
Abstract
BACKGROUND:
Adolescent idiopathic scoliosis (AIS) is the most common structural deformity of the spine during adolescence, which could cause varying degrees of physical and mental damage to patients. Schroth therapy and sling exercise are widely used in the treatment of patients with AIS currently, and have shown the significant therapeutic effect relatively.
OBJECTIVE:
To observe the efficacy of sling exercise combined with Schroth therapy on adolescents with mild idiopathic scoliosis (MIS).
METHODS:
Sixty patients with AIS were randomly divided into the Schroth
RESULTS:
After the treatment, Cobb angle, ATR in both groups were decreased compared with those before (
CONCLUSION:
Schroth therapy improved the degree of scoliosis, torticollis, quality of life, and bilateral paraspinal strength on adolescents with mild idiopathic scoliosis. The effect was more pronounced when the sling exercise was included in the treatment regimens.
Introduction
Adolescent idiopathic scoliosis (AIS) is the most common structural deformity of the spine during adolescence, the cause of which is unknown, and its incidence rate is about 2
Sling exercise refers to the hanging part or the entire body in the air through a rope, ring or other equipment, in order to achieve the purpose of training. Sling exercise has recently become one of the common training methods for musculoskeletal diseases [12, 13, 14]. It is a therapeutic method to restore functional motor patterns through high-level neuromuscular stimulation [15]. A number of studies have shown that sling exercise can improve the strength and endurance of subjects’ core muscles [16, 17]. Weng et al. [18] found that core stabilization training can significantly reduce the Cobb angle and improve the posture of AIS patients. However, as the representative of core stabilization training, little attention has been paid to the effect of sling exercise on AIS patients.
This study attempts to increase sling exercise on the basis of Schroth therapy and observe whether the two can play a synergistic effect, so as to better improve the posture, function and quality of life of adolescents with mild idiopathic scoliosis (MIS).
Materials and methods
Subjects and sample size calculation
G*Power was applied to calculate the sample size. The minimum sample size for each group was 53 at a statistic power of 0.95 referred to the previous research, an alpha level of 0.05 and an effect size of 0.45. Considering the dropout rate of 10.34% in the previous research, the minimum sample size in this study was 62 [19].
This study was conducted in accordance with the Declaration of Helsinki and the protocol was approved by the Ethics Committee of Suzhou Science & Technology Town Hospital (No. IRB202103001RI). A total of 64 AIS patients treated at Suzhou Science and Technology City Hospital met the diagnostic criteria of idiopathic scoliosis established by the International Scoliosis Rehabilitation Association [3]. All patients and their families fully understood the purpose and content of the study, and agreed to participate and signed the consent form before starting the intervention.
Inclusion criteria: 1) Cobb angle
Exclusion criteria: 1) Patients with spinal tumor, tuberculosis, fracture, spinal cord injury, ankylosing spondylitis, rheumatoid arthritis, osteoporosis, lumbar spinal stenosis, spondylolisthesis and so on; 2) Patients with severe cardiopulmonary diseases, exercise contraindications or after spinal surgery; 3) Secondary or degenerative scoliosis.
Study design
The method of randomized controlled trial was used. A total of 64 patients with AIS were numbered according to the order of their visits and divided into the Schroth
The Schroth group was given Schroth therapy [10]. The exercises included: 1) Physiologic balance training: Patients can improve the sagittal physiological curvature of the spine through it. 2) Daily activity posture training: patients use corrective posture such as “Muscle-cylinder” exercise under the sitting posture and the standing posture in daily life, lowering the left or right hip to make the spine in a neutral position, so as to reduce the asymmetrical force on the vertebral body and intervertebral disc. 3) Three-dimensional correction training: patients should take the initiative to raise and lower the hip to correct the pelvis, while translating the chest toward the concave side of the thoracic segment, also they were supposed to sink and adduct the convex side of the thoracic segment to stabilize the scapular area, and inhale the air into the concave side of the chest at the same time. Bilateral muscles of the spine contracted and maintained the movement when exhaling, 50 breaths as a group [10]. The above methods were trained three times a week for 90 minutes for four weeks [22].
The Schroth
After 4 weeks of exercise, 8 weeks of home exercise should be completed under the supervision of parents. The only exercise program was Schroth therapy. Each time of exercise was conducted for 60 minutes, 3 times a week for 8 weeks. After each exercise, parents would confirm that the exercise has been completed in the WeChat group with their mobile phones.
Outcome measurements
The baseline of the subjects in both groups were recorded at the first visit.
Primary outcomes measures
Cobb angle
The X-ray film of the whole spine in the standing position of the patient was taken, and the maximum curved arc on the coronal plane was selected to determine the upper and lower end of the maximum curved arc, and the angle between the parallel line of the upper edge of the vertebral body and the lower parallel line of the lower end of the vertebral body was measured. The final value of Cobb angle was the average value of the two measurements. Cobb angle measurement is the most reliable method of monitoring the progress of scoliosis [23].
Surface electromyogram (sEMG)
The surface electromyography analysis system(model: ULTIUM) produced by Noraxon Company in the United States was used to test the bilateral paraspinal muscles and select the glute bridge as test action. The electrode was placed at the 2 cm adjacent to the spinous process of the vertebra at the top of the largest curved arc, the two electrodes are separated by 2 cm along the muscle fibers, and the left and right sides of the spine are symmetrical [24]. Action requirements: Patients are supposed to stay in the supine position, make their hips and knees flexed and lift their buttocks off the ground until the torso, pelvis and thighs are in a straight line, while maintaining the highest point for 30 s. The sEMG signal of paraspinal muscle was recorded when the maximum voluntary contractile force was measured. The sampling frequency was 1 kHz, the noise level was less than 1
Secondary outcomes measures
Angle of trunk rotation (ATR)
The ATR was evaluated by Scoliometer and Adam’s forward flexion test. The subjects relaxed, stood with their feet together, looked forward, put their hands together, slowly bent forward to their knees, placed the Scoliometer directly above the spinous process, and read the ATR [26].
Scoliosis Research Society-22 (SRS-22)
The SRS-22 scale evaluated the patients from five dimensions: Function, Pain, Posture, Mental health and Treatment satisfaction. There were 22 items in the questionnaire, with a score from 1 (worst) to 5 (best) and a total score of 110, and each dimension takes its average. Because all the patients participated in the treatment for the first time, the treatment satisfaction was not listed as the evaluation item in this trial, and the final score was the average of the four dimensions. The higher the total score, the higher the quality of life of the patients [27].
The flow of patients.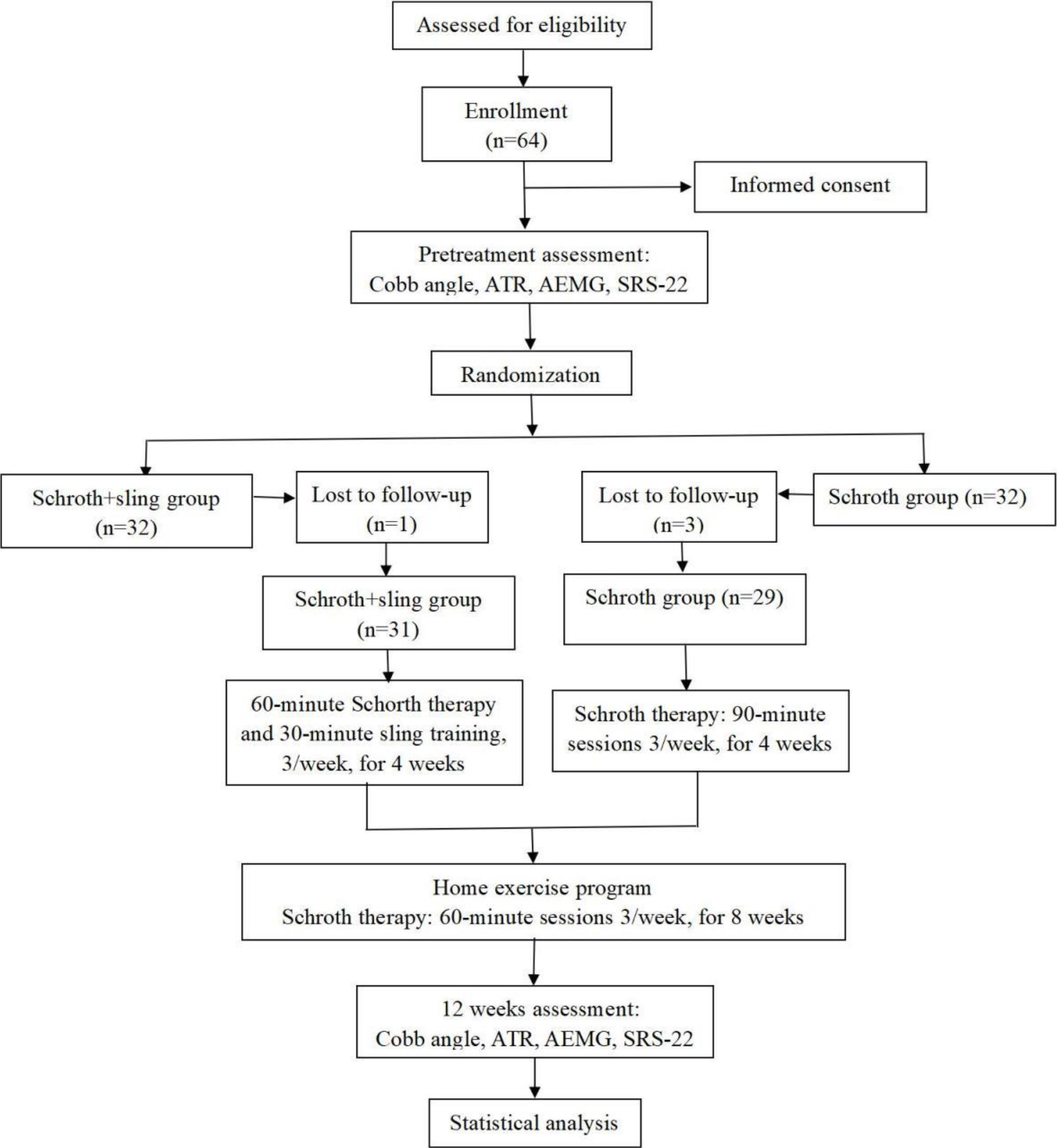
Statistical analyses were performed with SPSS version 23.0 statistical software. The inter-group comparison of counting data was conducted by Chi-square test. The measurement data were expressed in terms of (M
Results
A total of 64 AIS patients met the inclusion criteria. Four subjects were excluded because they did not complete the evaluation or treatment. Eventually, 60 patients were included in the study: Schroth
Baseline characteristics of the subjects
Baseline characteristics of the subjects
BMI: Body Mass Index; SD: Standard deviation. There were no statistical differences among the groups (
Baseline values of outcome measurements
SD: Standard deviation. There were no statistical differences among the groups (
Cobb angle
The results of repeated measurement analysis of variance of Cobb angle show that the main effect of measurement times was significant (
The result of repeated-measures analysis of variance of Cobb angle, AEMG, ATR and SRS-22 scores
The result of repeated-measures analysis of variance of Cobb angle, AEMG, ATR and SRS-22 scores
AEMG: Average Electromyogram; SRS-22: Scoliosis Research Society-22; SD: Standard deviation;
The Comparsion of Cobb angle, AEMG, ATR and SRS-22 scores between the groups
AEMG: Average Electromyogram; SRS-22: Scoliosis Research Society-22; SD: Standard deviation;
After 12 weeks of treatment, the Cobb angle of the two groups was improved in both groups, and the improvement in the Schroth
The results of repeated measurement analysis of variance of Convex side show that the main effect of measurement times was significant (
The results of repeated measurement analysis of variance of Concave side show that the main effect of measurement times was significant (
After 12 weeks of treatment, the AEMG of bilateral paraspinal muscles in the two groups was significantly improved than that before (
ATR
The results of repeated measurement analysis of variance of ATR show that the main effect of measurement times was significant (
After the treatment, there was an improvement in both groups in the ATR group (
SRS-22
The results of repeated measurement analysis of variance of SRS show that the main effect measurement times was all significant (
After the treatment, the scores of posture, mental health and total score in the Schroth
Discussion
Adolescence is the stage with the greatest risk of scoliosis progression [28]. Without early intervention, patients may have problems such as pain, appearance deformities and decreased paraspinal muscle strength [4, 29, 30]. Therefore, scientific intervention should be made timely and effectively for patients with mild AIS [3, 31]. Modi et al. [32] discovered the mechanism of spinal balance and self-adjustment. The stability of the spine requires the participation of the core muscle group. When the core muscle group is out of balance, the spine cannot maintain stability and scoliosis forms. On the contrary, if the core and spine are stable, scoliosis will improve accordingly. This study assumes that combining sling exercise with Schroth therapy can improve the related symptoms of AIS patients, which is confirmed in this study.
Sling exercise is one of the important ways to increase core stability. Closed-chain exercise mode is used to reconstruct the feed-forward mechanism of the body, stimulate nerves and muscles, help to activate spinal core muscles, and increase core stability and trunk control ability [33]. Patients with AIS are often accompanied with paraspinal muscle atrophy, decreased strength and even back pain, while long-term disuse or pain makes the stable muscles of the body core “shut down”, resulting in a decline in exercise quality and neuromuscular system control, and eventually a decline in the quality of life. Even if the pain or muscle disuse is temporarily relieved, the function of the core stabilizer continues to “shut down” and may cause pain or muscle disuse to worsen again, falling into a vicious circle. The core of sling exercise is to activate dormant or inactivated muscles. The exercise program is changed in the central nervous system, so through neuromuscular training, muscles may change from dormant state to activated state after injury, so as to restore its normal function.
After 12 weeks of treatment, the Cobb angle, ATR, SRS-22 and paraspinal muscle strength of the two groups were improved, especially in the Schroth
Stoke et al. [38] proved Hueter-Volkman ’s law that increasing vertebral pressure can reduce its growth rate, and reducing vertebral pressure can promote its growth. In patients with AIS, the pressure on the concave side of the vertebral body is large and the growth rate is slow, while the pressure on the convex side is small and the growth rate is fast [38]. Schroth therapy may increase the epiphyseal pressure of the convex side of the vertebral body, reduce the pressure of the concave side of the vertebral body and promote its growth by translating the concave torso and raising the convex side of the pelvis at the same time [10]. In this study, the improvement of Cobb angle in both groups may be related to it. The key point of Schroth therapy is to rotate angular breathing, that is, to increase the breathing of the concave part of the trunk, tighten the muscles of the convex part of the body, reduce the excessive expansion of the lungs on the convex side, and each angular breathing contributes to the correction of the horizontal plane of scoliosis [39], which may be related to the improvement of ATR in both groups of patients in this study. Noh et al. [40] found that Schroth therapy combined with core training can effectively improve the Cobb angle, ATR and SRS-22 posture of patients with AIS. Kuru et al. [41] randomly divided 45 patients with AIS into the Schroth group, home exercise group and control group (without any treatment). It was found that Cobb angle, ATR and waist symmetry were improved in the Schroth group, while those in control group were worsened. Aktan et al. [42] observed 45 AIS patients and found that the subjects’ ATR, posture, trunk muscle endurance and dynamic balance were improved after 7 days of Schroth intensive training. Short-term intensive Schroth training can improve the related symptoms of AIS patients, but teenagers are in the stage of growth and development, scoliosis is easy to worsen, correction is a long-term process, and the hospital treatment time is short, therefore, AIS patients need to efficiently complete the homework told by the therapist to ensure the curative effect.
To sum up, sling exercise combined with Schroth therapy can play a synergistic effect and more effectively improve the posture and quality of life of patients with mild AIS. The limitations of this study are insufficient sample size, difficulty in home exercise supervision and quality assurance, errors in Cobb angle measurement, and the only selection of paraspinal muscle in core muscle group evaluation and inability to rule out cross-talk in collecting EMG data. Whether sling exercise combined with Schroth therapy is equally effective in patients with moderate or severe AIS needs further study. In addition, this study needs further objective and quantitative evaluation methods such as gait analysis system, cardiopulmonary function and so on, to further explore the therapeutic effect and mechanism.
Conclusion
After 12 weeks of treatment, Schroth therapy improved the degree of scoliosis, torticollis, quality of life, and bilateral paraspinal strength on adolescents with MIS. Furthermore, the effect was more pronounced when the sling exercise was included in the treatment regimens. In future clinical practice, sling exercise should be considered in treatment for adolescents with MIS to achieve greater effectiveness and improve patients’ quality of life.
Author contributions
PZ: Methodology and Writing – Original Draft. XS: Formal analysis and Writing – Review & Editing. LZ: Investigation and Writing – Review & Editing. SW: Validation and Supervision. QW: Validation and Project administration.
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article or its supplementary materials.
Ethical approval
The study was approved by the Ethics Committee of Suzhou Science & Technology Town Hospital (No. IRB202103001RI).
Funding
The project was supported by Suzhou Science and Technology Association (2021kphd-07).
Informed consent
Written informed consent was obtained prior to the start of the intervention.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors declare that they have no conflict of interest.