
Abstract
BACKGROUND:
Low back pain (LBP) has emerged as a major public health concern leading to significant work productivity loss and deterioration in the quality of life.
OBJECTIVE:
A randomized, double-blind, placebo-controlled parallel-group clinical trial was conducted to investigate the effect of E-PR-01, a proprietary blend of Vitex negundo leaves and zingiber officinale rhizome, in individuals with LBP.
METHODS:
Seventy-two individuals aged 18 to 60 years with LBP were randomized in a 1:1 ratio in either the E-PR-01 or placebo group. The participants were instructed to take 2 capsules/day of the study products in two divided doses for 30 days. The study outcomes were changes in functional activity, bending flexibility, pain intensity, work productivity, and sleep quality. The sustained effect of the study products was also evaluated on the pain and physical functioning for 7 days after stopping the product intake. The product’s safety was evaluated by adverse events reporting throughout the study.
RESULTS:
Compared to the placebo, the E-PR-01 demonstrated a statistically significant reduction in functional disability (mean RMQ score:
CONCLUSION:
E-PR-01 significantly improved low back pain and bending flexibility in adults without adverse effects. Moreover, the effect of E-PR-01 lasted 7 days after stopping the intervention.
Keywords
Introduction
With the advancement in digital technology, more and more workforce is trying to learn new skills to transition to office-based white-collar jobs. The recent COVID-19 pandemic has fuelled this trend. However, one cannot ignore the harm that a sedentary lifestyle causes to an individual’s health because of prolonged daily sitting time [1, 2]. A sedentary lifestyle amplifies the risk of developing chronic pain [3]. Extended sitting hours at the workplace can increase the risk of non-communicable health disorders by 10–20% [4]. Recent trends have shown that the sedentary behaviour is a rising health concern and an adult individual spends majority of their waking hours sedentary [5].
Several studies demonstrate that individuals with a longer static sitting behavior are at higher risk of chronic low back pain (LBP) [6]. Most LBPs are non-specific with unknown etiology; hence the physicians generally have to rely primarily on analgesics. The global prevalence of chronic LBP has extensively increased in the past two decades and it has been recommended to include it in the WHO’s priority disease list [7, 8, 9]. It has been proven that individuals with an active lifestyle involving energy expenditures of
Globally, countries are making policy decisions, preparing guidelines, and taking appropriate action to engage young and older populations in physical activity to lead healthier and more active lives [14, 15, 16]. A recent systematic review of clinical practice guidelines concluded that non-steroidal anti-inflammatory drugs (NSAIDs), antidepressants, exercise therapy, and psychosocial interventions are the most recommended modalities by primary healthcare practitioners to manage non-specific LBP. However, evidences show that very few individuals suffering from chronic LBP have been benefitted by analgesics, even in case of severe pain [17].
Plant-based food and nutrients have invariably been used to heal the body from the overuse injuries of the musculoskeletal system. Herbal extracts such as Solidago chilensis (Brazilian arnica), Harpagophytum procumbens (devil’s claw) and Symphytum officinale L. (comfrey) are seen to improve function and relieve pain in low back tensile loading, and many more are being studied [18, 19]. However, most of these studies could not meet one or more clinical relevance criteria for LBP set by their authors.
Based on the previous scientific literature and a screening study, Enovate Biolife developed E-PR-01, a proprietary blend consisting of Vitex negundo leaves and zingiber officinale (ginger) rhizome extracts. The phytochemicals and secondary metabolites present in the V. negundo plant have been studied for their medicinal properties such as anti-inflammatory, anti-diabetic, anti-oxidant, anti-cancer, and antimicrobial activity [20, 21]. Z. officinale is a part of the family Zingiberaceae and is rich in polyphenols, which has demonstrated its potential to reduce inflammation and oxidative stress [22]. Clinically, ginger has been used for pain relief in oral and topical forms in various joint conditions, including chronic LBP [23, 24]. However, no clinical trials investigated the synergistic effect of these two extracts for non-specific LBP.
E-PR-01 was tested simultaneously in another randomized placebo-controlled trial to evaluate its effect on physical activity-induced joint pain in healthy individuals [25]. It successfully proved its clinically and statistically significant effect in alleviating the pain perceived by the participants. To substantiate the evidence supporting the efficacy of E-PR-01, the primary outcome of the present study was to investigate E-PR-01’s efficacy on physical functional activity in adults with non-specific LBP and a lower level of physical activity. The secondary objectives were to study the product’s efficacy on other associated factors, including pain intensity, mobility, work productivity, and sleep quality.
Material and methods
Study design
The present study was designed as a randomized, double-blind, placebo-controlled, parallel-group trial conducted between September 2021 and February 2022 at three clinical sites in Mumbai, Maharashtra, India. The study was conducted in compliance with the ICH-GCP guidelines, the 2004 Declaration of Helsinki, and 2016 Ethical Guidelines for Biomedical Research on Human Participants, Indian Council of Medical Research, India. The study was registered on ClinicalTrials.gov (ID: NCT04980469, Date: July 28, 2021) and approved by the Harmony Ethical Research Committee (CDSCO Reg. No. ECR/1411/Inst/MH/2020) (Protocol ID: EB/210402/VT/LBP, Date: July 01, 2021), Mumbai, Maharashtra, India. Written informed consent was obtained from all participants before conducting any study-related procedures. The primary outcome of the study was to explore the effect of E-PR-01 on functional activities in minimally physically active adults compared to the placebo. The study also investigated effect of E-PR-01, the investigational product (IP) on bending flexibility, pain intensity, work productivity, and sleep quality. The sustained effect of IP on the pain and physical function for 7 days after intervention cessation was also explored in comparison to the placebo. In addition, the safety of the product was evaluated by the number, frequency, and severity of adverse events (AE) and the proportion of participants who experienced the AE. This study followed the Consolidated Standards of Reporting Trials (CONSORT) guideline for reporting the results.
Participants
Adults aged between 18 and 60 years who were physically inactive for more than one-third of their awake time as assessed by the Longitudinal Aging Study Amsterdam (LASA) sedentary behaviour questionnaire were recruited for the study. Individuals with history of non-specific low back pain of not more than 12 months with persistent pain for at least seven weeks were included. The study participants reported a moderate to severe pain intensity in the area between the 12th rib and buttock creases. Other inclusion criteria were as follows: 1) Roland-Morris Questionnaire (RMQ) score of
Intervention
Each E-PR-01 gelatin capsule contained 200 mg of a proprietary blend of the extracts of V. negundo L. leaves and Z. officinale rhizome, whereas the placebo comprised of the same amount of microcrystalline cellulose (MCC). The participants were to administer one capsule twice daily after breakfast (between 9 AM–10 AM) and before dinner (2–3 hours before bedtime) for 30 days. The dose of the product has previously been tested for its efficacy and safety in healthy adults with mild to moderate knee joint pain. When fed to rats, V. negundo leaf extract revealed the pain-relieving properties proposed to be mediated by prostaglandin synthesis inhibition [26] or inhibition of cyclooxygenase (COX)-2 without much interference with COX-1 pathways [27]. Some preclinical experiments have shown that V. negundo can reduce the levels of pro-inflammatory cytokines such as tumor necrosis factor-
To preserve the blinding in the study, identical placebo capsules containing microcrystalline cellulose and matching with E-PR-01 in size, shape, color, and texture were manufactured by Enovate Biolife in a GMP-compliant manufacturing facility. The study products were packed in identical packaging with similar labels for dispensing.
Study conduct
During the screening visit, all the potential participants were assessed for the eligibility criteria, as mentioned in the previous section. The medical and medication history of the participants were evaluated. Anthropometrics (weight, height, and body mass index) and vital parameters (blood pressure and pulse rate) measurements were performed and recorded. Blood samples were collected for the estimation of fasting blood glucose levels (Hexokinase/G-6-PDH method using Glucose assay on the ARCHITECT cSystems) and TSH (Electrochemiluminescence immunoassay “ECLIA” on Cobas e immunoassay analyzers).
For the assessment of physical inactivity, each participant completed the duly validated LASA questionnaire consisting of 10 items [37, 38]. Only participants who spent
The impact of the LBP on the functional activity of participants was evaluated using the Roland-Morris Disability Questionnaire (RMQ), [39] a questionnaire developed by Martin Roland, Director of the National Primary Care Research and Development Centre, University of Manchester, UK. This 24-item self-reporting questionnaire has been widely used to assess possible activity restrictions due to non-specific LBP. It has a better construct validity as a measure of physical function disability [40]. The total score ranges from 0 (no disability) to 24 (severe disability) [39, 41]. The participants with a Roland Morris disability score between
After a 7-day placebo run-in period, the screened participants were again evaluated for pain intensity and functional activity using a 100-mm Visual Analogue Scale (VAS) [43] and RMQ, respectively, on the day of randomization. The participants who reported no change in pain VAS and RMQ scores compared to the screening day and had more than 80% run-in medication compliance were randomized in a ratio of 1:1 to the E-PR-01 or the placebo group as per the randomization chart. The master randomization chart was generated using StatsDirect Software Ver. 3.1.17 by the statistician who was not directly involved in the study execution. The randomization chart was saved and secured with limited access to the designated person. One bottle of study products containing 70 capsules and a diary to record any missed or lost dose was dispensed to the randomized participants. The participants, investigators, and the research team directly involved in the study were blinded to the product allocation.
Acetaminophen (500 mg tablet) was dispensed to all the participants as rescue medication (RM). The participants were instructed to take one tablet of acetaminophen in case of pain intensity
Both groups had a 30-day intervention period followed by a 7-day follow-up period. The outcome assessment visits were conducted on days 0, 7, 30, and 37. A record of dispensed and returned products was maintained by counting the number of capsules in the bottle to ensure IP compliance. Any concomitant medication taken by the research participant was recorded in the source document and e-case report form during each clinical site visit. The participants with at least 90% compliance during the intervention period and who complied with all study requirements were included in the per-protocol population for efficacy analysis.
Outcome measures
Primary outcome
Functional activity
Physical functioning assessment was the primary efficacy outcome of the study and was measured by RMQ, as described in the previous section. The participants were instructed to complete the RMQ on days 0, 7, and 30. The total score was evaluated and compared to the baseline and the control group. The minimal clinically important difference (MCID) for this questionnaire was stated to be at least 3 points if the baseline score was
Secondary outcomes
Bending flexibility
The fingertip-to-floor test is a valid measurement of the forward bending flexibility and mobility of individuals with chronic LBP. It has been used in several therapeutic trials due to its excellent validity (Spearman’s correlation coefficient
LBP intensity
The 100-mm VAS with zero denoting no pain and 100 denoting the worst possible pain was used to measure the intensity of pain perceived by the participants over the past 24 hours in the low back region. On days 0, 7, and 30, the participants were asked to mark the point on the VAS corresponding to the level of pain experienced in the specified region.
Work productivity
Chronic LBP is associated with lower work productivity, as observed in several studies [46, 47]. Using the Work Productivity and Activity Impairment Questionnaire (WPAI), the impact of chronic LBP on work and the performance of regular activities performed by the participants during the past week was evaluated in the present study. It is a self-administered questionnaire comprising six questions categorized into 4 groups: 1) absenteeism (percentage of work time missed during professional engagement), 2) impairment while working, 3) percentage overall work impairment (absenteeism plus presenteeism), and 4) percentage activity impairment (impairment in day to day activities) [48]. It has been validated to determine the impact of musculoskeletal disorders on work productivity [49, 50]. The participants filled out the questionnaire on days 0 and 30. Higher scores indicated less work productivity or greater impairment.
Sleep quality
Chronic LBP significantly alters the sleep quality of the affected individuals, as evidenced by several experimental and observational studies [51, 52, 53, 54]. The Insomnia Severity Index (ISI) is a brief instrument that assesses the day and night time components associated with insomnia. It has been used previously for the diagnosis of insomnia in clinical practice and to detect the treatment response in clinical studies. It is a 7-item self-report questionnaire that assesses sleep onset, sleep maintenance, early morning awakening problems, sleep dissatisfaction, interference of sleep difficulties with daytime functioning, noticeability of sleep problems by others, and distress caused by sleep difficulties. A 5-point Likert scale is used to rate each item, wherein 0 indicates no problem and 4 indicates a very severe problem. The total score ranges from 0 to 28, and based on the score calculated, the insomnia severity was categorized- 0–7: no clinically significant insomnia, 8–14: subthreshold insomnia, 15–21: clinical insomnia (moderate severity), and 22–28: clinical insomnia (severe). Participants were asked to recall their sleep patterns for the past month at baseline and then fill out the questionnaire on day 30.
Sustained effect of the product
For the assessment of the sustained effect of IP consumption on chronic back pain, all the participants who completed the 30-day study period were given a virtual diary consisting of the 100-point VAS scale and the RMQ at the end of the study visit to record their pain intensity and functional activity, respectively, daily for the 7 days after the end of the study. Day-wise VAS scores and RMQ scores were compared between the groups at the end of the follow-up period.
Safety outcomes
Adverse event monitoring was performed throughout the study. Vitals (blood pressure and pulse rate) were measured at each visit. Also, if the systolic blood pressure was
Statistical analysis
The sample size for the present study was based on previous similar studies [25, 55, 56]. A sample size of approximately 90 was decided for eligibility screening. Considering an estimated screening failure rate of 20%, 72 participants were to be enrolled and randomized into 2 groups in the ratio of 1:1 for completing 60 participants (approx. 30 in each group considering dropout or loss to follow-up rate of 20%) across the groups for analysis which was sufficient to evaluate the robust and reliable estimates for the efficacy and safety outcomes.
Participant disposition.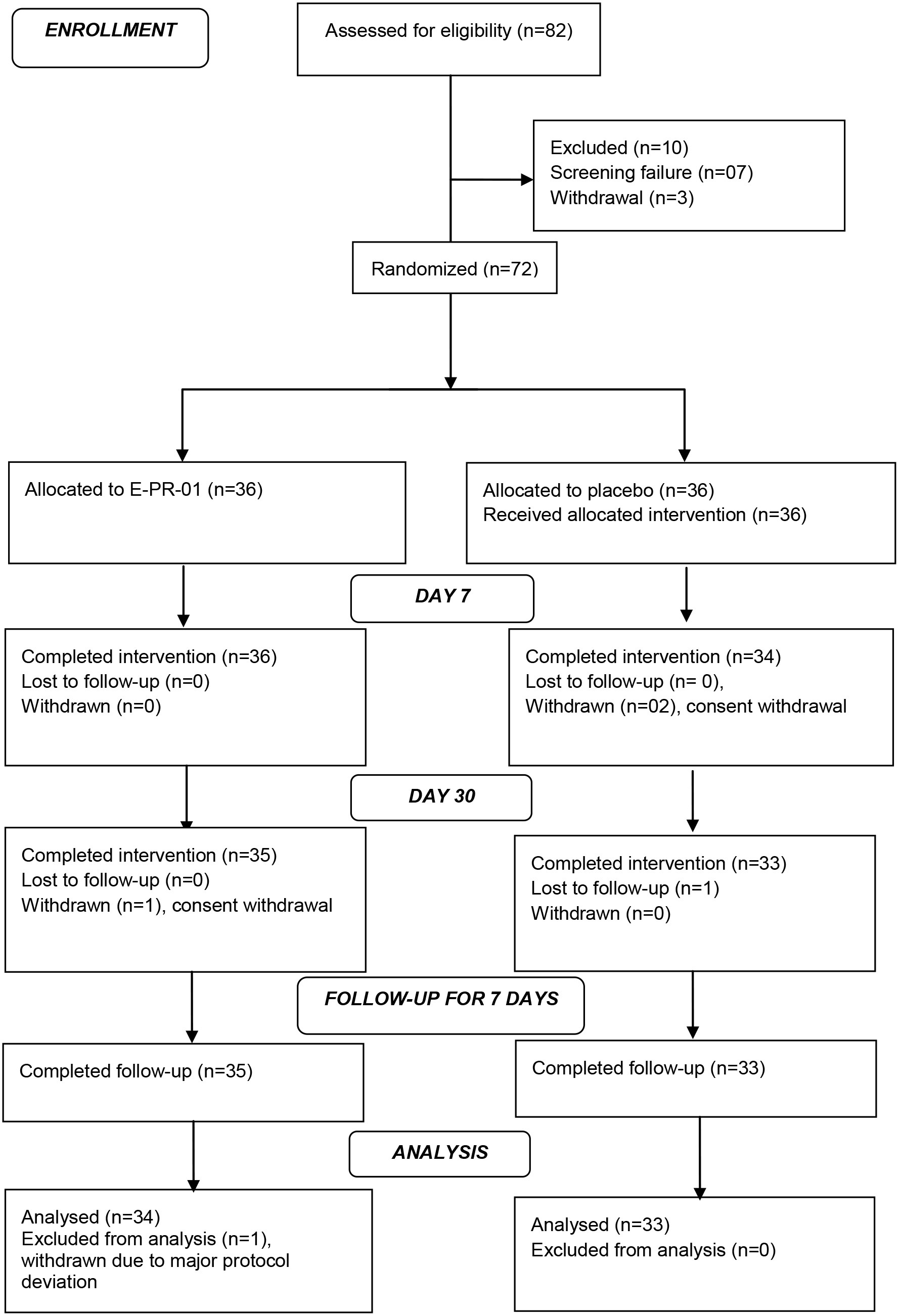
The data were analyzed using R/R Foundation for Statistical Computing, Vienna, Austria, and XLSTAT statistical and data analysis solution, New York, USA. In all analyses,
The study was planned based on the ICH-GCP guidelines, with a pre-approved monitoring and audit plan to ensure data quality.
Results
Participant disposition
Of the 82 participants screened, 7 could not fulfill the eligibility criteria, two were lost to follow-up, and one withdrew the consent. A total of 72 participants were randomized equally (
Demographic and other baseline characteristics [Mean (SD)]
Demographic and other baseline characteristics [Mean (SD)]
Notes: Percentages were calculated using the respective column header count as the denominator.
The two study groups were comparable in the demographic characteristics recorded at the screening visit. The overall mean (SD) age of the participants was 34.71 (7.93) years, with predominantly females in both groups. The physical inactivity time spent by the participants ranged from 6–14 hours per day, with a mean of approximately 10 hours per day. Table 1 summarizes the demographic and baseline characteristics of the randomized participants.
Summary of visit-wise roland morris disability questionnaire score
Summary of visit-wise roland morris disability questionnaire score
Notes: ap-value was calculated using ANCOVA with intervention as factor and baseline as covariate vs. placebo. bp-value was calculated using paired
Disability due to low back pain. RMQ, roland-morris disability questionnaire.
On the baseline visit, the mean RMQ scores of the study groups were comparable (
Effect on bending flexibility
On the baseline visit, the two study groups had a comparable mean distance between the right long finger to the floor with no statistically significant intergroup difference (
Effect on LBP intensity
The baseline pain VAS scores in both the E-PR-01 and the placebo group were comparable, with no statistically significant intergroup difference (
Summary of fingertip to floor test scores and pain VAS scores
Summary of fingertip to floor test scores and pain VAS scores
Notes: ap-value was calculated using ANCOVA with intervention as factor and baseline as covariate vs. placebo. bp-value was calculated using paired
Floor to finger distance.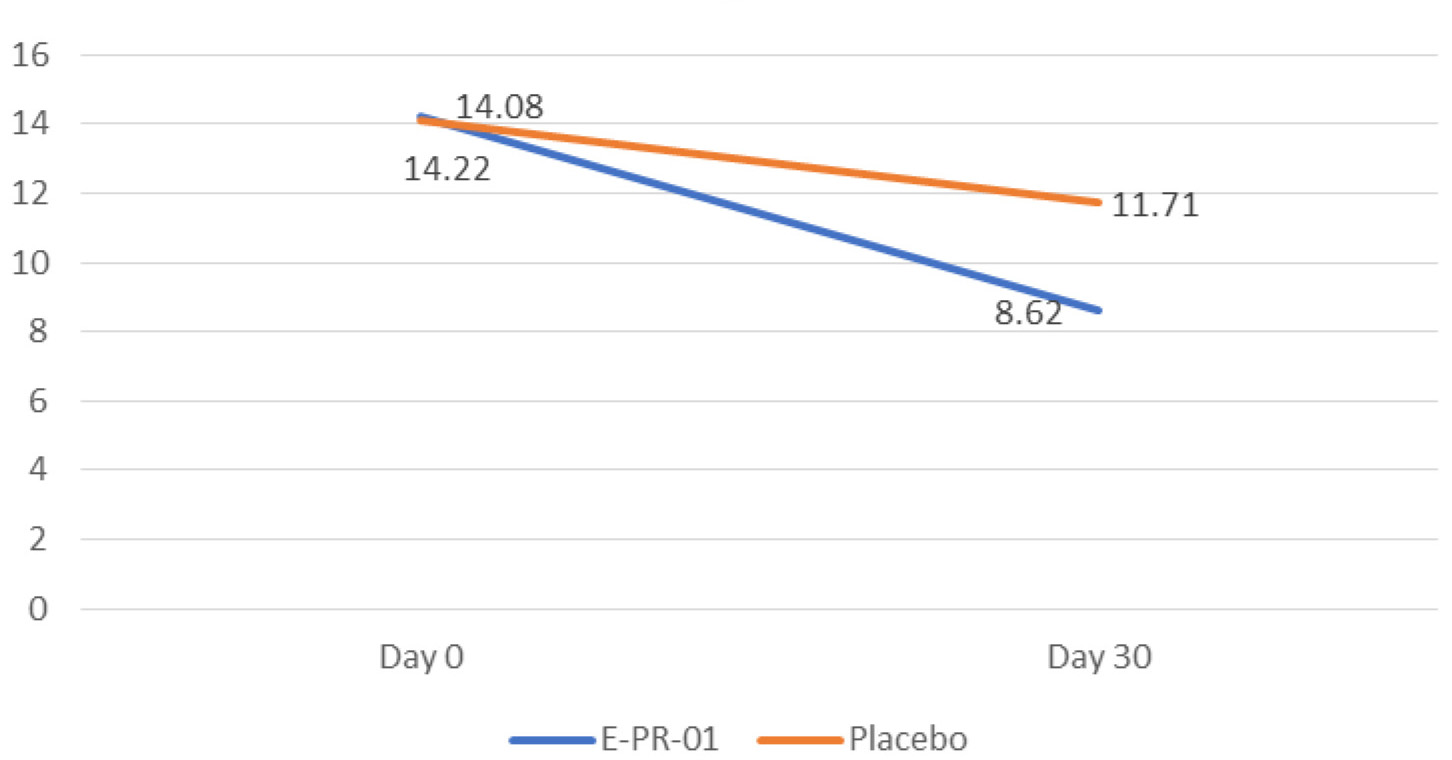
On day 30, there was a significant improvement in the pain VAS score in the E-PR-01 group from 16.23% to 41.8%, which was twice the improvement seen in the placebo group (19.73%). This result shows a statistically significant effect of the E-PR-01 group on pain intensity compared to the placebo (
Absenteeism due to LBP
Out of 67 participants analyzed, only 45 participants were professionally engaged. Twenty-four participants in the E-PR-01 group and 21 in the placebo group were evaluated for absenteeism from professional engagement. The total working hours in the E-PR-01 and the placebo were almost similar at baseline (mean (SD): 38.52 (14.50) vs. 39.48 (11.89);
Summary of work productivity and activity impairment questionnaire scores
Summary of work productivity and activity impairment questionnaire scores
Notes: ap-value was calculated using ANCOVA with intervention as factor and baseline as covariate vs. placebo. bOne observation was invalid, as the participant was on vacation on Day 30. cp-value was calculated using paired
On day 30, there was a reduction in the mean percentage of work time missed due to health in the E-PR-01 group; however, the magnitude of change from baseline was not statistically significant (
The mean percentage of impairment while working due to LBP was assessed for the same number of participants and was comparable for both groups with no statistically significant intergroup difference (
Overall work impairment due to LBP
The improvement in the percentage of overall work impairment during professional engagement after the 30-day administration of E-PR-01 was statistically significant compared to the baseline and the placebo group (
Impairment in day-to-day activities
The percentage of activity impairment in regular daily activity impairment other than professional engagement was assessed in 67 participants. After 30 days of intervention, both groups had a statistically significant reduction (
Effect on sleep quality
The baseline mean insomnia severity in both the study groups was at the subthreshold level and comparable (
Sustained effect of the product
The sustained effect of the product was measured over a follow-up period of 7 days after the cessation of the intervention by recording daily pain intensity on pain VAS and functional activity scores on RMQ. During this period, the participants were instructed to abstain from using any pain-relieving oral medications or topical applications. Both the groups showed a statistically significant sustained effect on the pain VAS scores and the functional activity till day 7. However, in the E-PR-01 group, the sustained effect was almost twice the magnitude noticed in the placebo group for both the pain intensity and the functional activity scores, and the difference between the two groups was also statistically significant (pain intensity (
Summary of the insomnia severity index
Summary of the insomnia severity index
Notes: ap-value was calculated using ANCOVA with intervention as factor and baseline as covariate vs. placebo. bp-value was calculated using paired
Sustained effect of IP on RMQ scores during the 7-day follow up period
Notes: ap-value was calculated using ANCOVA with intervention as factor and baseline as covariate vs. placebo. bp-value was calculated using paired
No significant change was observed in the vitals of the participants in both groups during the 30-day study period (Table 8). Two adverse events (dry cough,
Discussion
This 30-day randomized placebo-controlled clinical study was conducted to evaluate the efficacy of E-PR-01 in improving non-specific LBP and related work productivity in individuals having low physical activity levels. To date, no study has investigated the pain-relieving effect of V. negundo, one of the components of E-PR-01, in non-specific LBP-affected individuals. Several studies have previously investigated Ginger for its anti-inflammatory and anti-rheumatic activity in musculoskeletal pain [23]. However, only one study has reported its effect on chronic LBP wherein the effect of the local application of ginger oil was compared with a traditional Thai massage [24]. Management of non-specific LBP poses a unique challenge to the medical fraternity as most guidelines do not encourage the unjustified use of prescription analgesics [57]. The current study demonstrated that E-PR-01 not only reduced the pain intensity but also improved bending flexibility and work productivity in individuals suffering from non-specific LBP. Additionally, the improvement in functional activity and pain intensity was clinically significant as per the different MCIDs mentioned in the previous studies. The RMQ score in the E-PR-01 group was reduced by more than 30% by the end of one month of the administration, more than the MCID of 2.5, [58] 3.5, [59] and slightly exceeded the minimum level of detectable change of 5 points [41]. A
Sustained effect of IP on pain VAS scores during the 7-day follow-up period
Sustained effect of IP on pain VAS scores during the 7-day follow-up period
Notes: ap-value was calculated using ANCOVA with intervention as factor and baseline as covariate vs. placebo. bp-value was calculated using paired
Vital signs
Notes: ap-value was calculated using ANCOVA with intervention as factor and baseline as covariate vs. placebo. bp-value was calculated using paired
The bending flexibility, as measured by a fingertip-to-floor test, also showed highly significant improvement in the E-PR-01 group, which was almost twice as much as achieved in the placebo group. E-PR-01 also improved work productivity and reduced health-related activity impairment much better than the placebo, as evidenced by a highly significant reduction in percentage impairment while working (22.9 vs. 3.86) and overall work impairment (25.06 vs. 0.42) and activity impairment (25.59 vs. 11.52). This reduction was well above the MCID, as suggested by Tillett et al. in cases of Psoriatic arthritis [61]. No significant improvement was observed in absenteeism as assessed by work time missed in both groups. However, a positive trend was noticed in the E-PR-01 group, while the placebo group showed a reverse trend. Several observational studies have found a strong association between LBP and sleep quality [51, 52, 53, 54]. Improvement in sleep quality had previously improved the LBP and associated disability [62]. In our study, E-PR-01 improved the sleep quality of the participants significantly after one month of its administration compared to the placebo.
Previously oral intake of extracts of plants like moringa seed, Terminalia chebula fruit, Harpagophytum procumbens, and willow bark have been evaluated for their effect in reducing chronic LBP [63]. In a recently conducted study, the effect of moringa seed extract containing glucomoringin was examined on LBP in healthy working men and women. After four weeks of extract ingestion, the percentage change in the pain VAS scores was 35% which is lower than the percentage change observed in the E-PR-01 group [56]. A similar trend was noticed when the efficacy results of other herbal extracts (Terminalia chebula: 500 mg/day – 19.31%, 1000 mg/day – 18.97% in 12 weeks, and Harpagophytum procumbens root: 100 mg/day harpagoside – 40% in 4 weeks and willow bark: 120 mg salicin – 40% in 4 weeks) were compared with the results observed in the present study. Only willow bark extract having 240 mg salicin and Harpagophytum extract standardized to 50 mg/day harpagoside showed a better effect (67% and 60%, respectively) in the same intervention duration [55, 63, 64].
Chou et al., 2017 conducted a systematic review of clinical studies on systemic pharmacologic therapies like NSAIDs, skeletal muscle relaxants, antidepressants, and opioids; benzodiazepines, systemic corticosteroids, and antiseizure medications prescribed for LBP. The authors concluded that these therapies have small (defined as a reduction in pain by 5–10 points on a 0- to 100-point VAS or the equivalent and reduction in functional disability as 1–2 points on the RMQ) to moderate (defined as
A recent trial on weekly injections of platelet-rich plasma (5–6 mL) versus 15% lidocaine for 2 weeks followed by prolotherapy with 15% glucose solution for the next 2 weeks in chronic non-specific LBP reported a 23.3% improvement in mean RMQ scores in the lidocaine injection group and 35.25% in the platelet-rich plasma (PRP) injection after 4 weeks of administration which is lesser than the improvement (47.07%) observed in our study. It took 6 months for lidocaine and PRP to show improvement in disability scores equivalent to E-PR-01. The reduction in mean pain VAS scores in the lidocaine group was 24.56% vs. 27.11% in the PRP group, while the E-PR-01 group reported a reduction of 41.8% after 4 weeks of administration which was achieved after 6 months of administration in the lidocaine group and 3 months in the PRP group [66]. Another clinical trial conducted on a low dose (25 mg) amitriptyline versus 1 mg benztropine mesylate per day for 6 months showed a 28.9% reduction in pain intensity on the VAS from baseline to 6 months compared with a 12.67% reduction for the active comparator group which is lower than the reduction achieved in the E-PR-01 group in the present study. Compared to E-PR-01, the percentage reduction in RMQ scores was also lower, i.e., 37% and 23.17% for amitriptyline and benztropine mesylate, respectively, after 6 months of administration [67].
Currently, probiotics are being tested for their potential use in several health disorders. A recently conducted clinical study investigated the effect of Lactobacillus Rhamnosis on chronic LBP when administered at a dose of 6 billion twice daily for 100 days [68]. The study demonstrated a 13.33% vs. 10.52% reduction in back pain and 17.36% vs. 13.23% in disability scores in 100 days compared to a placebo.
Chronic back pain has been associated with lower quality of life [69, 70]. In addition to its remarkable effect on pain and functional activity, E-PR-01 has shown a significant effect on forward bending flexibility, work productivity, and sleep quality. Improvement in these outcomes can be attributed to the synergistic anti-inflammatory effect of the unique combination, which could help decrease pro-inflammatory markers such as IL-1
The present study demonstrated significant results in alleviating LBP and the investigational product E-PR-01 was found to be safe and well-tolerated. However, the long-term effect of the product was not assessed and extensive clinical trials are recommended to further explore the sustained effect of the product.
Based on the results of the present study and their comparisons with previous similar studies, we can say that both Vitex negundo and zingiber officinale extracts worked synergistically, producing a remarkable effect in controlling the pain and functional disability due to LBP without a specific etiology, a prevalent condition in today’s young as well as middle-aged generation who are having prolonged sitting hours at work or home. Additionally, it improved the overall quality of life by improving their work productivity and sleep quality.
Author contributions
Shalini Srivastava – conceptualization of the study, supervision of the study conduct, editing and reviewing the draft manuscript, finalization of the manuscript; Sagar Karvir – conduct of the study and reviewing the draft manuscript; Robert N. Girandola – editing and reviewing the draft manuscript and finalization of the manuscript. All authors read and approved the final manuscript.
Data availability statement
The data associated with the study are available from the corresponding author upon reasonable request.
Funding
Enovate Biolife funded the study and provided the study products.
Footnotes
Acknowledgments
The authors are thankful to all participants and investigators who participated in the study. The authors extend their gratitude to Enovate Biolife for providing the study products and Vedic Lifesciences for facilitating the execution of the study.
Conflict of interest
Shalini Srivastava is employed with Enovate Biolife. The other authors report no conflict of interest.