
Abstract
BACKGROUND:
Low back pain is prevalent in workers’ health and functional performance.
OBJECTIVE:
To evaluate the effects of a physical exercise program on low back pain and disability in fruit workers.
METHODS:
This randomized controlled trial assigned 44 workers (37
RESULTS:
A significant difference was observed in the within-group analysis, with a mean reduction in pain intensity in the EG and CG of
CONCLUSIONS:
The exercise program was not superior to using the educational booklet. However, both interventions showed substantial decreases in pain and disability levels.
Introduction
Low back pain is one of the most common skeletal disorders and the most prevalent work-related musculoskeletal disorder (WMSD), responsible for approximately 568.4 million cases worldwide in 2019 and reaching an annual prevalence of more than 50% in adults in Brazil [1, 2]. More recent data shows that low back pain prevalence rates increased by 26.8% between 1990 and 2017, being the leading cause of years lived with disability [3]. Low back pain can affect individual, physical, social, and psychological aspects, contributing to increased healthcare costs and work incapacity [4, 5, 6, 7, 8]. This condition was responsible for total social costs which totaled US$2.2 billion in Brazil between 2012 and 2016, and productivity losses accounted for 79% of these costs [4].
Low back pain in workers has shown a high prevalence and a strong relationship with absenteeism and presenteeism rates, being considered the leading cause of disability [7]. However, the prevalence rates vary according to the different branches of work, with values between 44 and 64% reported in health professionals, teachers, factory, and office workers [9, 10, 11, 12]. The reported prevalence of low back pain among agricultural workers can reach up to 86% [13, 14], and disability due to it is higher in low- and middle-income countries, where there are few possibilities for modifying work activities [7].
It is believed that a complex combination of factors causes low back pain. Among occupational factors, the type of work activity, maintenance of postures, repeated movements, and exposure to loads are considered important risk factors for low back pain [15, 16].
Agricultural workers perform activities which involve manual tasks performed in open environments and are often exposed to high temperatures [17, 18]. In addition to these factors, viticulture workers have greater overload in the upper limbs and trunk region, including twisting movements and repetitive lifting of excessive loads [19, 20]. The combination of these tasks and factors imposes a physical and functional demand related to the high prevalence rates of musculoskeletal complaints [21].
Different strategies for preventing and treating low back pain in workers have been researched in recent decades [22]. In this context, the practice of physical exercise has gained prominence due to its potential effects on reducing signs and symptoms of pain and improving the functional status of individuals [23]. In addition, the recent American Physical Therapy Association Clinical Practice Guidelines for low back pain strongly recommend using physical training interventions to treat chronic low back pain [24].
On the other hand, a recent systematic review with meta-analysis seeking to investigate the effect of physical exercise applied in the work environment on workers with low back pain, demonstrated that exercise was not superior to other pain management strategies, such as guidelines and booklets [25]. The studies included in this review [25] evaluated office and industry workers with acute and chronic low back pain.
Considering that agricultural workers have specific occupational demands [19, 20] and that acute and chronic conditions have different prognoses [26], the present study aimed to investigate the effect of an eight-week strength, endurance, and flexibility exercise program compared to guidance on pain and disability outcomes in fruit workers with chronic low back pain. The study hypothesized that the group submitted to physical exercise in the workplace would present a more significant reduction in their pain and disability levels.
Materials and methods
Study design
This is a randomized clinical trial with two parallel groups. All eligible volunteers were informed about the project steps and filled out a consent form to participate in the study. The protocol was duly approved by the Research Ethics Committee of the University of Pernambuco (protocol CAAE 17386919.6.0000.5207) and prospectively registered in the Brazilian Registry of Clinical Trials – REBEC (RBR-78bn48). In addition, all stages followed the recommendations provided by the “Consolidated Standards of Reporting Trials” (CONSORT) [27]. The study was conducted on two grape-producing farms in the cities of Lagoa Grande and Petrolina, located in the interior of Pernambuco, Brazil.
Participants
The study included fruit workers (men and women), aged between 21 and 55, physically independent, with chronic non-specific low back pain defined as pain or discomfort in the lumbar region of the spine for at least three months [28], with a minimum intensity of 3 on the Numerical Pain Scale [29, 30] and without a specific medical diagnosis. Additionally, participants with an unstable disease which contraindicated the practice of supervised physical exercise, with a history of trauma and/or surgery in the spine were not included. The exclusion criteria were practicing other physical activity programs, using medications and ergogenic resources, limiting health conditions, and pregnancy.
The sample size calculation was performed using the GPower 3.1.9.2 program to detect a 1.7-point difference in the intensity of chronic low back pain [31], with an estimated standard deviation of 1.51 points [32]. Considering a statistical power of 90%, alpha of 5%, and possible sample loss of 20%, 44 participants (22 in the experimental group and 22 in the control group) were included in the study.
Intervention
All participants were recruited from the same company, under the same leadership, and workers had the same work and break schedule. The intervention was carried out in specific accommodations for workers. All therapists involved with the interventions were adequately trained and qualified to respect the established protocols for the experimental and control groups.
Participants in the experimental group (EG) received an intervention consisting of supervised strength and flexibility exercise sessions performed in the workplace, each lasting between 20 and 28 minutes. The company established session times. For some workers it was at the end of the shift, while for others it was in the middle.
The training protocol was divided into three parts: 1) Stretching of the upper trapezius, pectoralis major, and erector spinae muscles. Then, stationary running. All exercises were performed in two series of 30 seconds; 2) the second part consisted of strengthening exercises for the upper and lower limbs, including resisted external shoulder rotation, push-ups, squats, horizontal row, and resisted shoulder abduction, lasting between 10–15 minutes; 3) the last part consisted of specific isometric strengthening exercises for CORE stabilization, lasting between 3–5 minutes, namely frontal plank and pelvic elevation (Fig. S1).
The recommendations of the American College of Sports Medicine for resistance strength [33] and some other indications related to intervals [34]were considered for planning the exercise program. The EG training program was conducted for eight weeks with a frequency of twice a week, on alternate days (Tuesdays and Thursdays) at the same time of day. In the first two weeks, subjects performed two sets of 12 to 15 repetitions, then progressing from the third to the fifth week to 10 to 12 repetitions. The participants performed three series from the sixth to the eighth week, varying from 8 to 10 repetitions. All exercises had recovery intervals of 30 seconds between exercises and 45 to 60 seconds between sets. The progression considered the number of series, repetitions, and positions according to the corresponding week. Load progression was performed for isotonic exercises using elastic bands, and plate weights (5 kg and 10 kg) were used.
Participants allocated to the control group (CG) were not submitted to any supervised training program in the workplace throughout the study. However, the team prepared a self-explanatory booklet with guidelines for performing exercises at home twice a week for these individuals. The booklet proposed stretching exercises for the posterior muscles of the cervical and thoracolumbar region, the anterior cervical muscles, the posterior muscles of the shoulder, pectoralis major, flexors and extensors of the elbow, wrist and fingers, and the lateral muscles of the trunk. Each stretching exercise should be held for 30 seconds and performed in two repetitions. Additionally, as a way of monitoring the activities proposed by the booklet, each participant was monitored weekly through telephone calls to collect information on the performance of the exercises, frequency, and possible adverse effects (Fig. S2).
Measurements
An individual assessment of the participants was initially conducted, including collecting sociodemographic data (age, marital status, sex, education), health history and back discomfort, history of physical activity, medication use, and anthropometric measurements (weight, height, and body mass index).
Then, the participants were evaluated considering the outcomes of interest. All instruments used in the present study were validated for the Brazilian population, and their measurement properties were previously assessed [35, 36, 37]. These measures were recommended by the Expert Committee on Low Back Pain as essential tools for clinical studies with individuals with low back pain [38].
The intensity of low back pain and the level of disability were considered the primary outcomes in the present study. An 11-point numeric pain scale ranging from 0 (no pain) to 10 (worst possible pain) was used to assess the perception of low back pain intensity [29, 30]. Participants were instructed to report low back pain intensity for the last seven days.
The Roland Morris Disability Questionnaire was used to assess disability associated with low back pain. It consists of 24 items describing daily tasks that people have difficulty accomplishing due to back pain. The scores on this questionnaire range from 0 to 24 points, with higher values indicating greater disability [35, 36]. Participants were instructed to answer the questionnaire based on the last seven days.
The secondary outcomes were kinesiophobia and perceived overall effects after eight weeks. The Tampa Scale of Kinesiophobia [37] was used to assess the kinesiophobia of the participants, consisting of 17 questions that address pain and intensity of symptoms, with a total score ranging from 17 to 68 points. In addition, the Global Effect Perception Scale was used to assess the perception of the effect of the interventions, which is an 11-point scale ranging from
Possible adverse events were monitored during the intervention period. Adverse events included worsening health status or the appearance of musculoskeletal complaints related to the interventions. Adverse events were monitored weekly and obtained through a face-to-face interview with the EG and a call with the CG. Volunteers were asked to report any use of medication, visits to the doctor, changes in clinical status, acute illnesses, or the appearance of any symptoms.
All outcomes were measured at baseline and after eight weeks of intervention by a blinded evaluator unaware of participant allocation. All participants were instructed not to reveal which group they belonged to during reassessment.
Randomization and blinding
The randomization process occurred at the end of the baseline assessments. The participants were randomly allocated into the experimental group (EG) or control group (CG). Randomization was generated using the website https://www.randomizer.org/, and hidden allocation was obtained using a numerical code sequence. Both procedures were performed by an independent, blinded researcher who was not part of the study. In addition, the evaluators were also blinded to the allocation of participants and execution of the training protocol.
Data analysis
All statistical analyses were conducted considering the intention-to-treat principle. Participant characteristics were presented using descriptive statistics, with central tendency, dispersion, and frequency distribution measures.
Differences within and between groups and their respective confidence intervals (95% CI) were calculated using Generalized Estimating Equations (GEE) models, considering the factors group, time, and the interaction group and time. Bonferroni’s post hoc was used to perform multiple comparisons when differences were detected. The assumption of normality of the residuals was evaluated by Q-Q plot analysis.
The Mann-Whitney test was used to compare the two groups (CG and EG) about the results of the Global Effect Perception Scale. Mean differences and 95% confidence intervals, as well as the interpretation of the clinical significance of the results were analyzed, adopting a significance level of 5%.
Statistical procedures were performed by a blind researcher using the SPSS version 22 software program (IBM Corp., Armonk, NY, USA).
Results
The first recruitment phase was completed in September 2020, and the second in January 2021. The intervention period for the first phase was between October and December 2020, and between January and March 2021 for the second phase. It was necessary to carry out two entries, given the many farm layoffs due to the COVID-19 pandemic.
A total of 90 workers were initially evaluated. However, only 63 were randomized into the experimental and control groups. Finally, 44 participants effectively participated in the study and received the intervention. The assessment, allocation, reassessment, and analysis processes are shown in Fig. 1.
Descriptive characteristics of participants at the baseline
Descriptive characteristics of participants at the baseline
Flowchart of participants throughout the study.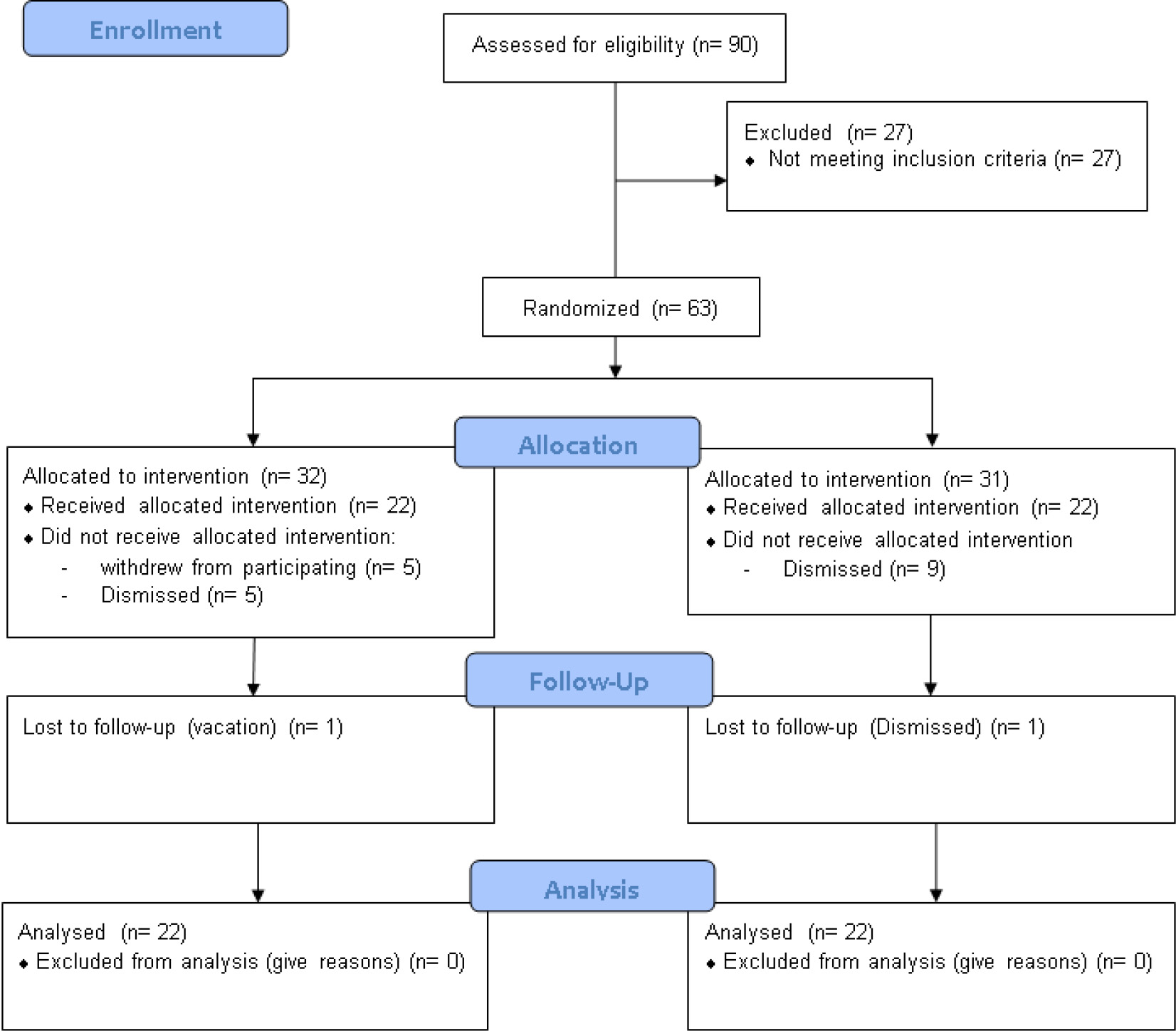
The sample consisted of 32 women (72.7%) and 12 men (27.3%), with a mean age of 37 years, body mass of 72.71 kilograms, a height of 1.62 meters, Body Mass Index of 27.68 and mean of pain of 6.79 points on the Numerical Pain Scale. Descriptive characteristics of participants in the total sample and stratified by group are presented in Table 1.
Mean (SD) for continuous outcomes at all study visits for each group, mean (SD) difference within groups, and mean (95% CI) difference between groups
Shaded areas indicate a statistically significant difference (
Table 2 presents the mean values, standard deviation, and differences within and between groups for pain intensity, disability, kinesiophobia, and Global Perceived Effect. The results indicated that pain and disability symptoms improved with both interventions (
No differences were found between groups (
This randomized clinical trial aimed to evaluate the effect of a resistance and stretching exercise program on pain intensity and function of the lumbar spine in fruit farming workers in the São Francisco Valley. The results found in this study demonstrated that both groups presented similar changes in the reduction of low back pain intensity and disability after eight weeks of intervention, with no significant differences between groups. Thus, it was possible to observe that supervised exercise in the work environment was not superior to orientation for carrying out exercises through a booklet in the home environment, rejecting our initial hypothesis.
A recent Cochrane systematic review of 249 studies [39] concluded that physical exercise is more effective in treating chronic low back pain, significantly reducing pain symptoms and functional limitations compared with no treatment, usual care, or placebo. On the contrary, our results demonstrated that the group that performed the supervised exercise program at the workplace did not present better results than the control group. However, our control group reported having completed the structured program of stretching exercises performed at home. In this sense, both groups may have benefited from the practice of exercises, considering that the literature recognizes that the different types or modalities of exercises have positive effects in managing musculoskeletal pain through different mechanisms [39].
Resistance exercises in the case of the experimental group may have resulted in increased muscle strength and function, gain in the range of motion, and improved neuromuscular control and stabilization. In addition to the physical benefits, the workers may have benefited from the emotional and psychological effects of physical exercise, which are strongly associated with improving pain and disability [39]. Furthermore, resistance exercise may have reduced pain perception, as it contributes to activating central pain inhibition and modulation mechanisms, increasing the concentration of
These findings seem to corroborate the conclusions of Bernardelli et al. [44], who observed that a regular physical exercise program at home or the workplace was equally effective in improving disability and kinesiophobia related to low back pain in workers with low back pain. In this context, training guidelines for a home exercise program can be promising in improving outcomes related to low back pain, which are less costly for the company in terms of lost work hours and are more cost-effective [44].
On the other hand, Jakobsen et al. [45, 46] demonstrated that ten weeks of supervised physical exercise at work was more effective than home exercises for reducing the intensity of low back pain in health professionals. However, methodological differences such as the characteristics of the workers and their work demands, the duration of the intervention, and the lack of monitoring of the home group explain the divergence in the results. In addition, whether there was a control or selection of volunteers about the initial intensity of pain and duration (acute or chronic) was not reported. These factors directly influence the size of the effect observed for the outcomes of pain and disability since most episodes of acute low back pain have a favorable course, with resolution within 6 to 8 weeks, even in the absence of active treatment [47]. The conclusion of previous studies [45, 46, 47] indicating the superiority of exercises performed in the workplace is based on statistical differences (difference between groups of 0.7 [CI95%
The decrease in the intensity of low back pain observed in the present study in both the experimental group of 4.55 points, and in the control group of 3.81 points, is above the established value for a minimal important clinical difference (MICD) for chronic low back pain, which is 1.7 points [31]. Similarly, a decrease of 4.45 points was observed for disability in the experimental group and 4.43 points in the control group assessed by the Roland-Morris questionnaire, with these reductions being greater than the MICD of this instrument, which is 3.5 points [48]. The reduction of pain and incapacity of the lumbar region in both groups above the predetermined MICD values [31] is confirmed by the volunteers’ Global Perceived Effect (GPE). Although no significant differences were observed between the experimental and control groups in the analysis of the workers” GPE, both reported mean values greater than three points, close to the upper limit of “total recovery” indicated by the scale, which is five points. These data have a meaningful clinical significance, as none of the workers reported worsening the clinical condition throughout the intervention, and almost half of the assessed sample reported feeling fully recovered.
Another relevant aspect to be analyzed regarding low back pain concerns kinesiophobia due to its relationship with disability and the perpetuation of symptoms. Lack of activity due to fear of movement can induce changes in muscle tropism and function and worsen symptoms [49]. When analyzing the Tampa Scale of Kinesiophobia (TSK) score, no significant difference was found between time and group. The results in the literature are divergent regarding the effects of different exercise modalities on kinesiophobia [49, 50, 51, 52]. However, our findings corroborate studies which evaluated more physically active participants with lower indicators of kinesiophobia in the baseline assessment [50, 51, 52]. This finding can be explained by the fact that even with a pain level above three points on the Numerical Pain Scale, all workers continued their activities normally on the grape farm. Gregg et al. [53] found that the changes in TSK scores after a rehabilitation program in patients with low back pain did not strongly correlate with pain scores, functional levels, or return to work results. Therefore, constructs such as kinesiophobia may or may not develop regardless of the intensity of symptoms and perceived disability.
Finally, the scarcity of clinical trials with intervention in the work environment involving fruit workers makes this study very relevant. However, the results of this study have some limitations. Our small, even though significant sample size and participant characteristics made it challenging to analyze possible moderating effects, such as gender differences. This fact is related to many layoffs due to the COVID-19 pandemic and the fear of employees that involvement in the intervention could harm productivity. Another limitation was using subjective instruments that required the participants’ recall to be answered, which could lead to a memory bias.
The clinical relevance of the current findings is that eight weeks of supervised exercise at the workplace do not offer different results in reducing the low back pain intensity or disability in fruit workers compared to home exercise guidelines using booklets. Future studies should be carried out to investigate whether a particular exercise modality is more effective than another in reducing low back pain and disability. In addition, it should be explored whether some interventions with exercise would be superior among workers with different occupational activities.
Conclusions
The results of the present study demonstrate that the intervention with a physical exercise program performed in the work environment was not superior to the intervention with home exercises guided by a self-explanatory booklet. However, both interventions showed important clinical improvements in pain intensity and disability. These findings reinforce that employers can use both strategies to mitigate the impact of low back pain on the health and functional and work performance of fruit workers.
Funding
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) – Finance Code 001.
Author contributions
Conceptualization, M.H.P.P., S.P.B.P., G.A.B., A.C.R.P., R.C.A.; formal analysis, M.H.P.P., S.P.B.P., G.A.B., A.C.R.P., R.C.A.; investigation, M.H.P.P., S.P.B.P., V.Y.S.N., F.A.S.O.; data curation, M.H.P.P., S.P.B.P., V.Y.S.N., F.A.S.O.; writing – original draft preparation, M.H.P.P., V.Y.S.N.; writing – review and editing, F.L., A.C.R.P., R.C.A.; supervision, F.L., R.C.A.; project administration, A.C.R.P., R.C.A.; All authors have read and agreed to the published version of the manuscript.
Ethical considerations
This study was approved by the Research Ethics Committee of the University of Pernambuco (protocol CAAE 17386919.6.0000.5207).
Informed consent
All participants read and signed the consent form, which contained all information regarding the study.
Data availability statement
The data supporting this study’s findings are available on request from the corresponding author.
Supplementary data
The supplementary files are available to download from
Footnotes
Acknowledgments
The authors would like to thank the workers and management of the farms where the study was conducted.
Conflict of interest
The authors declare no conflicts of interest.