased by 2.0 km/h. To the best of our knowledge, unlike current exoskeletal and wearable RAGTs including Lokomat (Hocoma AG, Volketswil, Switzerland) and Ekso health (Ekso bionics, Richmond, CA, USA), the best advantage of the SRGT is that it is relatively inexpensive, portable, easily utilized or affordable at any home setting, which generates most natural upper-trunk-lower reciprocal locomotor pattern. The control computer activates the actuator using empirical biomechanical stepping gait analysis data to improve the timing symmetry of each leg flexion and extension, reciprocally synchronizing them with trunk-upper limb movements, The SRGT is equipped with gait speed adjustment, an automatic weight controller, and a specialized saddle-harness. These adjust to the body weight during locomotor training to minimize weight-induced knee joint pain. Additionally, the side-frame and strap help realign genu varus deformities to promote the correct stride for an easier walk.
Participants in the CTGT group underwent treadmill gait training without weight support, and a physical therapist provided verbal instructional feedback and manual guidance for correct walking on the treadmill. Verbal instructional feedback comprised information on corrective knee valgus or varus alignment during treadmill gait training. If this was insufficient, manual guidance regarding the deviated knee joint valgus or varus alignment was provided to maintain optimal knee joint alignment during the training. As with the SRGT, the treadmill speed was set at 1.0 km/h and progressively increased by 2.0 km/h (Fig. 3).
Statistical analyses
Descriptive statistics included the mean and standard deviation. The one-sample Kolmogorov-Smirnov test was used to ensure normal distribution of the measurement data. A power analysis using G-Power software (Franz Faul, Kiel, Germany) was conducted to assess the total sample size requirement (
Demographic and clinical characteristics of the participants (
40)
Demographic and clinical characteristics of the participants (
Mean
Comparison of the medial knee JSW between the SRGT and CTGT groups
Mean
Comparison of HAM between the SRGT and CTGT groups
Mean
Comparison of knee varus angle between the SRGT and CTGT groups
Mean
The demographic and clinical characteristics of the participants are shown in Table 1. All participants successfully completed the experimental tests and interventions. There were no significant differences in sex, age, height, weight, or body mass index (BMI) between the SRGT and CTGT groups (
Comparison of WOMAC scores between the SRGT and CTGT groups
Comparison of WOMAC scores between the SRGT and CTGT groups
Mean
Analysis of covariance (ANCOVA) showed significant difference in in the medial joint space width (JSW) between SRGT and after CTGT (
Biomechanical measurement data
ANCOVA showed significant difference in HAM and VA between CTGT and SRGT (
Clinical data
ANCOVA showed significant difference in the WOMAC score between CTGT and RGT (
Discussion
This study provides the first evidence highlighting the long-term clinical and biomechanical effects of robotic-assisted and EMG-augmented gait training on JSW, knee joint kinematics (VA), kinetics (HAM), and WOMAC scores (joint pain, stiffness, and physical function) in older adults with medial compartment OA. As hypothesized, SRGT showed more meaningful difference in the medial joint space, varus deformity angle, HAM stress, knee joint pain, stiffness, and physical mobility measures than CTGT. Most importantly, our novel findings provide promising evidence that robotic-assisted and EMG-augmented gait training can help community-dwelling older adults with OA restore biomechanical malalignment and address the associated pain and functional physical mobility. To date, no studies have shown the effects of robotic gait training on OA, which makes it difficult to compare our present data with previous findings.
Analysis of the radiological imaging data showed significant differences in the medial knee JSW between CTGT and SRGT (22%), indicating substantial improvement in the medial knee joint space. Specifically, the mean JSW substantially increased to a near-normal width (4.5 mm) [20] after 4 weeks of robotic training. This finding is consistent with a previous radiological imaging study, which demonstrated an improvement in the knee-joint space of 0.34 mm (8.27%) after 12 weeks of strength training in 45 patients with mild to severe OA [25]. Moreover, the joint space equality ratio revealed that an initially decentered pressure to the medial compartment of the joint surface (“medial compartment joint space narrowing”), as commonly observed in varus deformity, became more equally distributed after SRGT. This indicates remarkable mitigation of knee varus malalignment in OA. A possible underlying rationale for such joint space improvement may be related to the specialized built-in mechanical traction system with counterweight suspension and movement guidance control via EMG augmentation. This design reduces and restrains the body weight load imposed on the knee joint, thereby increasing the joint space and improving arthrokinematic movement and pain. Furthermore, SRGT helped correct the altered knee joint alignment and movement during gait training. This was accomplished through the accurate robotic kinematic guidance force with real-time EMG feedback, which enriched the proprioceptive inputs to restore muscle balance, joint kinetics, and joint kinematics for optimal gait [26, 27].
Biomechanical data analysis demonstrated significance difference in HAM and varus angle between CTGT and SRGT (24.8%), suggesting that SRGT was more effective than CTGT in controlling excessive knee joint adduction moment stress and associated varus deformity. In particular, the knee adduction moment was significantly decreased by 25% after SRGT, and the resulting values were close to normal (2.8–3.0) [28], whereas no substantial changes were observed after CTGT (6%). These are in line with the kinetic findings of Shull et al. in 2013, which showed a 17% decrease in knee adduction moment after 6 weeks of treadmill gait training in older adults with moderate to severe OA [29]. Additionally, the 25% reduction in the HAM observed in the current study was greater than that reported in previous studies for lateral wedge insoles (9%) and valgus braces (6%) [30, 31]. Concomitantly, the reduced HAM or stress contributed substantially to a 20% decrease in the kinematic varus angle. This, in turn, improved varus deformity and the peak hip flexion angle and increased the medial joint space. A significant correlation was previously found between HAM and JSW (
Clinical data showed significance difference in WOMAC between CTGT and SRGT (15.49%), indicating meaningful clinical effects on pain, stiffness, and associated physical mobility. These findings are compatible with previous clinical data, which showed significant improvements in WOMAC scores after the upper-trunk-lower reciprocal locomotor training in adults with mild to moderate OA [36, 37, 38]. It is conceivable that excessive weight load reduction or redistribution during robotic-induced upper-trunk-lower reciprocal locomotor training reduced the mechanical stress imposed on an impaired joint surface and irritation underpinning joint pain and inflammation in OA.
This clinical RCT has a couple of research limitations that should be addressed in future studies. One limitation is that the radiographic images were obtained in an unloaded sitting position, as radiographic measurement does not permit scanning under the loaded position. The knee-joint space may be different in a loaded standing position, and one may argue that such unloaded radiographs may affect both the altered knee varus angulation and significance of the radiographic findings. Therefore, we used the relative change data from the baseline in both individual treatments. The other limitation is that this study did not measure the knee joint proprioceptive deafferentation, which is known to be an important pathophysiologic marker for the progression of OA. SRGT-induced restoration of the knee joint proprioception should be assessed in future studies. Nevertheless, our findings make an important contribution to the body of knowledge on effective and sustainable robotic treatment for older adults with OA, as well as to global health for older adults with OA during the pandemic period.
Conclusions
This clinical research study demonstrated that SRGT is more effective than CTGT at improving hip adduction kinetics, knee kinematics, pain and physical function in participants with knee OA. The present results provide clinical evidence-based insights into the utilization of SRGT, to maximize recovery of kinetics, kinematics, pain as well as physical function of OA rehabilitation in participants with knee OA.
Ethical approval
The study was approved by the Yonsei University Wonju Institutional Review Board (1041849-201712-BM-145-02) and Clinical Research Information Service (clinical trial number: KCT0003605).
Funding
This work was supported, in part, by the “Brain Korea 21 FOUR Project”, the National Research Foundation of Korea (Award number: F21SH8303039) and the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. 2021R1A2C101342312) to the Department of Physical Therapy, Graduate School, Yonsei University.
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No.RS-2023-00221762).
Informed consent
All participants signed an informed consent form.
Author contributions
Conceptualization and design: Y.C., H.Y., C. P., S.H.Y.; Data collection: Y.C., C. P., S.H.Y.; Interpretation: Y.C., H.Y., C. P., S.H.Y.; Writing-original draft: Y.C., H.Y., C. P., S.H.Y.; All authors read and approved the final manuscript.
Footnotes
Acknowledgments
None to report.
Conflict of interest
None to report.