
Abstract
BACKGROUND:
Blood flow restriction (BFR) training improves muscle strength and functional outcomes, but the proprioceptive implications of this technique in the rehabilitation field are still unknown.
OBJECTIVE:
The present study aimed at assessing the effects of BFR in terms of stabilometric and balance performance.
METHODS:
In this pilot randomized cross-over study, healthy young adults were included and randomly assigned to Groups A and B. Both groups underwent a postural assessment with and without wearing a BFR device. Study participants of Group A underwent postural baseline assessment wearing BFR and then removed BFR for further evaluations, whereas subjects in Group B performed the baseline assessment without BFR and then with BFR. Stabilometric and balance performance were assessed by the robotic platform Hunova, the Balance Error Scoring System (BESS), the self-reported perceived balance (7-point Likert scale), and discomfort self-rated assessment. Moreover, the safety profile was recorded.
RESULTS:
Fourteen subjects were included and randomly assigned to Group A (n: 7) and Group B (n: 7). Significant differences were shown in balance tests in static conditions performed on the Hunova robot platform in terms of average distance RMS (root-mean-square) with open eyes (OE), anteroposterior (AP) trunk oscillation range with OE, mediolateral (ML) average speed of oscillation with OE, and total excursion AP range with closed eyes (CE) (BFR: 3.44
CONCLUSION:
Taken together, our data showed that BFR affects balance performance of healthy subjects. Further studies are needed to better characterize the possible role of BFR treatment in the context of a specific rehabilitation protocol.
Introduction
In the last two decades, a growing literature has been focusing on the potential role of blood flow restriction (BFR) in several physical exercise and rehabilitative programs [1]. BFR is a training technique developed in the 1970s and based on partial arterial occlusion and total venous occlusion achieved through a pneumatic cuff or strap [2]. This technique might be effectively combined with physical exercises, promoting both neuro-muscular adaptations in an anoxic environment and increases in muscle strength and tropism [3, 4, 5]. BFR has been extensively studied in both healthy and post-injured subjects, especially in chronic painful conditions like knee osteoarthritis [6, 7]. Interestingly, growing literature suggests that the main advantage of this technique is the lower training load needed to achieve a hypertrophy response of muscle fibers, with relevant implications for the rehabilitation process of several musculoskeletal conditions [8, 9].
More in detail, the BFR training might improve neuro-muscular strength and hypertrophy in combination with low-intensity exercises (20–40% 1 repetition maximum test-1RM) and functional exercises [1, 10]. At present, the precise mechanisms underpinning these clinical effects still remain unclear. However, it has been proposed that the increase in metabolic stress might shift the recruitment of greater caliber motor units, which are not normally recruited during low-intensity activity [11]. On the other hand, it should be noted that BFR training might have positive effects on pain management, with recent reports suggesting that acute analgesic effects can occur after a single training session with BFR [12, 13, 14, 15]. However, since exercise-induced hypoalgesia can persist up to 24 hours after exercise, it has been hypothesized that pain reduction following BFR training may be related to the same possible mechanisms [13, 16]. In this scenario, the systematic review by Miller et al. [17]showed that BFR training might promote local adaptations at the level of the skeletal muscle system, but limited information is currently available about other systems.
In the rehabilitation field, neuromotor control training is considered a cornerstone of the therapeutic programs tailored for patients affected by motor function impairment. These interventions aim to improve physical performance and neuro-muscular recovery and prevent skeletal muscle injuries. Interestingly, it has been reported that changes in the proprioceptive and motor control functions might increase the prevention of skeletal muscle injuries and increase physical performance in athletes [18, 19]. Similarly, proprioceptive training might be effective in older adults to improve balance control and reduce the risk of falls [20]. Despite several different types of proprioceptive training reported in literature, the effects on proprioceptive outcomes still remain uncertain, probably due to the great heterogeneity of training methods [21].
In this context, posture is defined as the spatial position and orientation of the human body resulting from the neuromuscular activation of skeletal muscle system regulated by the central nervous system based on multisensory inputs [22]. Adequate spine posture is a crucial target of several rehabilitation interventions since optimal results allow for the best athletic gesture and prevention of different musculoskeletal disorders [23]. Although good posture might prevent chronic disabling conditions [24, 25], there is still a gap of knowledge about the optimal strategies affecting spinal posture [22, 26, 27].
The figure shows the Blood Flow Restriction device and the Hunova
Moreover, to the best of our knowledge, the effects of BFR on balance and spinal posture have not been widely explored yet, despite the positive results in terms of strength and muscle mass improvement [1, 10]. Moreover, it should be noted that the impact that BFR on proprioceptive system is still unknown and few studies assessed the effects of proprioceptive training wearing BFR [28].
Therefore, through this pilot randomized cross-over study, we aimed at assessing the effects of BFR on posture and balance and the safety profile in healthy young adults. This could have relevant implications providing clinically useful insights into this novel approach and its possible improvement in the rehabilitation field.
Participants
This study included a series of healthy subjects enrolled between July and December 2022. Inclusion criteria were: a) age between 18 and 40 years old; b) healthy status; c) signing in the informed consent. Exclusion criteria were: a) risk factors for thromboembolism; b) history of venous thrombosis and/or pulmonary embolism; c) risk factors for deep vein thrombosis; d) coagulopathy and/or risk factors for coagulopathies; e) history of peripheral arterial vascular disease or suspected arterial or venous insufficiency of the lower limbs; f) pulse wave velocity (PWV) above 10 m/s [29]; g) anemia; h) trauma to the lower limbs in the previous 30 days; i) physical impairment affecting testing procedures; l) dental surgery in the previous 30 days.
All subjects were assessed for eligibility by a multidisciplinary team composed of an expert physician specialized in physical and rehabilitation medicine and a physiotherapist with years of expertise in postural assessment.
This pilot randomized cross-over study was realized following the CONSORT guidelines [30]. The approval of the trial protocol was obtained from the Ethic Committee of the Azienda Ospedaliera Nazionale SS. Antonio e Biagio e Cesare Arrigo, Alessandria, Italy (ASO.RRF.22.01; protocol number 21982) and was performed in accordance with the Declaration of Helsinki [28] and pertinent national and international regulatory requirements. All researchers involved were instructed to protect the participants’ privacy, and all participants were asked to carefully read and sign an informed consent form and were allowed to revoke their consent to participate in the study without any limitation.
Intervention
All subjects assessed for eligibility and meeting the eligibility criteria were enrolled in this study. All subjects enrolled were randomly assigned to two groups (Group A or Group B) through a randomization scheme with a 1:1 allocation without blocks. Participants were blinded to group allocation during baseline testing (T0).
Group A. All subjects enrolled in Group A wore BFR devices (MAD-UP SAS, 49100 Angers, France) with the blood flow reduction cuffs applied between the proximal third of quadriceps femoris muscle and the inguinal fold. Figure 1 shows the BFR device used in this study. Pressure cuffs were applied by a physical therapist experienced in musculoskeletal disorders and the use of the BFR device. For calibration of the device, the subject lay supine and the pressure cuffs were applied to both limbs targeting the pressure of arterial partial occlusion. The calibration of the pressure was performed automatically by the device, by detecting the initial arterial pressure. The arterial partial occlusion has been subsequently verified by a doppler probe (linear transducer, 7.5–10 MHz, Cerbero, ATL, 20100 Milan, Italy) positioned on the posterior tibial artery. Once the machine has been calibrated, the cuff pressure was adjusted to 80% of occlusal pressure. During the assessments, the device automatically adjusted for blood pressure changes by selecting the program “Performance” in “Free mode” with a blood flow reduction time setting of 10 minutes. After baseline assessments (T1), the subjects removed the BFR device and undergone to the same assessments without BFR device.
Group B. Study participants performed all baseline assessments without wearing BFR. After the baseline assessment (T1), all study participants enrolled in Group B performed all stabilometric and balance assessments wearing BFR as previously described in Group A.
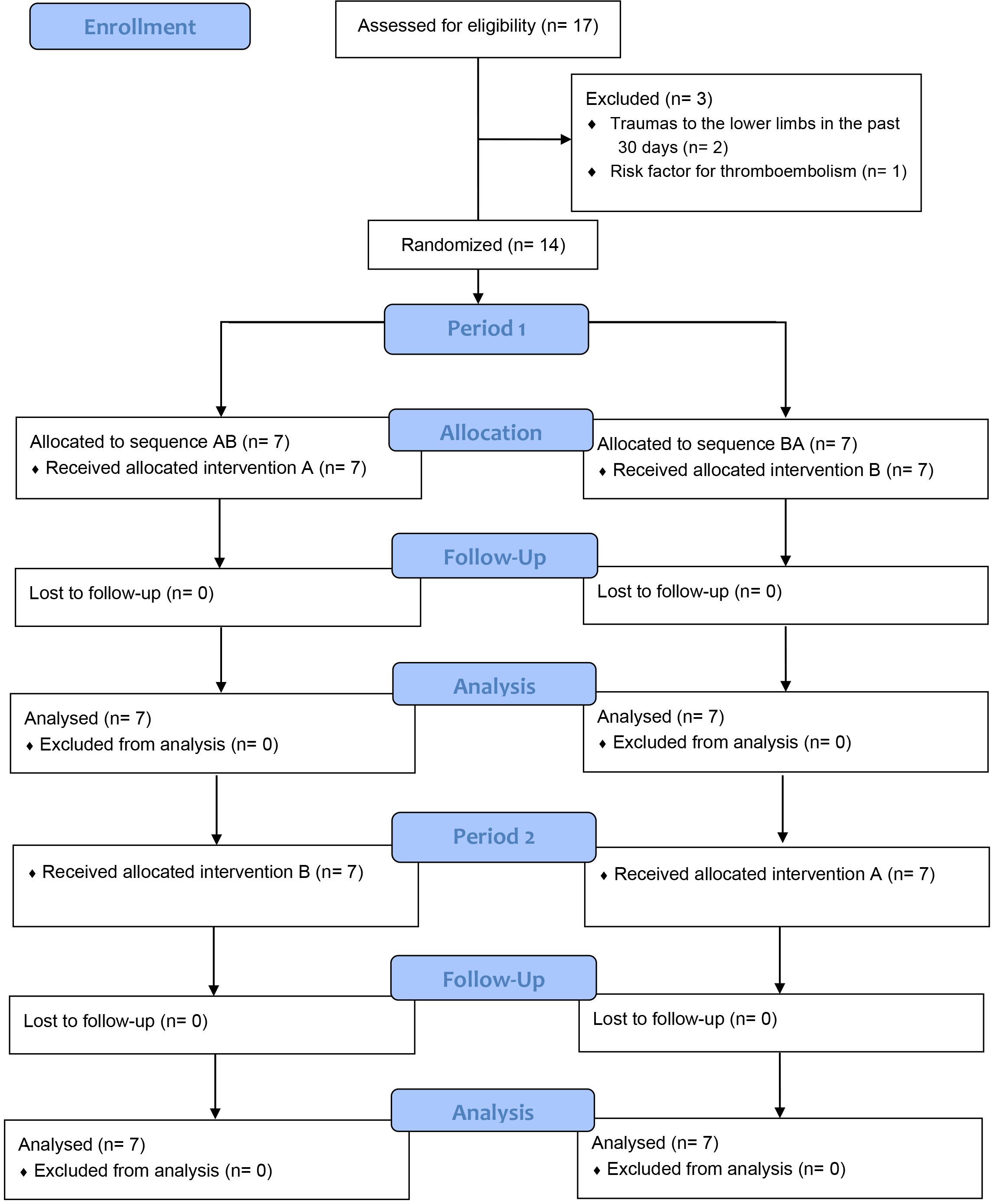
Further details about the study selection and randomization process are summarized in Fig. 2.
At the baseline assessment, sociodemographic and anthropometric data were collected. However, due to the intrinsic nature of the study intervention, blinding the operator during the data collection was not possible. Primary and secondary outcomes were assessed at each time point.
The robotic platform Hunova
Balance test in static conditions performed on the Hunova
Elastic balance test performed on the Hunova
Dynamic balance test performed on the Hunova
During the Hunova
Sway Area [cm
Average distance – RMS [cm]: The average distance, from the center, of the oscillations.
Sway Path [cm]: the length of the oscillation path of the CoP trajectory [33].
Romberg index: Relationship between the stabilometric values with CE and the corresponding values with OE.
A-P and M-L Range of oscillation [cm]: Oscillation of the CoP in static conditions or of the platform’s angular displacement projection in unstable dynamic conditions. These variables indicate the amount of oscillation in either the anterior-posterior or mediolateral directions and are related to the subject’s instability [33].
A-P and M-L Average speed of oscillation [cm/s]: the average speed of swing in the anteroposterior and mediolateral directions.
A-P and M-L Trunk oscillation range [deg]: Parameters that provide information on the compensatory and corrective trunk control strategies required to maintain optimal balance. They were calculated by comparing the maximum and minimum degrees of inclination of the roll (mediolateral range of oscillation, MLO) and pitch (anteroposterior range of oscillation, APO) angles. They are based on the trunk sensor signal (IMU sensor) [33].
Trunk movement [deg/s
Secondary outcomes were:
Balance Error Scoring System (BESS) score. BESS is a clinical tool for assessing balance and static postural control. The BESS includes three different tasks: double-leg stance, single-leg stance, and tandem stance. Errors are recorded throughout each 20-second trial as the subjects perform the stances with their CE on a firm surface and on a foam surface. Opening eyes, lifting hands off the hips, walking, stumbling, or falling out of position, lifting the forefoot or heel, abducting the hip by more than 30
Self-reported perceived balance through 7-point Likert scales: This is a qualitative balance assessment based on self-reported perceived balance based on 7 different items (ranging from “completely stable” to “not at all stable”). The rating was assigned based on the subjective perception of the subject’s own stability.
Rating of perceived exertion through Borg scale CR-10: This is a rating scale to assess self-perceived fatigue during the tests. Subjects were asked to give a score from 1 to 10 (1 represents “totally fatigued” and 10 “not at all fatigued”).
Discomfort in using the BFR through Numerical Rating Scale (NRS): Subjects were asked to verbally evaluate their discomfort on a scale from 0 to 10 (with 0 equal to “totally comfortable” and 10 equal to “total discomfort”) [35].
Safety: Any adverse events that occurred during the tests.
Each session was supervised by the same physiotherapist with a therapist/patient rate of 1:1. All data were analyzed by the same personnel blinded to the treatment performed.
Due to the pilot design of the study, the sample size was not calculated. However, in line with recent recommendations for pilot studies [36], we targeted a sample size of at least 12 study participants.
All data were analyzed using GraphPad Prism 7.0 (GraphPad Software, Inc., San Diego, CA, USA). The non-Gaussian distribution of the outcome variables was assumed due to the low sample size. The Shapiro-Wilk statistic was used to confirm the non-Gaussian distribution of variables. Categorical variables were reported as numbers and ratios, while continuous variables were represented as means
Results
Out of 17 subjects assessed for eligibility, 14 young adults met the eligibility criteria and were randomly assigned to Group A (n: 7; mean age: 28.0
In particular, the subjects in group A were aged 28.0
Significant intra-group differences were reported in Group A in balance test performed in static conditions on the Hunova
Clinical outcome measures assessed in the two groups
Clinical outcome measures assessed in the two groups
Continuous variables are expressed as means
In contrast, the intra-group statistical analysis in Group B showed significant effects in balance test in static conditions on the Hunova
Results of the pooled analysis for the outcome measures
Continuous variables are expressed as means
The between-groups analysis compared showed significant differences (
The assessment in the elastic balance test performed on the Hunova
Lastly, there were no significant differences in the outcome measures assessed with dynamic balance test on the Hunova
All subjects included showed no side effects. The discomfort during the BFR test was registered by NRS scale, showing a mean of 3.08
In recent years, BFR has been introduced in the rehabilitation management of different chronic disabling conditions to reduce pain intensity, weight load, and improving anabolic changes in trained muscles [1]. Despite several reports focused on the positive impact of BFR training in terms of muscle strength and functional performance [37, 38, 39], the effects on balance performance and spinal posture have not been characterized yet.
In light of this consideration, this pilot randomized crossover study aimed at assessing the postural changes induced by BFR device, in order to provide clinically relevant evidence about the effects on neuromuscular control during rehabilitation wearing BFR.
Interestingly, our results showed that BFR might affect balance performance in both static and dynamic conditions. More in detail, our results showed that BFR might interact with AP average distance, AP trunk oscillation range, and ML average speed of oscillation in static conditions with OE. Interestingly, the recent study by Burkhardt et al. [28] assessed the effects of BFR on muscle activation during dynamic balance exercises. The authors reported that wearing BFR might affect the activation of vastus lateralis and soleus muscles and significant effects of BFR were reported in terms of perceived postural instability [28]. However, there are no previous studies assessing the effects of BFR in terms of static balance performance, elastic balance performance, and dynamic balance performance. On the other hand, dynamic balance exercise combined with BFR might be an option to potentially improve benefits of proprioceptive training, especially considering the increasing evidence suggesting that BFR might be most beneficial combined with low-intensity muscle training [40]. In this context, dynamic balance training is commonly performed with low-intensity muscle contraction (20–40% 1RM) and might take potential advantages of BFR integration without adjusting exercise intensity.
Moreover, it was interesting to notice that our data underlined significant differences in Romberg index during elastic balance test on the Hunova
Therefore, BFR might affect the muscle response due to the limitation of oxygen delivery resulting in different expressions of muscle force in proprioceptive training [46, 47]. In contrast, growing literature is now suggesting that BFR might affect peripheral sensation during exercise training, reducing pain intensity [48, 49]. Despite the antinociceptive role of BFR has not been fully characterized, BFR might affect the afferent signal of pain sensation by an anaerobic environment. In this context, hypoxic conditions might modulate pain intensity through a noxious conditioning stimulation mechanism. More in detail, an ascending painful input from a distant body area (or conditioning stimulus) reduces the perception of another painful input from other sites of the body. As result, BFR could be considered a conditioning stimulation modulating ascending inputs of pain sensation [50].
On the other hand, BFR might affect not only pain sensation but also other multisensory peripheral inputs with previous reports reporting secondary effects of BFR training including paraesthesia [48]. Interestingly, these sensitive peripheral alterations might include proprioceptive inputs in accordance with the significant results found in terms of Romberg index during elastic test on the Hunova
Although BFR might affect balance performance, the subjects included did not report differences in terms of subjective balance perceived (with BFR: 5.73
To the best of our knowledge, this is the first study combining robotic rehabilitation technology with BFR. In recent years, growing attention is rising on digital innovation and robotic rehabilitation for several disabling disorders [53, 54, 55]. In this scenario, several studies have assessed stabilometric performance with Hunova
However, we are aware that this study is not free from limitations. Firstly, the small sample size severely limits the strength of our findings. On the other hand, it should be noted that, according to the pilot design, we targeted a specific sample size following the most recent recommendations for pilot studies [36]. In addition, compared with a parallel group design, less participants are required for a cross-over study to obtain the same power for a target effect size according to the CONSORT statement [58].
Moreover, healthy subjects might be characterized by a high endocrine system with potential implications of these results in terms of applicability for pathological subjects. However, were considered healthy subjects in accordance with the phase I trial recommendations of the US Food and Drug [59] since no previous study assessed the neurophysiological implications of BFR in balance control in humans.
In this context, PWV, which represents an independent risk factor for cardiovascular accidents, was assessed as inclusion criteria, but it was not assessed at T1. PWV reflects arterial stiffness, and an increase of 1.0 m/s in PWV leads to a 12–14% increased risk of cardiovascular events [60]; it is known that strength training increases in healthy young people the arterial stiffness [60], but it is not known if BFR training may induce a greater risk. A recent systematic review on low-intensity resistance exercise with moderate BFR reported that BFR applied to the lower limbs may induce positive effects related to arterial stiffness, although a degree of caution has been suggested in order to prevent unwanted responses in arterial stiffness markers [61].
Another major limitation is that the study participants did not perform specific training to the BFR device and Hunova
Lastly, a superficial electromyography assessment might further characterize the neuromuscular control impairment from a physiological perspective. Despite these considerations, it has been already assessed in literature the effect of BFR on muscle activation outcomes [28, 62], although no previous study assessed balance performance with objective stabilometric assessment during BFR training.
Conclusions
In this pilot cross-over study, we assessed the effects of BFR on balance performance and safety profile in healthy adults randomly assigned to two groups. Taken together, our findings suggested a potential positive effect of BFR in static and elastic balance performance on the Hunova
Funding
This study is part of the project NODES which received funding from the MUR – M4C2 1.5 of PNRR (grant agreement no. ECS00000036).
Ethics statement
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethic Committee of the Azienda Ospedaliera Nazionale SS. Antonio e Biagio e Cesare Arrigo, Alessandria, Italy (ASO.RRF.22.01; protocol number: 21982). Informed consent was obtained from all individual participants included in the study.
Footnotes
Acknowledgments
The authors would like to thank Stefano Moalli and Giulia Stacchino for their support of this work.
Conflict of interest
None to report.