
Abstract
BACKGROUND:
Hip osteoarthritis (OA) is a chronic progressive disease that impresses a noticeable burden to society and healthcare systems. Physical exercise constitutes the first-line hip OA treatment approach, nevertheless, there is currently no gold standard method to treat this disease.
OBJECTIVE:
To evaluate the efficacy of proprioceptive neuromuscular facilitation (PNF) on functioning in patients with hip OA.
METHOD:
A pilot randomized controlled trial (RCT) was carried out on patients with painful bilateral hip OA with a body mass index (BMI)
RESULTS:
Twenty patients (40 hips) were enrolled and randomized into two groups: PNF group (mean age: 70.7
CONCLUSION:
The results of this pilot RCT showed that incorporating PNF exercises into the rehabilitation program yielded notable enhancements in improving lower limb function, strength and ROM in hip OA patients. Nonetheless, further prospective studies including wider sample size are needed to implement scientific knowledge on this physical therapy approach, in patients with hip osteoarthritis.
Background
Hip osteoarthritis (OA) is a major cause of hip pain, functional disability, and poor quality of life particularly in older people [1]. Risk factors include age, female sex, obesity, genetics and major joint injury [2]. Its prevalence has been gradually increasing in both low- and high-income countries, with a significant burden on healthcare systems around the world [3]. Pain is a crucial symptom of OA syndrome, and is what usually leads those affected to seek medical care [4]. Besides, these patients with hip OA have reduced hip range of motion (ROM), compared to healthy peers [5], and a generalized reduction in lower limb muscle strength [6]. Several studies have documented that impairments in both of these domains are associated with limitations in functional performance [5, 6, 7] and self-reported physical function [8]. In this context, it is mandatory an early diagnosis in order to improve the public health intervention to primary prevention and early detection of hip OA, with a positive implication also in the current management of these patients from a rehabilitative point of view [9, 10, 11].
Regarding non-pharmacological interventions, exercise and losing weight are strongly suggested, while participating in self-management programs and manual therapy in combination with supervised exercise were conditionally recommended [12].
The 2019 Osteoarthritis Research Society International (OARSI) guidelines established that structured land-based exercises are the core treatments for hip OA [13], while Ottawa guidelines defined that strength training exercises displayed a great improvement for pain, disability, physical function, stiffness, and range of motion in patients with hip OA [14].
Nevertheless, an amount of knowledge gaps remains concerning physical therapy approach for hip OA, such as the required frequency, intensity, type, and duration of exercises [15, 16, 17]; indeed, there is no agreement in the literature on which is the reference method to be applied in this condition, albeit it is recognized the role of physical exercise and nutraceuticals in modulating molecular pathways of osteoarthritis [15, 16, 17].
Several Proprioceptive Neuromuscular Facilitation (PNF) techniques commonly mentioned in the literature, including the contract-relax method and the contract-relax-antagonist-contract method to improve mobility [18, 19, 20], as well as the repeated contraction method and the replication method to facilitate neuromuscular outputs [21]. In fact, PNF is an approach planned to promote the neuromuscular mechanisms response, such as movement, muscular strength and resistance, joint stability, by stimulating the proprioceptive receptors within the skin, joints, muscles, and tendons [22]. Therefore, PNF is a comprehensive rehabilitation approach, that includes task-oriented training with the application of manual facilitation to promote motor learning, motor control, strength, and mobility in patients affected by several diseases [15, 23]. Initially, PNF techniques were used to aid rehabilitation of patients with spasticity by facilitating muscle stretching, through powered inhibitory mechanisms affecting the target muscle, and/or enhancing muscle strength through powered excitatory mechanisms, including patients affected by facial palsy [22, 23, 24, 25]. Then the PNF was started to be used also to treat other non-neurological conditions such as respiratory diseases, whiplash, and shoulder injuries [26, 27, 28].
Recently, there is evidence in the literature that PNF is more effective in increasing ROM through stretching, particularly regarding short-term ROM gains, compared to conventional interventions in young subjects with hamstring retraction of the limb [29]. In fact, PNF stretching is found to be beneficial in improving hip flexion range of motion, hamstring flexibility, thus increasing muscle strength [20]. Finally, PNF has already been shown to reduce pain and improve functionality in knee OA and even in cervical spine OA [30].
To the best of our knowledge, there is a gap in the published literature that lacks studies on the clinical effects of PNF in patients affected by hip OA. Therefore, the aim of this pilot randomized controlled trial (RCT) was to evaluate the efficacy of PNF on functioning in patients with hip OA.
Materials and methods
Participants
In this pilot RCT, patients affected by hip OA were recruited from the outpatient care of Physical and Rehabilitation Medicine, University Hospital “Renato Dulbecco” of Catanzaro, Italy from January to September 2022. Inclusion criteria were: (1) subjects aged from 65 to 85 years; (2) clinical diagnosis of bilateral hip OA according to the criteria defined by the American College of Rheumatology [31]; (3) hip pain defined by a Numeric Rating Scale (NRS)
We excluded patients with the following characteristics: (1) important cognitive impairment (Mini-Mental State Examination score
Ethical approval was obtained from the Ethics Committee of Calabria Region (number 168/2022). The study was performed according to the Consolidated Standards of Reporting Trials (CONSORT) guidelines and the Ethical Principles for Medical Research Involving Human Subjects outlined in the Declaration of Helsinki. All participants were fully informed about all experimental procedures and signed a written informed consent form prior to participation.
Intervention
At baseline (T0), participants were randomization (with a 1:1 ratio) into 2 treatment groups: Control group: patients undergoing manual therapy; and PNF group: the patients underwent the same treatment as the control group but with the addition of 10 treatment sessions according to PNF, lasting 45 minutes, 5 sessions/week for 2 weeks. In all patients, the same experienced physiotherapist treated left hip and right hip of each patient individually, with the same protocol, and then each hip was analyzed as belonging to a different patient.
The PNF protocol uses a tactile and proprioceptive afferently pool made up of the seven basic techniques (pattern, manual control, adequate and optimal resistance, verbal command, visual coordination, traction or approximation, stretch) to facilitate muscle contraction. It consists of the following techniques:
Pelvic tilt: the patient is in the lateral decubitus position on the bed. The therapist positions himself posteriorly to the patient, diagonally near the pelvis, places his hand anteriorly on the iliac crest and then overlaps the other hand. At this point he pulls down and back and asks the patient to bring the pelvis up and forward to the opposite shoulder. FADER (flexion, adduction and external rotation). In this scheme, the hip is extended, abducted and internally rotated, with the knee flexed and the foot in plantarflexion. The therapist places the proximal hand on the vastus medialis muscle and the distal hand on the instep with the four fingers on the medial edge. He asks the patient to bring up his hallux, straighten the knee and kick inwards. Hip flexion should occur simultaneously with knee extension. This is functionally the gait pattern, as the quadriceps muscle is engaged in both the hip flexion and knee extension components. EABIR (Extension Abduction, and internal rotation scheme): with a “A” variant, the scheme starts with the hip flexed, adducted and externally rotated, knee extended, foot dorsiflexed and supinated. The therapist places the distal hand with the thumb at the root of the fingers and the four fingers at the medial edge. The proximal hand goes under the thigh with the palm up on the hamstring muscle. The patient brings the leg down and out with the knee still extended. The heel turns outward and the foot extends plantar and pronated. Conversely, with the” B” variant, the patient brings the leg down and out while simultaneously flexing the knee, to activate the posterior bi-articularity. The heel turns outward and the foot extends plantar and pronated. EADER (Extension, Adduction, external rotation). The patient is supine. The scheme starts with the hip flexed, abducted and internally rotated, the knee flexed and the foot dorsiflexed. The proximal hand is in the inferior-medial area of the thigh on the semimembranosus and semitendinosus muscles, while the distal hand is cupped under the foot with the thumb at the root of the fingers. The therapist can easily tense all extensor muscle groups by closing all corners of the hip, knee and foot. In the beginning, the knee is positioned in the centre of the therapist’s chest. The hip extends, adducts, and externally rotates, the knee extends, and the foot extends and supinates. The pattern ends next to the other leg. Thus, it is the strongest triple extension pattern of the lower limb as it activates all the dominant components. Bridge progression: The patient positions himself with flexed hips and knees and feet in resting position. The patient is asked to lift the pelvis off the surface, contracting the buttocks, to maintain the position and then slowly return to the starting position. The bridge was proposed in an increasing progression of difficulty and that is why a recruitment pyramid has been created: (a) bridge on two legs, (b) bridge on one leg with the other resting on the therapist’s shoulder, (c) bridge on one leg with the other leg bent at the knee. (d) bridge on one leg with the other leg extended. (e) Bridge on one leg with the other leg extended, with a ball between the knees. Rhythmic stabilization: the technique consists of a series of consecutive and alternating isometric contractions of antagonistic muscle chains. The patient is supine in the single foot bridge position. The therapist applies resistance to the medial or lateral distal third of the thigh of the stance limb, asking the patient not move from his current position. The resistance from the opposite side is gradually introduced and the initial one gradually released. Moreover, the patient is then positioned in lateral decubitus with the hip extended, abducted 30∘ and internally rotated, the knee is extended. The therapist, placed along the diagonal, slight resistance anteriorly on the iliac spine or posteriorly with the hand placed edgewise on the gluteal crease, asking the patient not move from the position. The resistance from the opposite side is gradually introduced and the initial one gradually released.
Control group (conventional rehabilitation): underwent 10 sessions of manual therapy, lasting 45 minutes, 5 sessions/week for 2 weeks; the manual therapy included passive and active kinesiotherapy techniques (concentric and eccentric isotonic contractions), stretching techniques (passive in relaxation, whereby the therapist brings the muscular chain into tension and holds it for 60 seconds) on the hamstrings, quadriceps femoris, adductors, lateral rotator group and iliopsoas muscles.
Consolidated Standards of Reporting Trials (CONSORT) flowchart for trial recruitment.
For each patient, the left hip and the right hip were treated individually and bilaterally with the same protocol.
At the first visit, patients will receive a supply of paracetamol (500 mg tablets) as a rescue medication to relieve hip OA pain. In case of pain, patients can take up to 4 tablets (for a total of 2 g) per day of paracetamol, for a maximum of 4 days a week. In the event that patients take a greater amount of rescue medication, they will have to leave the study.
Outcome measures
The primary outcome was the Harris Hip Score (HHS), a disease-specific measure to assess the changes in hip function of patients with OA which contains eight items representing pain, walking function, activities of daily living, and range of motion of the hip joint. Final score ranges from 100 (no disability) to 0 (maximum disability) [32].
The secondary outcomes were: (1) pain in the hip, assessed by the NRS scale; (2) ROM of hip movements in terms of: abduction, adduction, flexion-extension, internal and external rotation; (3) muscle strength of the iliopsoas, quadriceps femoris, and hamstrings muscles, by Medical Research Council score (MRC); (4) physical performance, by 6-minute-walking test (6MWT): the score was measured using a single wearable inertial sensor (G-Sensor® BTS Bioengineering S.p.A., Milan, Italy) to instrumentally confirm the meters travelled during the 6MWT. This inertial sensor was positioned on the participant’s waist using a semi-elastic belt covering on the L4–L5 region for walking assessment, providing acceleration values along three orthogonal axes. The distance was recorded in meters. Post-processing of the data using dedicated software (BTS G-Studio; BTS Bioengineering S.p.A.); (5) disability-related quality of life (Health Related Quality of Life, HRQoL) measured with EuroQol 5 Dimensions 3 Levels Index (EQ-5D-3L Index) and EuroQol Visual Analogic Scale (EQ-VAS); (6) Balance and gait were assessed using the Tinetti balance scale. This test evaluates gait parameters such as speed, stride distance, symmetry, standing balance, and rotation. Maximum scores are 12 points for pace and 16 points for balance, for a total of 28 points [33]. The enrolled study participants were assessed at the baseline (T0), at the end of 2-week rehabilitation program (T1), at 3 months after baseline (T2), and at 6 months after the baseline (T3).
All patients and the physician in charge of outcome assessments were blinded to the allocation. The physiotherapist in charge of the intervention did not take part in the evaluation of the outcomes.
Statistical analysis
Statistical analysis was performed with R v5.3 (R foundation, Vienna, Austria). For statistical purposes, MRC scale was converted in ordinal data, with a score of 1 considered as 1, 1
Results
Out of the 62 hips assessed for eligibility (31 patients), 22 were excluded (see the CONSORT flow diagram in Fig. 1 for further details). As a result, twenty patients (40 hips) were enrolled after providing informed consent and were randomized into two groups: PNF group (mean age: 70.7
In detail, no between-group differences were found at the baseline assessment in terms of HHS score (PNF T0: 72.0
Results represented as marginal means plots. Experimental group: 1; control group: 2. Abbreviations: HHS: Harris Hip Score; NRS: numeric rating scale; ROM: range of motion.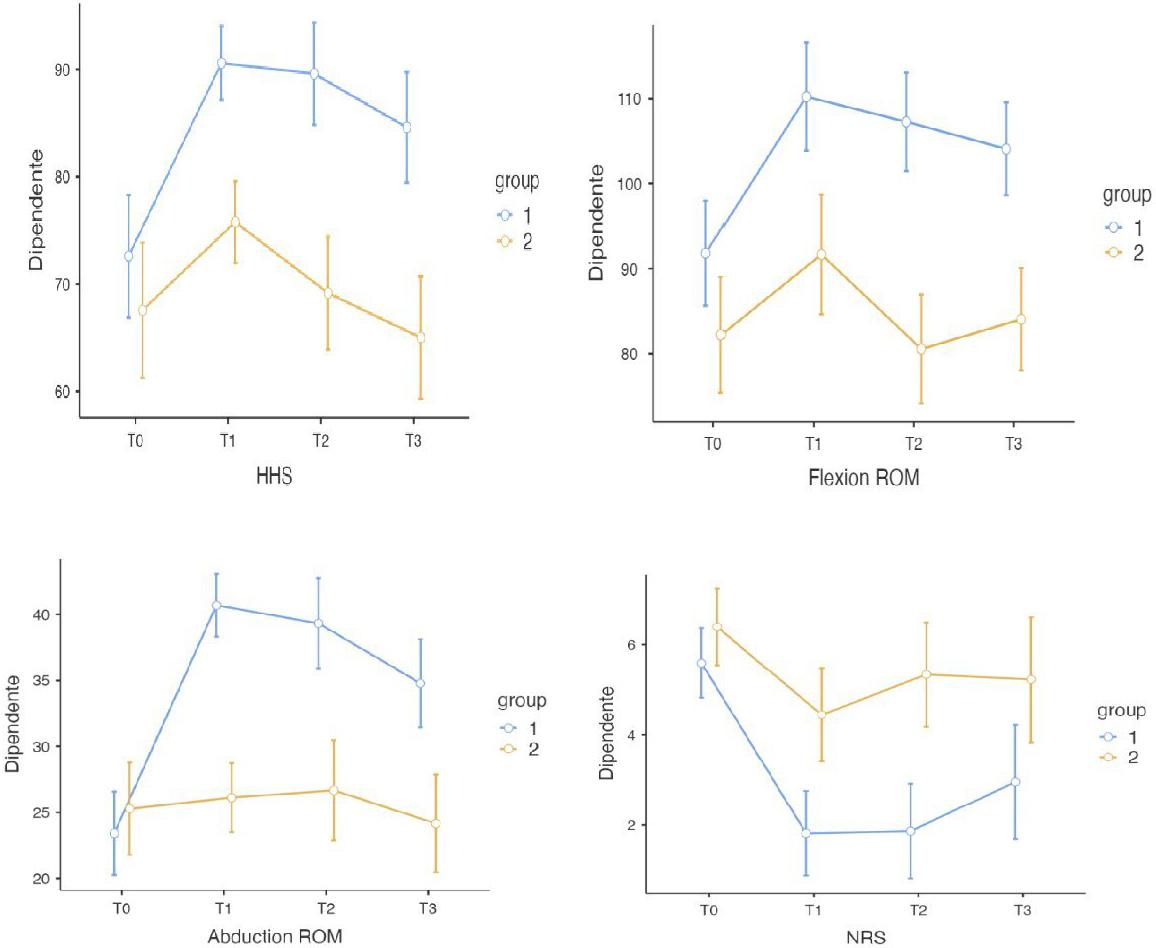
A statistically significant improvement in pain intensity was reported in the between-group analyses at all timepoints (
Furthermore, the between-group analysis demonstrated a statistically significant improvement in flexion ROM at T1 (T1:
Baseline characteristics
Continuous variables are expressed as means
In the abduction ROM measurement, there was a statistically significant improvement in the experimental group (
Results represented as marginal means plots. Experimental group: 1; control group: 2. Abbreviations: MRC: medical research council; EURO-QoL 5D-3L: EuroQol 5 Dimensions 3 Levels; 6MWT: six-minute walking test.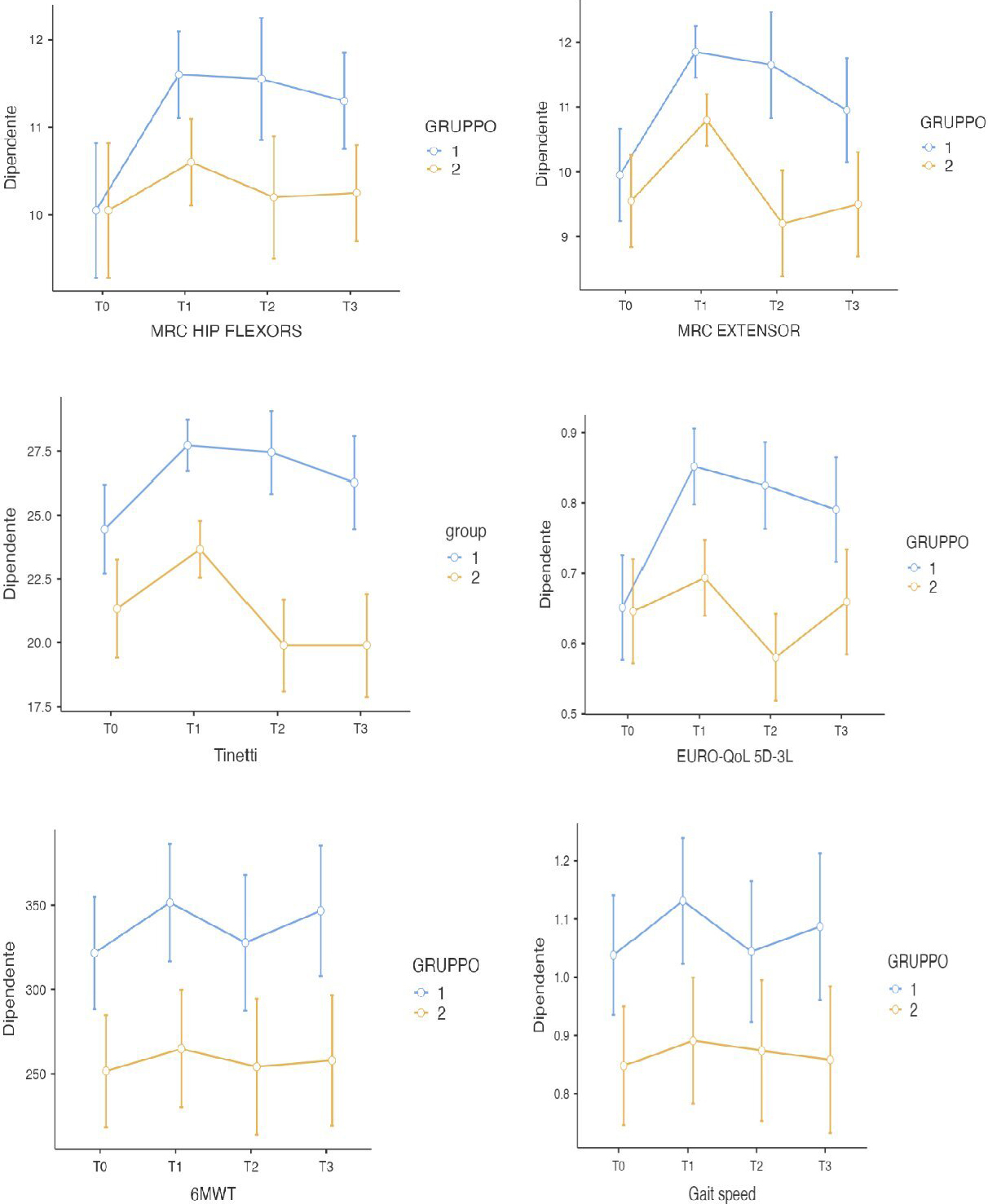
The results of muscle strength assessment through the MRC scale showed a statistically significant improvement (
Both intervention and control groups reported statistically significant improvements in Tinetti scale after treatment (
Repeated measures differences in outcome measures for the CONTROL and PNF (proprioceptive neuromuscular facilitation) groups
Continuous variables are expressed as means
A statistically significant difference in the EQ5D3L Index rating scale was found at T1 (
Moreover, a statistically significant improvement (
Similarly, in gait speed assessment, it was reported a statistically significant improvement (
The aim of this pilot RCT was to demonstrate the efficacy of a rehabilitation treatment based on the PNF approach in patients with hip OA, compared to treatment based on conventional physical therapy. Interestingly, integrating PNF 6-packs of therapeutic exercises into the conventional rehabilitation program led to statistically significant improvements in most of the outcome measures. First of all, the HHS recorded an improvement in the study group compared to the control group with a score maintenance at 3 months after the end of the treatment supporting the positive medium-term effects of PNF. In this scenario, the previous study by Schiavi et al. [34], reported a statistically significant improvement in HHS score (
Although previous studies demonstrated that the PNF method is effective in reducing pain in patients with knee OA and cervical spine OA [30], the results of our study suggested that PNF could be considered a safe and reliable rehabilitation technique inducing pain relief also in people with hip OA. This reduction in pain intensity assessed by NRS scale was statistically significant even after three months and six months of follow-up, in contrast with the control group showing a significant increase in hip pain after six months from the end of treatment. In the RCT by Poulsen et al. [36], which compared the education of the patient with hip OA with or without the aid of manual therapy in pain relief, the combination of the two interventions decreased the NRS scale by about 1.90 points at T1, which then increased after twelve months. In our RCT, our data showed a reduction of 4.1 points in NRS score, which is also maintained at T2 with a statistically significant improvement (
In the contraction-relaxation and hold-relaxation techniques, resisting the stretch generates significant force and elongation within the stretched muscle; this large force is perceived as a noxious stimulus and is seen as potentially hurtful, which triggers activation of the Golgi tendon organs (GTOs) which inhibit stretch to prevent injury. On the other hand, some authors suggested that even pain can be inhibited by sensory inputs from GTOS [40].
To date, PNF stretching techniques are commonly used in sports and clinical environments to improve both active and passive ROM to optimize motor performance and rehabilitation; in fact PNF stretching has been described as an effective stretching technique when the goal is to increase ROM, particularly in short-term [37]. Our findings showed a significant increase in ROM both in hip flexion (
In this scenario, Hando et al. [40] reported the efficacy of manual therapy on ROM for hip OA, demonstrating an increase in hip flexion of approximately 25∘ after the end of the treatment. Manual therapy consisted of muscle stretches, joint movements, and muscle lengthening, combined with exercises over an 8-week period. Thus contraction-holding-relaxation-stretching technique could actively recruit the posterior chain, the gluteal muscles (large, medium and small) and the hamstrings also subjected to stretching techniques, differentiating the posterolateral compartment (femoral biceps) from the posteromedial compartment (semimembranosus and semitendinosus). The work on the lengths of these anti-gravity muscles prevents shortening and improves their expression of strength. In fact, the improvements of PNF method were also statistically significant in terms of muscle strength. It had already been studied how the PNF method is beneficial in improving muscle strength and endurance in patients with knee OA [41].
Moreover, in patients with hip osteoarthritis we recorded improvements in muscle performance assessed using the MRC scale, both in flexors and extensors (
Balance and gait parameters showed a significant improvement both at T1 and at T2 (
Interestingly, our data underlined considerable improvements in the quality of life of patients with hip OA in the short term, using the Euro-QoL 5D-3L scale, which through a descriptive model, examines: mobility, self-care, usual activities, pain/discomfort and anxiety/depression [47]. A RCT by Saffari et al. [48] assessed the effectiveness of an intervention based on a theory of planned behaviour in improving health-related quality of life in middle-aged and older adults with hip or knee osteoarthritis. After three months of treatment, the authors recorded a significant improvement in T1 of 0.28; similarly, our findings showed an improvement of 0.20 in the EQ-5D-3L, which was maintained at 3 and 6 months after the end of the treatment. We also found significant increases in terms of distance in the 6MWT at T1 (
It is important to stress, however, that weight loss and exercise lead to better function and less pain. Hence the advantages of combining treatments to strengthen the effects [50].
Altogether, our data suggested that PNF treatment can effectively integrated with a conventional rehabilitation approach in people with hip OA, providing benefits in terms of physical performance, physical functioning, pain intensity, and HR-QoL. To the better of our knowledge, this is the first pilot RCT assessing the role of PNF associated with a conventional rehabilitation approach in people with hip OA.
Despite these considerations, this study is not free from limitations: first, inherent in the design of the study itself, a pilot study needs larger samples to validate or reject the results obtained. Secondly, in compiling the various outcomes, we evaluated each individual patient’s hip as a separate datum from the evaluation of the contralateral one, but the global functionality of the hip joint should be considered as unique. We also included subjects with a BMI
Conclusions
Taken together, the findings of this pilot RCT showed the efficacy of treatment based on the PNF method and how it can significantly improve lower limb function, strength and ROM in a cohort of patients with hip OA. Furthermore, patients’ perception of quality of life increased; both balance and gait improved considerably in PNF group compared to control. The rationale for these results should be that PNF exploits the neurological mechanisms that regulate muscle contraction and gesture coordination to favour the recruitment of hypovalid motor units, and to stimulate the adoption of correct motor patterns, often altered in hip OA, through the mechanisms of neuromuscular facilitation and inhibition. Nonetheless, further prospective studies including wider sample size are needed to implement scientific knowledge on this physical therapy approach, in patients with hip osteoarthritis.
Ethical approval
Ethical approval was obtained from the Ethics Committee of Calabria Region (number 168/2022).
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Data availability statement
Data used to support the findings of this study are available from the corresponding author upon request.
Author contributions
Conceptualization: AdS; Methodology: AdS and AA; Investigation: RS, SF, and MS; Formal analysis: AdS, NM, and RS; Data curation: AdS and NM; Writing – original draft preparation, AdS, NM, and RS; Writing – review and editing: LL, MI, and AA; Visualization: SF and MS; Supervision: AdS. All the authors read and approved the final version of the manuscript.
Footnotes
Acknowledgments
The authors would like to thank Giuseppe Alessio and Salvatore Posteraro for their support of this work.
Conflict of interest
The authors have no conflicts of interests to declare.