
Abstract
BACKGROUND:
The population of older adults with knee osteoarthritis (OA)-related disabilities is increasing globally. However, studies regarding instrumental activities of daily living (IADL) in older adults with knee OA are limited.
OBJECTIVE:
This study investigated the psychological factors associated with IADL disability in older adults with moderate to severe knee OA.
METHODS:
A cross-sectional study was conducted on 179 patients with knee OA aged
RESULTS:
Of the 179 participants, 88 (49.1%) showed disability in conducting IADL. PSEQ-4 (odds ratio
CONCLUSION:
Even after controlling for cofounders, our study found that self-efficacy, assessed using the PSEQ-4, was related to IADL disability in older adults with moderate to severe knee OA.
Introduction
Knee osteoarthritis (OA) is a prevalent age-related chronic condition and a common cause of disabilities limiting daily activities in older adults [1]. Since the population of older adults with knee OA-related disabilities is increasing globally [2], healthcare professionals need effective countermeasures to address this concern.
Instrumental activities of daily living (IADL) are essential elements in the independent lives of older adults. It is defined as independent functioning in a given environment and includes activities such as meal preparation, shopping, commutation, financial management, and performance of other household chores [3]. Meanwhile, basic activities of daily living (BADL) include basic self-care activities such as bathing, dressing, eating, and other indoor activities [4]. IADL require more complex functioning than BADL. As IADL disability in older adults influences health-related quality of life [5], all-cause mortality [6], and decline of cognitive function [7], assessments and interventions for IADL disability are important for this population
Disabilities in patients with knee OA are affected by factors such as gait speed, knee muscle strength, and pain [8, 9]. Psychological factors, such as pain catastrophizing [10, 11, 12], self-efficacy [12, 13, 14] and depressive symptoms [14, 15, 16] have also been reported among disabled patients with knee OA. A meta-analysis has shown the importance of psychological intervention for disability in patients with knee OA [17].
However, most studies of psychological factors and disability among patients with knee OA [10, 11, 12, 13, 14, 15, 16] have treated disability as a concept that combines BADL and IADL. It is well known that disabilities in older adults progress hierarchically [18]; IADL disability occurs before BADL disability [19]. Especially among older adults with knee OA, countermeasures should be taken at an early stage to prevent an incident or deterioration of disabilities. In particular, older adults with moderate to severe knee OA are more likely to develop disabilities in their daily lives than healthy older adults [20]. Therefore, investigating specific factors related to IADL disability in older adults with moderate to severe knee OA is useful information to develop effective interventions. To our knowledge, there are limited studies of IADL disability among older adults with knee OA [16, 21]; only our previous study has specified that gait speed and pain intensity are related to IADL disability in older adults with knee OA [22]. Psychological interventions are recommended for such disabilities [17]; however, which specific psychological factors are associated with IADL disability remain unclear. Factors such as demographics [23], motor function [22, 24, 25, 26], and pain intensity [22, 27] have been shown to influence IADL disability in older adults. Additionally, most studies of psychological factors and disability among patients with knee OA [10, 11, 12, 13, 14, 15, 16] found associations between psychological factors and disability by including motor function and pain status as confounders. Some psychological factors, such as self-efficacy, are affected by physical function and pain intensity [28]; therefore, these factors must be considered as confounders when attempting to establish an association between psychological factors with IADL disability.
This study aimed to determine the psychological factors associated with IADL disability in older adults with moderate to severe knee OA. We hypothesized that psychological factors such as pain catastrophizing, self-efficacy, and depressive symptoms are independently associated with IADL disability, even when adjusted for demographics, motor function, and pain intensity as confounders.
Materials and methods
Study design
This study used a cross-sectional design, and its conducting and reporting were guided by the STROBE guidelines [29]. Sample recruitment was conducted at Shonan Kamakura General Hospital from May 17, 2019 to May 30, 2021. All participants provided informed consent before the study began. The study was conducted in accordance with the Declaration of Helsinki and was approved by the research ethics boards of the Tokushukai Group Ethics Committee (No. TGE01198-024).
Participants
Patients with knee OA scheduled for primary unilateral total knee arthroplasty (TKA) or unicompartmental knee arthroplasty (UKA) were eligible for this study. The inclusion criteria were those aged
Procedures
All participants were given a two- to three-month waiting period after deciding to undergo TKA or UKA. On the day participants decided to undergo TKA or UKA, well-trained physical therapists taught them self-exercises to do during waiting periods. Self-exercises were designed to improve knee muscle tightness and strength based on individual knee conditions (e.g., muscle strength and range of motion [ROM] exercises). All physical function measurements, such as gait speed, were performed by well-trained physical therapists, and participants completed the self-administered questionnaires one month before the surgery.
Outcome measures
IADL status
IADL status was assessed on six activity items (preparing food, shopping, housekeeping, doing laundry, using transportation, and handling finances), referencing the IADL scale proposed by Lawton and Brody [3]. Taking medication and using a telephone were excluded, as it was expected that the condition of knee OA would not affect these items. Participants were asked to rate their abilities to perform these IADL activities by “able,” “need help,” or “unable.” Based on previous cross-sectional reports [24, 27], we defined those participants who opted for “need help” or “unable” to perform for at least one item as “disabled”; otherwise, they were defined as “non-disabled.”
Psychological factors
Pain catastrophizing, self-efficacy, and depressive symptoms were assessed as psychological factors based on previous reports that discussed the relationship between disability and psychological factors in patients with knee OA, as they show strong relation to disability even when adjusted for other confounders such as demographic factors and pain intensity [10, 11, 12, 13, 14, 15, 16].
Pain catastrophizing was assessed using the Japanese version of the six-item short form of the Pain Catastrophizing Scale (PCS-6) [31]. The Pain Catastrophizing Scale consists of subscales related to magnification, rumination, and helplessness [32]. PCS-6 has the same properties as the original version, correlates to pain intensity assessed by numerical rating scales (
Self-efficacy was assessed using the Japanese version of four-item short form of the Pain Self-Efficacy Questionnaire (PSEQ-4) [34]. The Pain Self-Efficacy Questionnaire is a 10-item self-report questionnaire used to assess self-efficacy in individuals with chronic pain [35]. The PSEQ-4 has the same properties as the original version [34], correlates pain intensity assessed by numerical rating scales (
Depressive symptoms were assessed using the Japanese version of the fifteen-item Geriatric Depression Scale (GDS-15) [36]. The GDS-15 can screen depression (area under the curve of the receiver characteristic operating curve
Confounders
We assessed gait speed and pain intensity as confounders for outcome measures, referring to previous studies that report factors related to IADL disability in older adults [22, 24, 25, 26]. Knee muscle strength and joint ROM were also assessed as confounders, since they are considered specific factors related to disability in patients with knee OA [37]. Based on previous studies regarding IADL disability and gait speed [22, 24, 25, 26], usual gait speed (UGS) was measured using a 5-meter gait test [38]. If participants use a cane on a daily basis, we permitted using it during measurement.
The Japanese version of the pain subscale of the Knee injury and Osteoarthritis Outcome Score (KOOS-pain) was used for the representative index of pain intensity [39]. The KOOS-pain consists of nine questions. Participants were asked about their condition one week before the evaluation date. Standardized answer choices were provided, and each question was assigned a score ranging from 0 to 4. A normalized total score of 0 to 100 was calculated, and higher scores indicated that patients reported less pain. A score of
Isometric knee extension strength (IKES) was measured using a handheld dynamometer (
Statistical analysis
The participants were divided into two groups according to their IADL status: those who answered “need help” or “unable” to perform on at least one item were assigned to the IADL disabled group, and those who answered “able” in all items were assigned to the IADL non-disabled group. All outcome measures and confounders were compared between the two groups. The chi-square test was used for categorical variables, and Student’s
Which psychological factor can be associated with IADL disability was determined using a binary logistic regression model with IADL status as the dependent variable (disabled
To determine the sample size for the logistic regression analysis, the number of cases (N)
Results
Of 357 patients, 166 were excluded due to a history of TKA or UKA on the other knee (
Participant flowchart. BADL 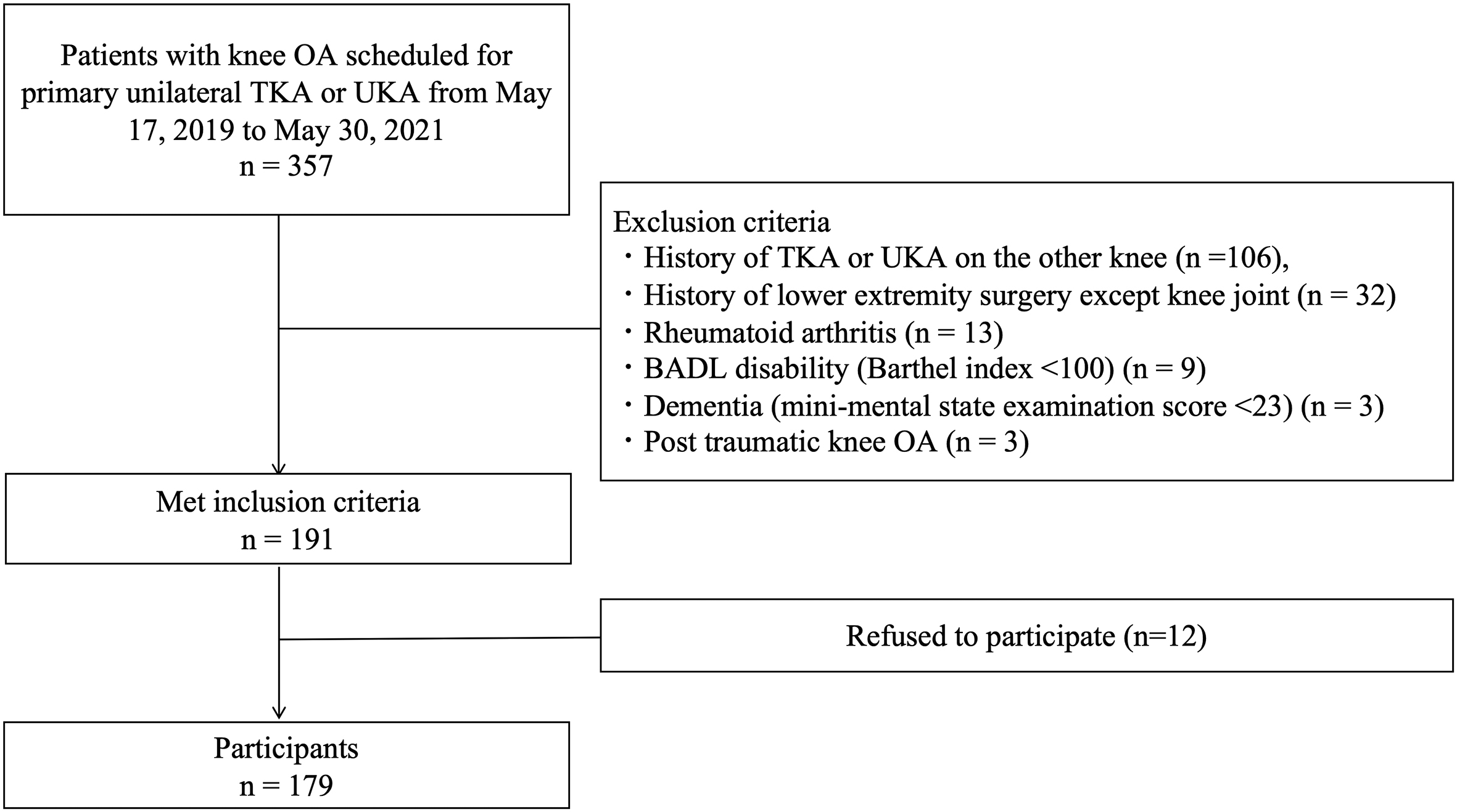
All participants completed all assessments, and all confounders were collected from their medical records. Participants’ characteristics are presented in Table 1. Of all participants, 88 (49.1%) had IADL disabilities. Sixty-one (69.3%) showed disability in shopping and 47 (53.4%) showed disability in using transportation (Table 2).
Baseline characteristics of the study population
CCI
Content of IADL disability in IADL disabled group (
IADL
The IADL non-disabled group was significantly younger (
Comparison of measurements and confounders between IADL non-disabled and disabled groups
Effect size was estimated using
In the binary logistic regression analysis with IADL disability status as a dependent variable, IKES on the unaffected side was adopted as a confounder. IKES on both sides showed significant differences between the two groups, but the effect size on the unaffected side was greater than that on the affected side. Therefore, only IKES on the unaffected side was included to avoid multicollinearity. In Models 1–3, PCS-6, PSEQ-4, and GDS-15 were significantly independent variables. In Model 4, PSEQ-4 (odds ratio [OR]
Logistic regression model with the dependent variable as IADL disabled or not
The present study aimed to investigate the psychological factors associated with IADL disability in older adults with moderate to severe knee OA. The values of the PCS-6, PSEQ-4, and GDS-15 tools significantly differed between the IADL non-disabled and IADL disabled groups. However, in the logistic regression analysis, which included all of the selected psychological factors and confounders, self-efficacy, assessed using PSEQ-4, was identified as a significant psychological factor associated with IADL disability.
In the logistic regression model, sex and UGS were also significant independent variables. Alexandre et al. [23] have shown that sex is a factor associated with IADL disability in older adults. Our results support this finding. A reduction in gait speed is also strongly associated with IADL disability in older adults [24, 25, 26]. Our current findings are consistent with those of our previous study, which showed gait speed to be a discriminatory factor for IADL disability in older adults with knee OA [22]. In our study population, the main items pertaining to IADL disability were outdoor activities such as shopping (68.6%) and using transportation (50.6%), which require a degree of gait speed. Furthermore, because the effect size of UGS was the highest among all the measurements when compared between the two groups, it could be a crucial factor associated with IADL disability in older adults with moderate to severe knee OA.
Catastrophizing about pain has been linked to increased physical disability in patients with knee OA [45]. Somers et al. reported that pain catastrophizing explained a significant proportion of the variance in physical disability measures [11]. Depressive symptoms are also significant psychological issues in public health [46]. According to a recent systematic review and meta-analysis, 19.9% of people with OA had depressive symptoms [47]. A cohort study of functional decline in daily life in patients with arthritis over two years found that depressive symptoms were a significant risk factor for functional decline, even after controlling for physical function and demographic factors [16]. For patients with chronic pain, the fear-avoidance model, which explains the relationship between psychological factors and disability progression in daily life, has been proposed. In the model, pain catastrophizing and depressive symptoms have been shown to be some of the leading causes of disability [48], and should be considered when accounting for relationships between psychological factors and disability. Moreover, self-efficacy has also been reported a mediator in the relationship between pain intensity and disability [49]. Our results implied that pain catastrophizing and depressive symptoms could be factors associated with IADL disability. However, based on the results of our multivariate analysis, self-efficacy as assessed by the PSEQ-4 was the most important factor associated with IADL disability in older adults with moderate to severe knee OA.
With respect to the relationship between pain self-efficacy and disability in patients with knee OA, Sinikallio et al. [12] suggested that self-efficacy assessed using the Pain Self-Efficacy Questionnaire was the only psychological factor associated with disability in multiple regression analysis that included demographics as confounders. Some cross-sectional studies have shown that self-efficacy, which partially includes pain elements, is a factor related to disability in patients with knee OA [14, 15]. A cohort study of older adults with knee pain indicated that self-efficacy is a predictor of self-reported disability [13]. A new finding of our study is that self-efficacy assessed by PSEQ-4 was also a factor related to disability even if the disability in daily life was limited to IADL. Regarding IADL disability and self-efficacy, using a logistic regression analysis that included demographics and pain intensity as confounders, a previous cross-sectional study of older adults with chronic joint pain showed that self-efficacy is associated with IADL disability [27], which is consistent with our results. Self-efficacy describes the confidence that a person has in their ability to achieve a desired outcome [50]. In patients with knee OA, those with high self-efficacy for controlling arthritis pain have higher pain thresholds than those with low self-efficacy [51]. Therefore, older adults with knee OA who have high self-efficacy might be considered less likely to voluntarily restrict activities included in IADL even if they have knee pain. Consequently, we considered self-efficacy, assessed using the PSEQ-4, associated with IADL disability even after adjusting for other confounders.
This study has several limitations. First, since this was a cross-sectional study, causal relationships between psychological factors and IADL disability incidence could not be determined. Second, this study included patients with knee OA scheduled for TKA or UKA, who were in a different treatment situation compared with other older adults with knee OA. Therefore, it might be difficult to generalize the results to older adults with early-stage knee OA or in a low pain status. In particular, awaiting surgery could affect pain intensity and psychological factors related to pain. Nonetheless, the average KOOS-pain score in this study population was not inferior to those in other studies [52]. The median PCS-6 and PSEQ-4 scores were also not inferior to those in previous studies in patients with chronic pain [33, 34]. Therefore, effects of awaiting TKA or UKA to pain intensity and psychological status were small. Third, because IADL disability was assessed using categorical variables as the dependent variable in our logistic regression analyses, we could not identify the effect of each factor on IADL disability. However, when comparing the two groups, the effect sizes of the variables that were significantly related to IADL disability in logistic regression models were approximately the same.
As we excluded patients with BADL disability, as measured by the Barthel index, from our study population, no participants required assistance with BADL. Additionally, CCI revealed that only a few participants had moderate to severe comorbidity affecting BADL. However, many patients may struggle with long-distance walking or stair climbing due to pain or poor knee function. Hence, it was not surprising that 49.1% of all participants had IADL disability, which was defined as requiring assistance to perform IADL activities. Previous cohort studies have shown that even one IADL disability affected all-cause mortality [6] and the rate of cognitive function decline [7]. We believe that those with IADL disability in our study population are more likely to experience health problems in the near future and should be closely monitored. The purpose of this study was not to predict IADL disability using assessments; rather, it was conducted with the conviction that greater knowledge about psychological factors in older adults with knee OA will aid in understanding the risk of IADL disability or deterioration.
Conclusion
Regarding psychological factors, self-efficacy, assessed using the PSEQ-4, was associated with IADL disability even after adjusting for confounders. Sex and gait speed were also associated with IADL disability in older adults with moderate to severe knee OA. Our study demonstrated the importance of self-efficacy, assessed using the PSEQ-4, as the factor most associated with the presence of IADL disability in older adults with moderate to severe knee OA. Future studies are necessary to elucidate the mechanism through which self-efficacy is related to IADL disability in this population. Additionally, the sample size should be increased, and multivariate analysis should be performed using other factors that can affect IADL disability, such as living environment and educational level. Furthermore, longitudinal studies are needed to identify predictors of the development of IADL disability in older adults with moderate to severe knee OA.
Ethical approval
The study was approved by the research ethics boards of the Tokushukai Group Ethics Committee (No. TGE01198-024).
Funding
The authors report no funding.
Informed consent
All participants provided informed consent before the study began.
Author contributions
KN: Conceptualization, Methodology, Investigation, Formal analysis, Writing – original draft, Project administration. TI: Methodology, Writing – original draft. NN: Investigation, Writing – Review and Editing. TS: Methodology, Writing – Review and Editing. TJ: Methodology, Writing – Review and Editing, Supervision.
Footnotes
Acknowledgments
The authors thank D. Kurihara, K. Imahira, and K. Suda for their cooperation with data collection.
Conflict of interest
The authors declare that they have no conflict of interest.