
Abstract
BACKGROUND:
Hemiplegic shoulder pain (HSP) is a common morbidity of stroke. Different treatment modalities can be used for optimizing the results and limiting the possible side effects. This research compares the effects of two therapies used to reduce the pain and improve the quality of life of the patients with HSP.
OBJECTIVE:
This study aimed to compare the effects of transcutaneous electrical nerve stimulation (TENS) and suprascapular nerve blockage (SSNB) in patients with HSP.
METHODS:
In this clinical research, 24 patients with HSP who participated in a conventional rehabilitation program were randomized into TENS or SSNB treatment groups. A 100 mm visual analogue scale was used to assess the severity of pain. Passive range of motion (ROM) of the shoulder was measured. The Modified Ashworth Scale (MAS) was used to evaluate spasticity of the upper extremities, and the Modified Barthel Scale was used to assess activities of daily living (ADL). Quality of life was measured using the Stroke-specific Quality of Life (SS-QoL) questionnaire.
RESULTS:
The pain scores of the SSNB group decreased more significantly (
CONCLUSION:
TENS and SSNB were beneficial in relieving pain and increasing passive shoulder ROM and ADL in all patients. The alleviating of pain was faster in patients who underwent SSNB.
Introduction
Stroke is one of the leading causes of disability worldwide. Various complications are seen in hemiplegia due to stroke. Hemiplegic shoulder pain (HSP) is one such complication, with an incidence of 30–70% [1, 2]. HSP is a very common disorder and has various mechanical and neurogenic causes [3, 4, 5]. Mechanical causes include injuries to the surrounding tissues, motor loss, and muscle tone changes due to misalignment in the shoulder. In addition, neurogenic factors such as central pain, spasticity, or loss of sensation, also play a role in HSP [5].
The rehabilitation team plays a role in protecting the hemiplegic upper limb. Proper positioning of the upper extremities is required in hemiplegic patients. Despite training the patients’ families in this situation, HSP can develop very frequently. HSP causes deterioration in functional status and reduces quality of life; therefore, its treatment is important. The first-line treatment for HSP is usually via conservative methods [3]. Proper positioning of the upper limb, the use of shoulder braces while standing, physiotherapy, and exercises are beneficial treatments for HSP. Medications to reduce inflammation such as NSAIDs and other analgesics can help to alleviate the pain. Transcutaneus electrical nerve stimulation (TENS) is a commonly used treatment for painful conditions in clinical practice. TENS is thought to be beneficial for pain control in patients with HSP [6].
Intra-articular steroid injections or steroid injections into the subacromial bursa may also be helpful for pain control. Considering that 70% of the shoulder’s sensation is provided by the suprascapular nerve [7], suprascapular nerve block (SSNB) has been found to be beneficial in chronic shoulder pain and in patients with HSP [8, 9].
Nevertheless, in the literature there are conservative options for treating shoulder pain and these options are supported by the evidences. Although various treatment methods are used to control pain in patients with HSP, information on the clinical outcomes of these treatments is limited [10]. The treatment of HSP is based on a multidisciplinary approach, which aims to use different therapies optimizing the results and limiting the possible side effects [11].
Rehabilitation and physiotherapy are not always sufficient to achieve satisfactory pain relief. Pain may lead to decrease in shoulder range of motion (ROM), activities of daily living (ADL), and quality of life (Qol) in patients. The primary aim of this study is to compare the effects of TENS and SSNB on HSP. Secondly, we aimed to investigate the effects of these two treatment modalities on shoulder ROM, ADL, and Qol in patients with HSP.
Methods
Design
This comparative research study was conducted in our stroke rehabilitation unit.
Participants
The inclusion criteria for the study were an age of at least 18 years, a stroke duration
Interventions
Patients were randomized into 2 treatment groups, TENS (
Outcome measures
The patients were evaluated with the following outcome measures at the beginning of the study, at the first week of treatment, and at the end of the third week.
Visual Analogue Scale (VAS): A 100 mm VAS was used to assess the severity of pain. Shoulder ROM: Passive abduction, flexion, and external rotation ROM of the shoulder were measured with a goniometer. The modified Ashworth scale (MAS): MAS was used to evaluate spasticity around the shoulder adductor and elbow. MAS has been applied in clinical practice and research as a measure of spasticity. The modified Ashworth scale purpose is to grade muscle spasticity. MAS is evaluated between 1–5. A scale of 1 indicates no resistance and five indicates rigidity [11]. Modified Barthel scale: A modified Barthel scale was used to assess the activities of daily living (ADL). Modified Barthel scale is used to assess physical independence in activities of daily living. (Assesses the patient’s independence in mobility and personal care in ten items.) It consists of ten items (nutrition, bathing, self-care, dressing, bowel care, bladder care, toilet use, transfer, ambulation or wheelchair use, and stair climbing) and each item are scored separately. The total score is between 0–100. The higher the score, the higher the patient’s level of independence [12]. Stroke-Specific Quality of Life Scale (SS-Qol): Quality of life was measured using the SS-QoL. The patients were evaluated at the beginning of the study, at the first week of treatment, and at the end of the third week. SS-Qol is a disease-specific quality of life scale and consists of 49 items that assess 12 domains: social role (5 items), mobility (6 items), energy (3 items), language (5 items), self-care (5 items), mood (5 items), personality (3 items), thinking (3 items), upper extremity function (5 items), family roles (3 items), vision (3 items), and work/productivity (3 items). The scores of these 12 domains are summed to obtain a total score of 49–245. Higher scores indicate a better quality of life [13].
In the descriptive statistics of the data, mean, standard deviation, median, lowest, highest, frequency, and ratio values were used. The distribution of variables was assessed using the Kolmogorov-Smirnov test. The independent sample
Results
The demographic and clinical characteristics of the study groups are summarized in Table 1. The ratio of female patients in the SSNB group and the ratio of male patients in the TENS group were significantly higher (
The demographic and clinical characteristics of the study groups
The demographic and clinical characteristics of the study groups
The difference in the follow-up parameters of the TENS and SSNB groups
The difference in the follow-up parameters of the TENS and SSNB groups.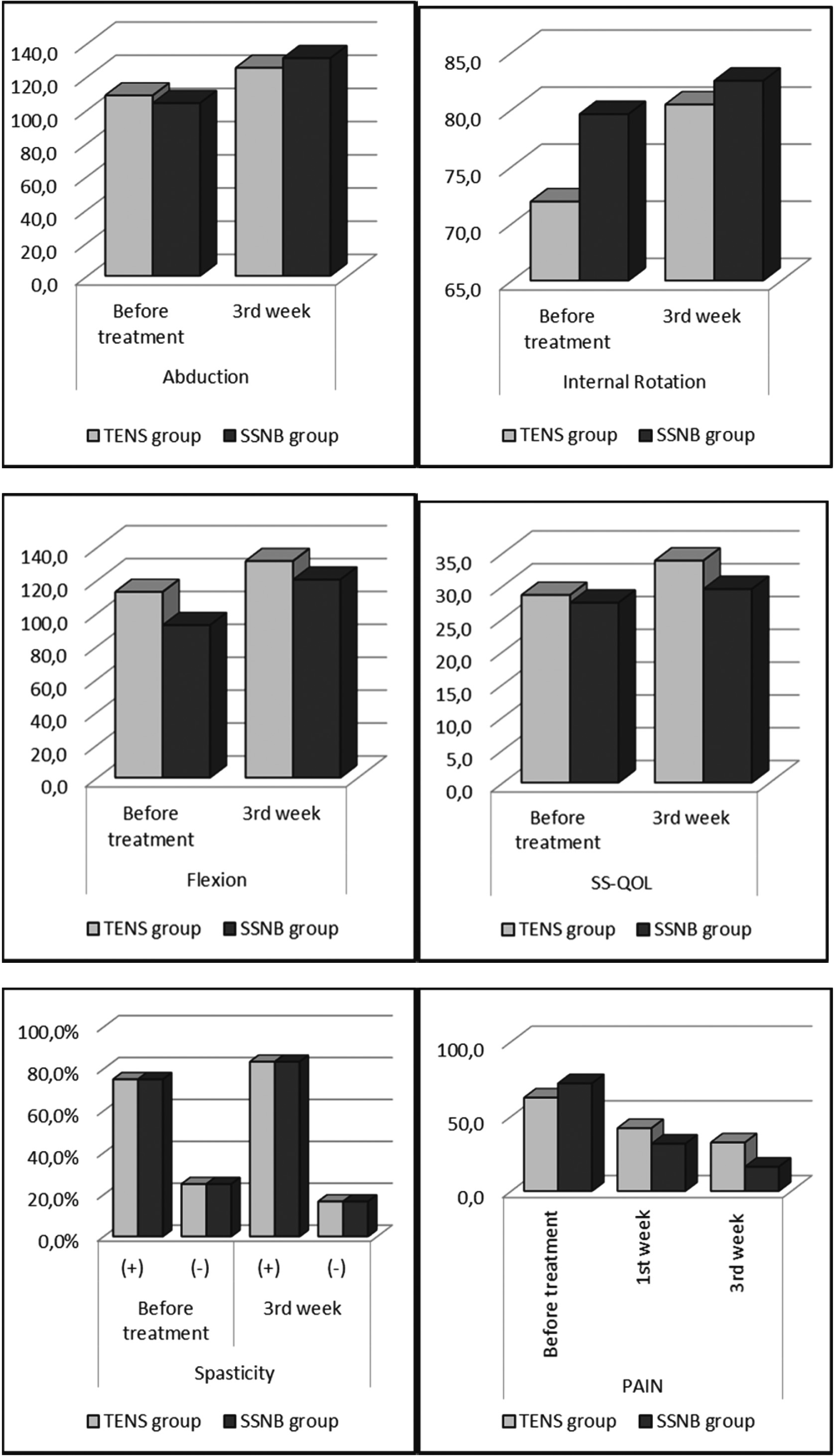
The differences in the follow-up parameters of the TENS and SSNB groups are shown in Table 2 and Fig. 1. In both groups, pain scores measured by VAS at the 1st and 3rd weeks showed a significant (
At week 3, the shoulder passive abduction and flexion ROM in both groups increased significantly (
The shoulder passive external rotation ROM increased significantly (
SS-QOL scores measured at the 3rd week in both groups were significantly higher than before treatment (
Spasticity scores as measured after treatment with the MAS and Modified Barthel Scores did not differ significantly compared to pre-treatment values in both groups (
HSP is associated with upper extremity weakness, right hemispheric lesions, sensory impairment, spasticity. It tends to begin in the subacute and chronic poststroke periods, and can be related to glenohumeral subluxation. Physical therapy with passive ROM exercises and prevention of shoulder injury are important to reduce the developing hemiplegic shoulder pain.
TENS is a physical therapy agent that stimulates small diameter, high threshold cutaneous afferents to block transmission of nociceptive information in peripheral nerves and activates extrasegmental analgesic mechanism. Although it is uncertain, TENS may help reducing most types of chronic pain and may be used as an adjunct to other more active treatments.
The suprascapular nerve is a mixed motor and sensory peripheral nerve. The nerve innervates shoulder muscles and sends sensory branches to the shoulder area. SSNB is a safe and effective method to treat pain in chronic pain of the shoulder.
In this study, both TENS and SSNB were found to be beneficial in terms of pain, shoulder ROM, daily living activities, and quality of life in patients with HSP. SSNB was better than TENS in terms of its rapid effects in reducing pain. Pain relief and improved ROM over a shorter period enable faster and more effective rehabilitation for HSP patients. This can lead to better functional results.
If there is increased muscle tone around the shoulder, antispasmodics and botulinum toxin injections could also be helpful for reducing the HSP. In the study by Mera et al. 30 subjects with post stroke spasticity were divided into two groups. One of the groups received botulinum toxin injection and physiotherapy while the other group received botulinum toxin injection, rESWT and physiotherapy. Assessments were performed before treatment and first, second and third months after treatment. Using MAS, VAS for pain and MyotonPro
In the study by Aydin et al., there was a more significant improvement in pain, shoulder ROM, and quality of life in the SSNB group at the 1st and 3rd months compared to those who only performed a home exercise program [15]. Moreover, in the SSNB group, there was an improvement in pain 1 week after the injection, and this situation continued for the 1st and 3rd months. Conversely, there was no improvement in pain in the home exercise group. In the same study, the quality of life as measured by EQ-5D also improved in the 1st week in the SSNB group. There was no difference between the baseline values in either group in shoulder spasticity, as measured by the MAS and Brunnstrom Motor Stages after treatment.
In a placebo-controlled study in patients with HSP conducted by Adey-Wakeling et al., the decrease in pain severity measured by VAS at the 1st and 4th weeks was greater in the SSNB group than in the control [16]. The same study also reported no differences between the groups in terms of disability and quality of life.
In a study conducted by Picelli et al. in stroke patients with chronic HSP with a stroke duration of
In a 4-week study by Boonsong et al., the efficacy of SSNB and ultrasound were compared in patients with HSP. The reduction in shoulder pain was faster in the SSNB group than in the ultrasound group [18], but there were no differences between the groups in terms of shoulder ROM. No complications were reported during the treatment.
Farì et al. investigated the efficacy of radiofrequency in treating various musculoskeletal pain.They reported that radiofrequency was more effective in reducing pain than control treatments in adhesive capsulitis. In our study we used SSNB instead of radiofrequency for treating the HSP to reduce the pain [19].
In a study in patients with HSP by Ekim et al., TENS application for 20 minutes, 5 days a week, for a total of 15 sessions, was superior to placebo in terms of pain and improvement in ADL, as assessed by the Barthel Index [6]. In another placebo-controlled study by Leandri et al. involving 60 patients with HSP, the patients were divided into 3 groups and received a total of 12 sessions of TENS over 4 weeks. At the end of the treatment and 1 month later, high-intensity TENS increased the passive flexion, abduction, and extension openings of the shoulder, but there was no significant effect in the low-intensity TENS group [20]. In this study, because of its better tolerability, the TENS intensity was adjusted to be within the limits of the pain threshold. In a previous study conducted on patients with chronic pain, there was no difference in pain between different TENS applications [21]. TENS applied at the pain threshold has been found to be useful in the treatment of acute and chronic painful conditions [22].
Kim and Chang compared the effectiveness of pulsed radiofrequency stimulation of the suprascapular nerve with intra-articular corticosteroid injection for chronic hemiplegic shoulder pain following stroke. This study included 20 patients with hemiplegic shoulder pain after stroke, randomly assigned to the pulsed radiofrequency and intra-articular corticosteroid injection treatment groups (
In our study, in both groups, pain scores measured by VAS at the 1st and 3rd weeks showed a significant decrease when compared to the pre-treatment period. The decrease in pain scores in the SSNB group was significantly higher than in the TENS group at both the 1st and 3rd weeks when compared to the pre-treatment group. The reduction in shoulder pain was faster in the SSNB group than in the TENS group. Spasticity scores as measured after treatment with the MAS and Modified Barthel Scores did not differ significantly compared to pre-treatment values in both groups.
In our study, no complications were observed in either group. Both TENS and SSNB were found to be safe. One patient in the TENS group diagnosed with COVID-19 was excluded from the study. All remaining patients completed 15 sessions of TENS treatment.
This study has strengths and some limitations. Its strength is that, to the best of our knowledge, this is the first study comparing TENS and SSNB in the treatment of HSP. SSNB can be used as an additional treatment when conventional treatments are insufficient in pain control in HSP. Its limitations are that the sample size was relatively small, the follow-up period was relatively short, and there was no long-term follow-up. Another limitation is that the person making the evaluations was not blinded to the treatments.
Conclusion
Both TENS and SSNB have been deemed beneficial in relieving pain and increasing passive shoulder ROM and ADL in patients with HSP. It was observed that pain control was achieved more quickly with SSNB in the first week. Although, the clinical trials with big sample sizes are needed, SSNB is advantageous to enable the patients to participate in rehabilitation programs actively in a short time.
Ethical approval
The study was performed in accordance with the Declaration of Helsinki and was approved by the Bakırköy Dr Sadi Konuk Research and Training Hospital Ethics Committee (Approval number 2020-25-04). Written informed consent was obtained from all subjects.
Funding
This study was not supported by any foundation.
Author contributions
All authors contributed to the study conception and design. All authors read and approved the final manuscript.
Footnotes
Acknowledgments
The authors are grateful to the patients and hospital staff who contributed to this study, Istatistik Akademisi for analyzing the data and Scribendi for proofreading and editing.
Conflict of interest
The authors do not have commercial or other associations that might pose a conflict of interest.