
Abstract
BACKGROUND:
The local hemodynamic response after cupping therapy has been considered as a contributing factor for improving muscle tissue health; however, the effects of cupping pressure and duration on the spatial hemodynamic response have not been investigated.
OBJECTIVE:
The objective of this study was to investigate the hemodynamic response inside and outside the cupping cup under various pressures and durations of cupping therapy.
METHODS:
A 3-way factorial design with repeated measures was used to investigate the main and interaction effects of the location (areas inside and outside the cup), pressure (
RESULTS:
A significant three-way interaction of the location, pressure, and duration factors was observed in oxyhemoglobin (
CONCLUSION:
Our findings indicate that an appropriate combination of cupping pressure and duration can effectively affect the spatial hemodynamic response of the biceps.
Introduction
Cupping therapy is performed by applying cups to the selected skin area for creating negative pressure by flame or suction [1], and is usually used for relieving musculoskeletal pain [2, 3]. Although cupping therapy is a popular intervention, evidence of cupping therapy for managing musculoskeletal impairment remains insufficient and conflicting results of clinical trials on cupping therapy have been reported in the literature [2, 4, 5, 6]. A recent survey of 158 healthcare professionals in the United States on their practice of cupping therapy indicates that clinical guidelines for selecting appropriate cupping pressure and duration are not sufficient to guide their clinical practice [7]. There is a need to establish the dose-response relationship of cupping therapy for improving the clinical effectiveness of cupping therapy on managing musculoskeletal impairment [3, 8].
In order to better understand the effects of cupping therapy on managing musculoskeletal impairment, local hemodynamic responses have been proposed as a potential mediating factor for promoting musculoskeletal healing after cupping therapy [9, 10]. Skin hyperemia after cupping therapy has been reported in the literature [10, 11, 12]. Kim et al. demonstrated that cupping therapy resulted in an increase in muscle blood volume after cupping therapy [13]. Such an increase in skin and muscle blood flow may accelerate the removal of metabolic wastes and the supply of oxygen to the treated area for improving muscle tissue health [9, 10]. This hyperemic response is considered a protective increase in blood flow following cupping therapy [14, 15].
Understanding the effects of cupping pressure and duration on the hemodynamic regulation may help establish the dose-response relationship of cupping therapy for improving the clinical effectiveness [9, 10]. However, there is only limited evidence on the effects of pressure and duration of cupping therapy on the hemodynamic response of the skin and muscle [10, 11, 12]. The regulation of muscle hemodynamic response from other interventions (e.g. foam rolling massage [16] and muscle stretching [17] could be referenced to predict the hemodynamic response after cupping therapy. Soares and colleagues provided the first evidence that foam rolling massage improves skeletal muscle oxygenation [16]. They demonstrated that forearm muscle oxygenation increased after 30 sec of foam rolling massage while there was no change in muscle oxygenation after 2 min of rolling massage. In another example, the mechanical force acting on the muscle induced by muscle stretching has been demonstrated to be a force-dependent response to congestion of venules or arterioles in rats [17, 18]. Although muscle stretching is different from cupping therapy, it is logical to assume that the muscle hemodynamic response after cupping therapy is also a force-dependent response because of the muscle blood flow regulation in response to mechanical stresses [19, 20, 21]. In order to better understand the effects of pressure and duration of cupping therapy on the hemodynamic response of the muscle, more research studies are needed.
Near-infrared spectroscopy (NIRS) has been used to quantify the changes of the concentration of oxyhemoglobin, deoxy-hemoglobin, blood volume, and oxygenation in the tissue (e.g. muscle and brain) [14, 22, 23, 24]. NIRS is also been used to investigate muscle oxygen metabolism [16, 25], a factor identified as a critical determinant of the hyperemic response after stretching and exercise [14, 22, 23]. NIRS may be a useful tool to assess how various intensities of cupping therapy affect the hemodynamic response of the muscle. The use of NIRS for measuring muscle hemodynamic responses after cupping therapy is usually operated at a single site [13, 26]. However, spatial heterogeneity of the microcirculatory system is found in the muscle [27, 28, 29]. Wolf et al. used NIRS to measure 22 locations of the calf muscle hemodynamics and demonstrated a significant spatial heterogeneity of muscle hemodynamics [27]. Mizuno and colleagues also demonstrated that muscle hemodynamic response is highly heterogeneous based on its location, for example, proximal and distal sites [28]. Thus, a single-channel NIRS may not be sufficient to catch the whole hemodynamic response of the muscle inside and outside the cup. To date, there is no study using multi-channel NIRS to investigate the spatial hemodynamic response (i.e. both areas inside and outside the cupping rim) of the muscle after cupping therapy.
Under different cupping pressure and duration, the muscle hemodynamic responses may be further influenced by the spatial heterogeneity issues. Specifically, it is largely unknown whether the muscle outside the cupping cup could show a significant increase in blood flow after cupping therapy. Given the importance of oxidative metabolism to the functional capacity of muscle, a large spatial difference in oxygenation and blood volume between the area inside and outside the cup rim may confound the efficacy of cupping therapy Despite there is no standard guideline on the location for applying cupping therapy specific acupoints and trigger points are usually used in cupping therapy practice [8, 30]. However, it is unclear whether an offset of the cup to the predetermined acupoint would still benefit the treated muscle or not. Thus, it is needed to study the muscle hemodynamic response at the area inside the outside the cup, especially under various pressures and durations of cupping therapy.
Therefore, this study aimed to investigate if there is a spatial difference of the hemodynamic response of the biceps muscle between the area inside and immediately outside the cup under various pressures and durations of cupping therapy. In order to investigate the spatial effect of muscle hemodynamic response to various treatment characteristics of cupping therapy, a three-way factorial design was conducted to assess the effect of the location, pressure and duration of cupping therapy on muscle hemodynamic responses using multi-channel NIRS. We hypothesized that: 1) there is an interaction between the location, pressure and duration of cupping therapy on muscle hemodynamic responses including oxyhemoglobin, deoxy-hemoglobin, blood volume and oxygenation (hypothesis #1); and 2) cupping therapy could significantly improve muscle blood volume in the area outside the cup (hypothesis #2). The long-term goal of our research is to establish the dose-response relationship of cupping pressure, duration and location (areas inside and outside cup) on the muscle hemodynamic response for improving clinical effectiveness of cupping therapy.
Methods
A 2
Participants
The inclusion criteria were healthy individuals aged between 18 and 40 years. The exclusion criteria were as follows: non-blanchable response of the red skin areas over the biceps and triceps of the dominant side, open wounds, scar or tattoo over the tested area, diagnosed ischemic cardiovascular hypertension (SBP
(A) The drawing shows the location of 10 photodetectors and 4 near-infrared light sources for a total of 16 channels of the sensor band. The grey circular area indicates the area inside the cup. The channels 9, 10, 11, and 12 are used to calculate muscle hemodynamic responses inside cup, and the channels 7, 8, 13 and 14 are used to calculate muscle hemodynamic responses outside cup. (B) Examples of time-series data of oxyhemoglobin and deoxy-hemoglobin from different channels after cupping therapy. Channel 7 signals (CH7) are from the area outside the cup and Channel 9 signals (CH9) are from the area inside the cup.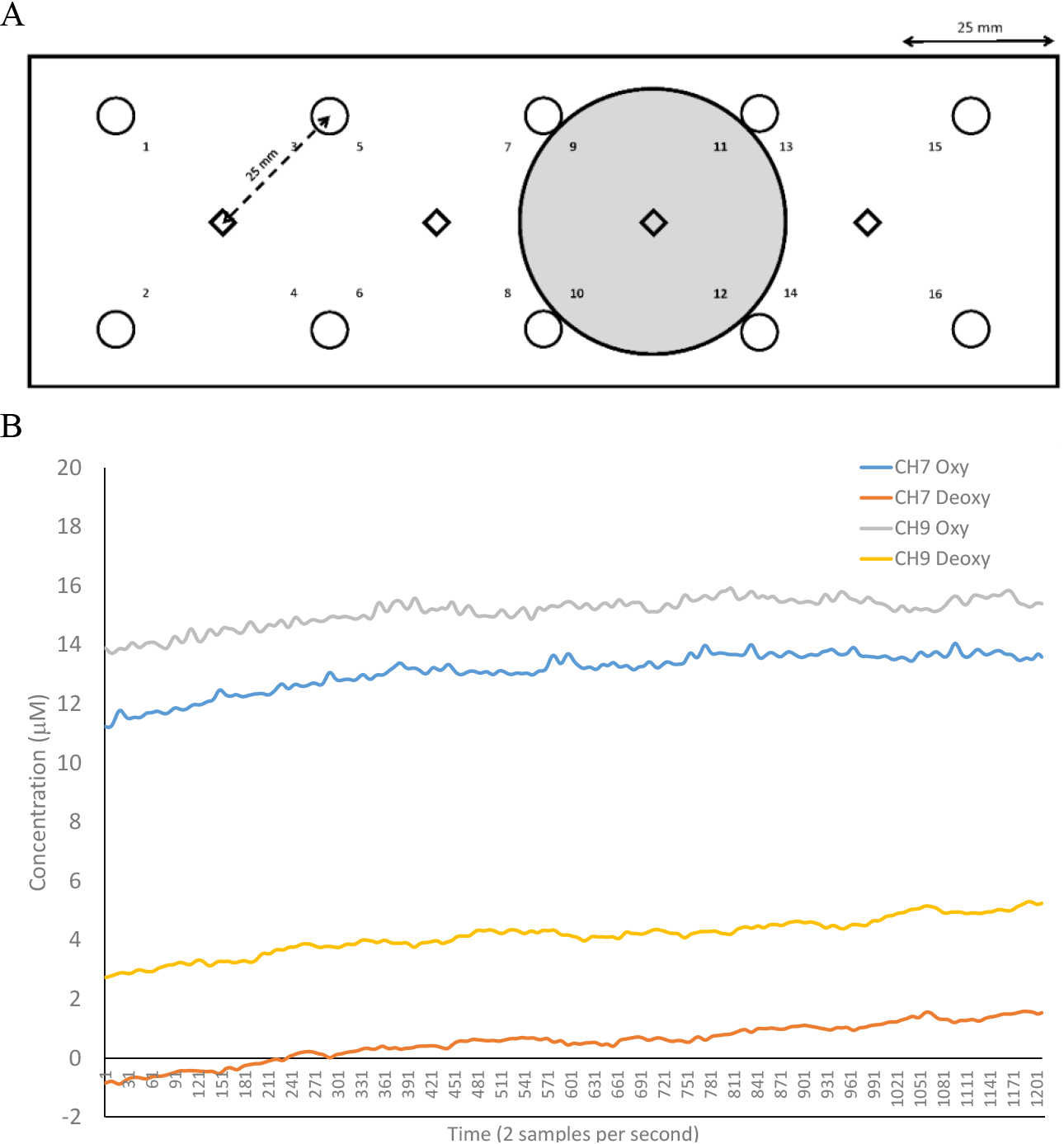
A functional NIRS sensor band (fNIR Imager 1000, fNIR Devices LLC, Potomac, MD, USA) was used to measure changes in hemodynamic responses of the biceps muscle, including oxyhemoglobin, deoxy-hemoglobin, blood volume and oxygenation (Fig. 1A). In this study, oxyhemoglobin represents the concentration change of oxyhemoglobin (
This study used an automatic suction device (P1000-PCS, California Medical Device Manufacturing Facility, CA, USA) to create a negative pressure inside the cup by using an electrical suction pump. The device consists of a vacuum gauge, a vacuum regulator, a power switch, and a vacuum cup. This device can produce negative pressure ranging from 0 to
Procedures
All testing procedures were performed in the Rehabilitation Engineering Laboratory at the University of Illinois at Urbana-Champaign in a thermos-neutral environment (24–26∘C). Subjects visited the laboratory for four days separated by at least 24 h and not more than 72 h. The participant rested at least 30 min in a supine position to acclimate to room temperature. Before the testing session, a mark was drawn on the biceps muscle (from the center of the cubital fossa to one-third of the acromion) to identify the location of applying the cup. Three marks on the four corners of the band of NIRS sensor were drawn to mark the location of the NIRS band. The NIRS sensor was used to measure the hemodynamic activity of the biceps muscle for 5 min. During the whole procedure, participants were asked to keep the same position and do not move. The participant fully extended the dominant-side elbow with the palm facing upward, and the angle between the arm and the body was 45 degrees. Elastic bandage was used to wrap the NIRS sensor to the arm to prevent any extraneous light from interfering with the NIRS signal. The pre-cupping hemodynamic activity was measured for 5 minutes. Then, the cupping cup with the inner diameter of 45 mm was applied on the biceps muscle area (in the center of cubital fossa to one-third of acromion) for either 5 min or 10 min at either
Several procedures were used to decrease biases in this study. Research participants were blinded for 4 cupping therapy protocols. They were instructed that different intensities of cupping therapy would be tested. One researcher performed data collection procedures and saved the NIRS files as protocols A, B, C, and D. Another researcher performed standard signal processing (low pass filter) to these files named as A, B, C and D who was not aware of the research hypotheses.
Statistical analysis
The three-way analysis of variance (ANOVA) with repeated measures was used to examine the main effect of location (areas inside and outside cup), pressure (
Results
Eighteen healthy individuals (12 women, 6 men) volunteered to participate in the present study and their characteristics were: age 25.0
Statistical results of the three-way ANOVA with repeated measures on the main effects of location (inside and outside the cup), pressure (
225 and
300 mmHg), duration (5 and 10 min) and the interaction effect among location, pressure, and duration on muscle hemodynamic responses
Statistical results of the three-way ANOVA with repeated measures on the main effects of location (inside and outside the cup), pressure (
*Indicates
A significant three-way interaction of the location, pressure, and duration factors was observed in oxyhemoglobin (
There was a significant main effect on the duration factor on oxyhemoglobin (
The deoxy-hemoglobin response
A significant three-way interaction of the location, pressure, and duration factors was observed in deoxy-hemoglobin (
(A) The averaged oxyhemoglobin responses of the biceps muscle measured at the area outside the cup after four intensities of cupping therapy. The values are presented as the change compared to the pre-cupping oxyhemoglobin value (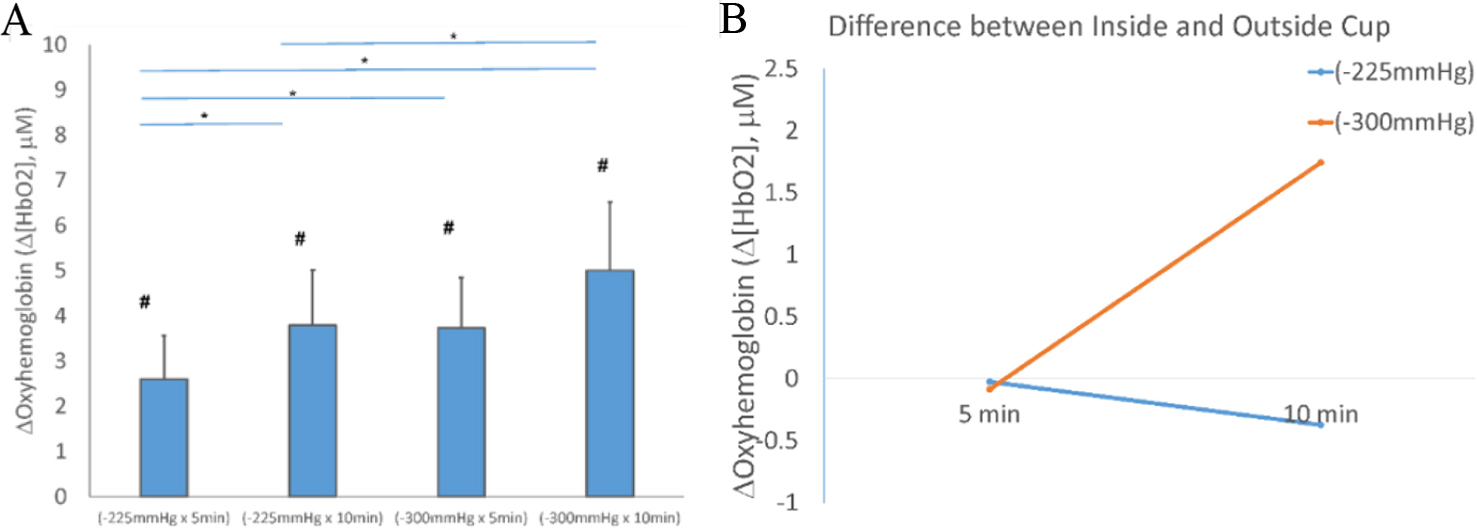
A significant three-way interaction of the location, pressure, and duration factors was observed in blood volume (
The oxygenation response
There was no significant interaction of the location, pressure and duration factors on oxygenation (
All individual data are presented in Fig. 6.
(A) The averaged deoxy-hemoglobin responses of the biceps muscle measured at the area outside the cup after four intensities of cupping therapy. The values are presented as the change compared to the pre-cupping deoxy-hemoglobin value (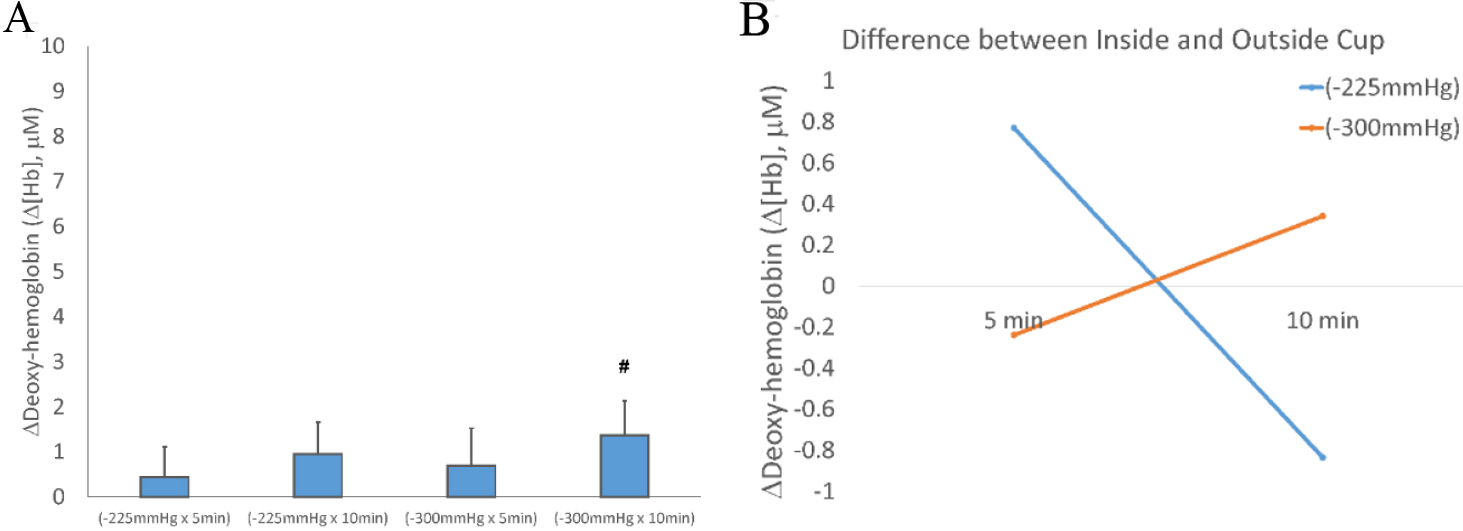
(A) The averaged blood volume responses of the biceps muscle measured at the area outside the cup after four intensities of cupping therapy. The values are presented as the change compared to the pre-cupping blood volume value (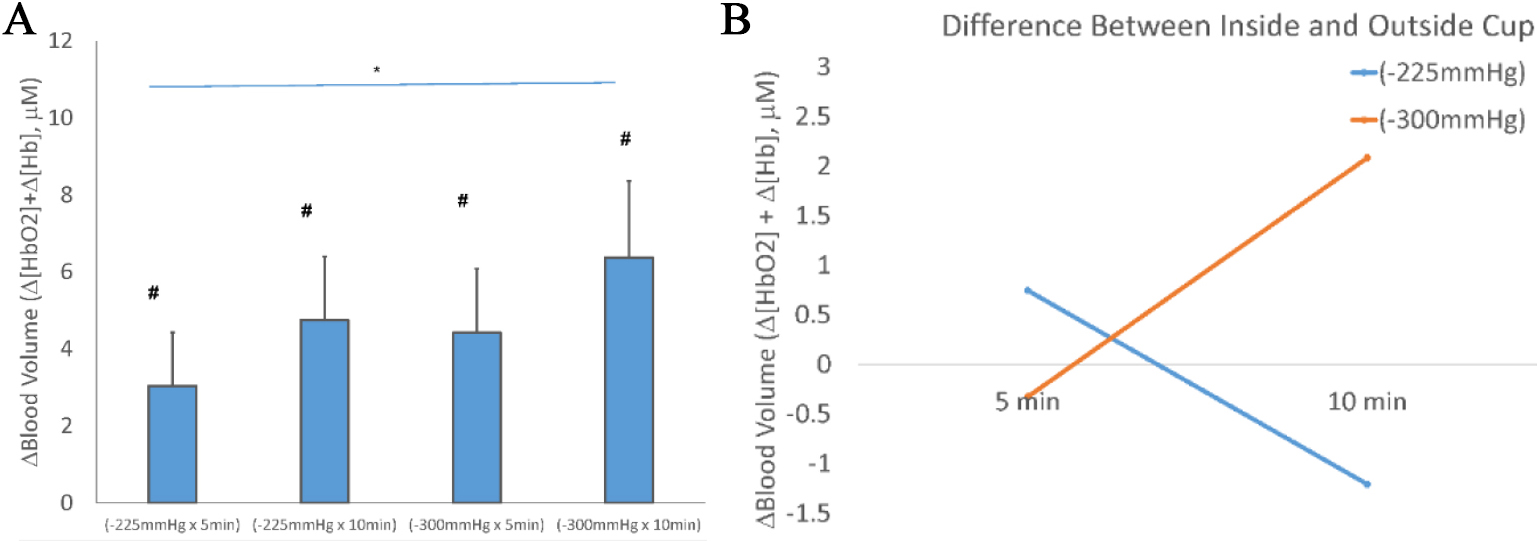
Our study demonstrated that the treated area outside the cup also showed a significant increase in oxyhemoglobin, blood volume and oxygenation of the biceps, and demonstrated a significant interaction effect between the location and duration factors and significant main effects of pressure and duration factors on oxyhemoglobin, blood volume and oxygenation This study found that the cupping intensity affects not only the area inside the cup but also the area outside the cup on oxyhemoglobin, blood volume and oxygenation of the biceps Our findings provide the first evidence of the dose-response relationship of cupping pressure, duration, and location on muscle oxygenation. Our findings indicate that an effective cupping therapy is determined by an appropriate combination of cupping pressure, duration, and location (the area inside and outside the cup).
(A) The oxygenation responses of the biceps muscle measured at the area outside the cup after four intensities of cupping therapy. The values are presented as the change compared to the pre-cupping oxygenation value (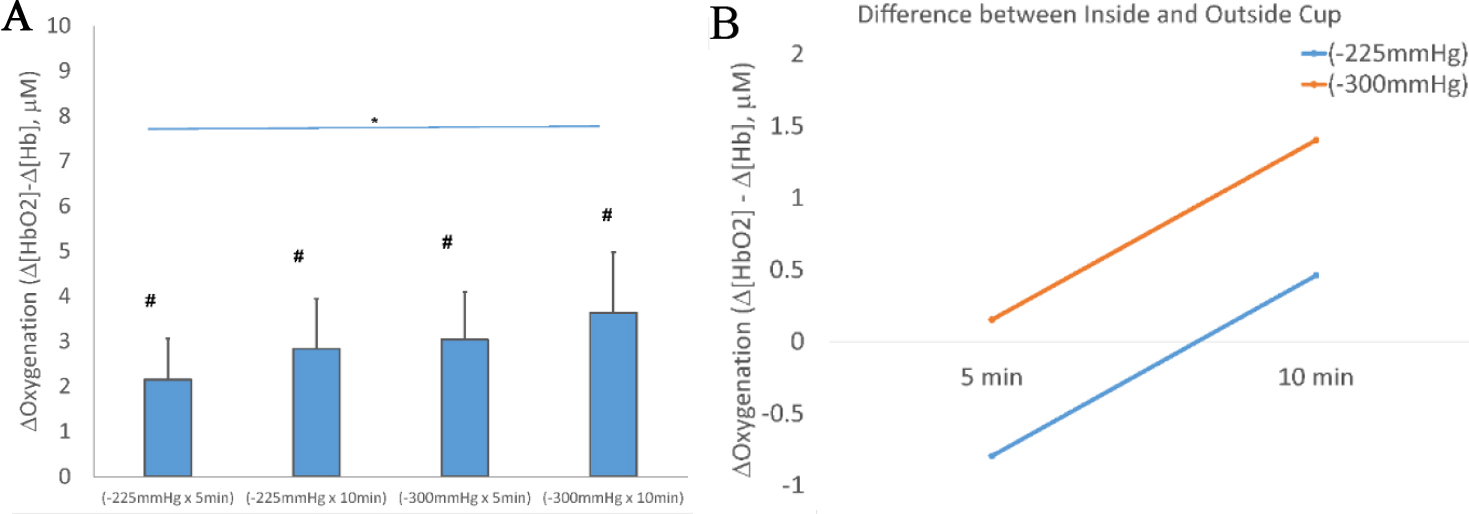
Individual data of A) oxyhemoglobin (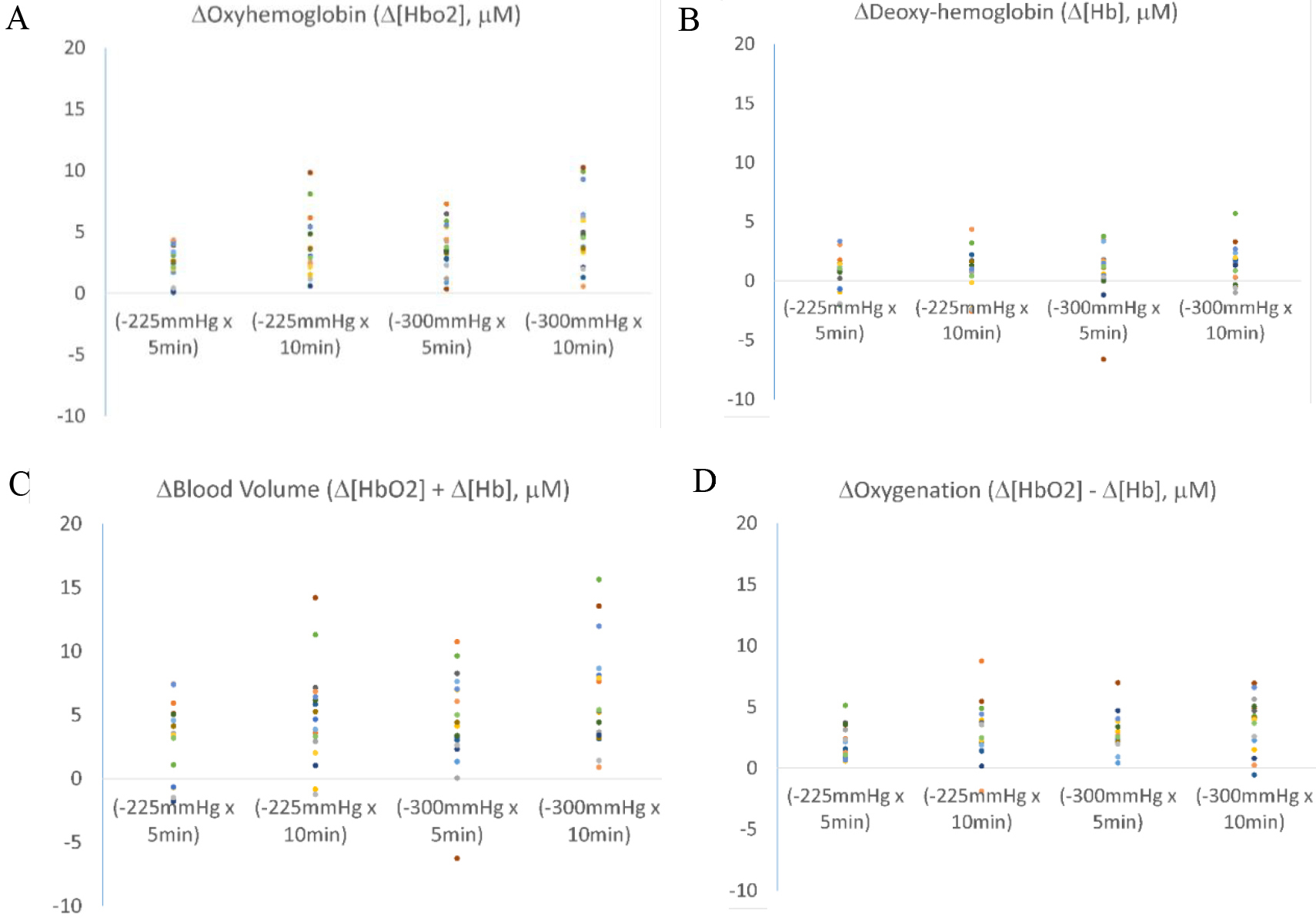
An important finding of the present study is a significant interaction between the location and duration factors for oxyhemoglobin (
To date, it remains unclear whether the hemodynamic response of the muscle from the area inside and outside the cup would be correlated. Our results indicate that the muscle hemodynamic responses in the areas inside and outside the cup are similar, although the muscle area inside the cup is under tension according to the finding from a simulation study, the muscle directly under the rim of the cup is under compression, and muscle outside the cup is not under tension nor compression [44]. The tensile stresses appear to be larger in a bulb-shaped region under the center of the cup. The existence of high tensile stresses inside the cup rim and in the central region enclosed by the cup is believed to be the primary cause of ecchymosis, a discoloration of the skin caused by the escape of blood into the tissue from ruptured blood vessels. This study reveals that there are no heterogeneities of oxyhemoglobin, deoxy-hemoglobin, blood volume, and oxygenation in the biceps muscle between the areas inside and outside (within 2.5 cm) the cup because both areas show similar responses to cupping therapy. It seems that the existence of high tensile stresses inside the cup rim and in the central region inside the cup implies the same level of mechanical stimulation to the muscle blood volume and oxygenation of the biceps brachii. Based on our results, the cupping effect is not only limited to the area inside the cup, but also the area outside the cup. Cupping therapy is usually used for the reduction of musculoskeletal pain; however, it may be difficult to find the exact pain point. The application of cupping therapy on the surrounding area may be able to induce the same physiological response as applying the cup on the exact acupoint or pain point.
Mechanical deformation of the vasculature may initiate rapid vasodilation in the contracting skeletal muscle. It appears that smooth muscle cells can directly respond to changes in elevated extravascular pressure, generally referred to as myogenic autoregulation [19]. Thus, a highintensity cupping therapy can induce a larger mechanical deformation of the vasculature, which induces a greater reactive hyperemic response [13, 26, 31]. Capillaries in skeletal muscle are surrounding myocytes, lengthening of sarcomeres will create a kinetic sequence of events moving outward such that the capillary extension reserve will cause compression and reduced vessel diameter. This alters vascular resistance and subsequently alters blood flow [45, 46]. However, it seems that muscle stretching needs to be under a certain physiological range for decreasing the mean capillary diameter and increasing blood flow after the removal of the stimulation [46]. For the spatial responses of oxyhemoglobin, deoxy-hemoglobin, blood volume and oxygenation in the biceps muscle after cupping therapy at different intensities, the level of mechanical deformation and the reduced capillary diameter of the vasculature in the areas inside and outside the cup are the same when the duration is short. As the cupping duration is longer, the reduced capillary diameter of the vasculature is different between the areas inside and outside the cup. The effects of mechanical stimulation on oxidation between the areas inside and outside the cup need a longer duration to reach a significant change. This may be partly explained by the results of our research.
One of potential benefits of cupping therapy is to increase metabolic demands of the treated muscle. Based on our results, cupping therapy may not be able to induce a higher metabolic rate of the muscle. Our results indicate that cupping pressure at
There are limitations of this study. First, this study was conducted in a homogenous group of participants with normal body mass index. The findings of this study may not be generalized to people who have obesity because of the potential influence of adipose tissue thickness on the penetration depth of the light of NIRS device as well as the mechanical forces induced by cupping therapy. Moreover, there were more females than males that may influence the results. Keller and Kennedy demonstrated that men exhibited faster skeletal muscle tissue desaturation than women after fatiguing handgrip exercise [55]. Future studies should investigate the gender and race effects on the hemodynamic response after cupping therapy. Second, a multi-channel fNIRS device was used in this study with a continuous-wave spectroscopy mode that only measures the relative changes of muscle oxyhemoglobin and deoxy-hemoglobin. It is unclear whether the setting of fNIRS could be directly used to measure muscle hemodynamic responses. It is noted that muscle oxygenation measured from NIRS could be cofounded by cutaneous microcirculation. Based on the findings from our previous studies, cupping therapy can significantly increase skin blood flow using laser Doppler flowmetry [10]. Third, the intensities of cupping therapy tested in this study included 4 common combinations of pressure (
The spatial response of oxyhemoglobin, deoxy-hemoglobin, blood volume, and oxygenation of the biceps muscle after various intensities of cupping therapy was investigated using a multi-channel NIRS system. Our results support that the clinicians should pay attention to cupping pressure and cupping duration for effectively improving muscle oxygenation. Our findings also indicate that the cupping duration factor is important when treating a wider area of soft tissue impairment because a sufficient duration is needed to induce a spatial response for improving muscle oxyhemoglobin of the area outside and inside the cup. Our findings indicate that an effective cupping therapy could benefit the area inside the cup and immediately outside the cup.
Author contributions
YJ conceptualized the study; YL, PM, JG, and ZS collected data; and all authors contributed to the analysis of data and writing of the manuscript.
Data availability statement
The dataset generated during this study is not publically available due to planned computational analyses for publication, but is available from the corresponding author upon reasonable request.
Ethical approval
The study protocol was approved by the Institutional Review Board at the University of Illinois at Urbana-Champaign (IRB #22900).
Funding
This study received no funding.
Informed consent
The participants gave written consent for participating in this study.
Footnotes
Acknowledgments
None to report.
Conflict of interest
The authors declare that they have no conflicts of interest.