
Abstract
BACKGROUND:
Joint position reproduction measures the angle acuity of reference angle reproduction using an indicator angle. However, reference angles are often not available.
OBJECTIVE:
This study aimed to examine joint position sense at three different targeted joint angles, which were estimated from the maximum range of motion (maxROM) without a reference angle at each targeted joint angle.
METHODS:
The maxROM was measured in straight leg raise (SLR) and active knee extension (AKE) positions. In both positions, a targeted joint angle at 75% of the maxROM was assessed first, followed by that at 50% and 25% of the maxROM. A one-sample t-test was used to analyze differences between the targeted and reproduced angles in both positions.
RESULTS:
All reproduced angles significantly differed from the targeted angle in both SLR and AKE positions except for the reproduced angle measured at 75% maxROM. Overall, position errors in the AKE position were higher than those in the SLR position.
CONCLUSIONS:
Estimating the angle based on the maxROM without a matched reference angle may lead to significant discrepancies in comparison with the targeted joint angle. In clinical settings, if accurate reproduction of motions is required to improve proprioception, providing a reference angle might be helpful.
Introduction
The lower extremity frequently undergoes rapid axial rotation; hence, it is vulnerable to sports injuries [1, 2]. Identifying risk factors for sports injuries is likely to be of clinical significance [3]. Proprioception is defined as a sense of joint position, joint movement, and force, and poor proprioception is a modifiable risk factor in relation to sports injuries [4, 5]. Individuals with ankle instability have been reported to show deficits in joint position recognition and larger errors in passive joint positioning than those without ankle instability [6, 7]. Moreover, in a study involving American Football League players, those who had suffered hamstring injuries displayed a diminished sense of movement compared to their uninjured counterparts, underscoring the importance of proprioceptive function in physical rehabilitation [8]. It is established that stretching, a common component of sports training, also enhances joint position sense [9]. Various sub-modalities of proprioceptors, found in muscles, tendons, ligaments, joints, and skin, detect information related to motion, direction, acceleration, and deceleration [10, 11]. Notably, proprioceptors like Ruffini endings and Pacinian corpuscles, located in joint capsules and skin, perceive tissue stretching during movement and contribute to determining joint position [12].
Subject demographics
Subject demographics
Among the various methods available to measure proprioception, joint position reproduction (JPS) has emerged as a preferred method [4]. JPS involves placing one extremity at a designated joint angle (referred to as the reference angle) and reproducing the same angle with the contralateral extremity (referred to as the indicator angle) [13]. In general, active joint positioning, where the patient independently positions the joint without support, tends to have higher accuracy compared to passive joint positioning, where the examiner controls the patient’s motion [14]. However, it’s important to recognize that JPS primarily measures the accuracy of recognizing and reproducing the reference angle, rather than assessing movements performed during everyday activities or sports [15, 16]. Therefore, it is necessary to go beyond simply measuring JPS and instead, become aware of one’s maximum flexibility and use it as a basis to accurately determine how well one can perform the desired muscle performance [17]. Previously, we measured three different submaximal forces without matched reference forces. Based on 100% of measuring maximum voluntary contraction (MVC), three different submaximal intensities (75%, 50%, and 25% of the MVC) were estimated, and contraction intensities were measured, respectively [18, 19]. We noted that under- and over-contraction were observed at high and low targeted intensity, respectively, suggesting that reference force may affect the sense of force.
This study aimed to examine joint position sense at three different targeted joint angles estimated from the maximum range of motion (maxROM), without providing a reference angle for each targeted joint angle. Joint position sense was determined in two different positions, namely, straight leg raise (SLR) and active knee extension (AKE) positions.
Subjects
The study subjects were 29 healthy adults (Table 1). Individuals who had musculoskeletal or neurological disorders or had undergone surgery on the lower extremity in the last 6 months were excluded [20]. This study was approved by the Institutional Review Board of Woosong University, and written informed consent was obtained from all participants.
Procedures
The participants were instructed to lie in a supine position on a treatment table. The measured lower extremity was randomly assigned, and the contralateral lower extremity was fixed with a strap. The measured lower extremity underwent a SLR in full knee extension in accordance with the examiner’s instructions. At maxROM, the participants were asked to hold the posture for approximately three seconds for the examiner to make measurements. This step was repeated twice, and the mean value was recorded as the maxROM. After a short rest, the participants flexed the hip to the targeted joint angles (75%, 50%, and 25% of the maxROM), which were estimated based on the maxROM. The measured hip flexion angle at each targeted joint angle was recorded as the reproduced angle of hip.
After completing all of the measurements in the SLR position and resting for a sufficient amount of time, AKE was performed. In the AKE position, the measured leg and the unmeasured contralateral leg in the SLR were assigned as the non-measured and measured sides, respectively. The non-measured lower extremity was fixed with a strap. In a relaxed state, the examiner induced 90
Reproduced joint angles at three different targeted joint angles and normalized to the maxROM (%maxROM)
Reproduced joint angles at three different targeted joint angles and normalized to the maxROM (%maxROM)
maxROM, maximum range of motion
Hip (a) and knee (b) range of motion measurements using a clinometer.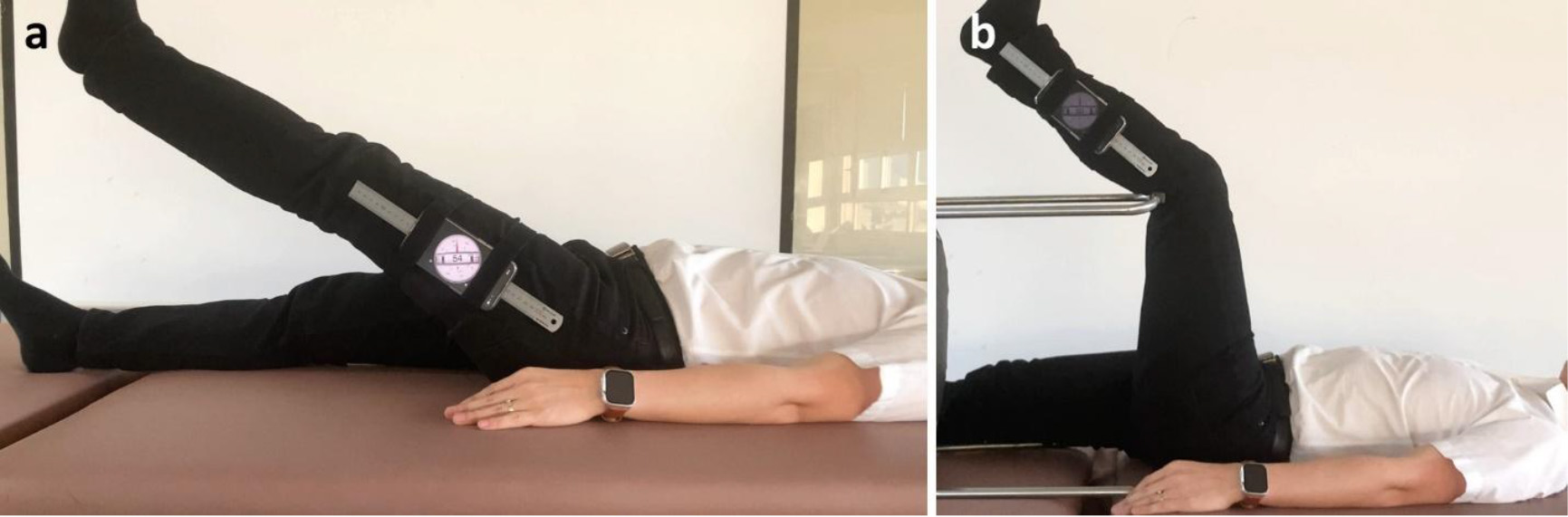
In accordance with prior researches, measurements were taken at 75%, 50%, and 25% of maxROM [18, 19]. A targeted joint angle at 75% of the maxROM was assessed first, followed by that at 50% and 25% of the maxROM in both positions. During the intervention, the participants were not blinded; however, they were instructed to keep their head up straight to prevent them from observing their lower extremity motions. Joint ROM was measured using a clinometer application (Plaincode Software Solutions, Stephanskirchen, Germany) installed on an iPhone 11 (Apple Inc, Cupertino, CA, USA) [21]. The smartphone with a metal rod attached was placed at the midpoint between the greater trochanter and the lateral femoral condyle in the SLR position (Fig. 1a) and at the midpoint between the lateral epicondyle of the femur and the lateral malleolus in the AKE position (Fig. 1b) [22, 23, 24].
Data normality was assessed using a Shapiro-Wilk test. A one-sample
Results
In the SLR position, reproduced angles at 50% and 25% of the maxROM were significantly higher than targeted angles, respectively (
The difference between the targeted angle and the reproduced angle in the straight leg raise position.ROM, range of motion.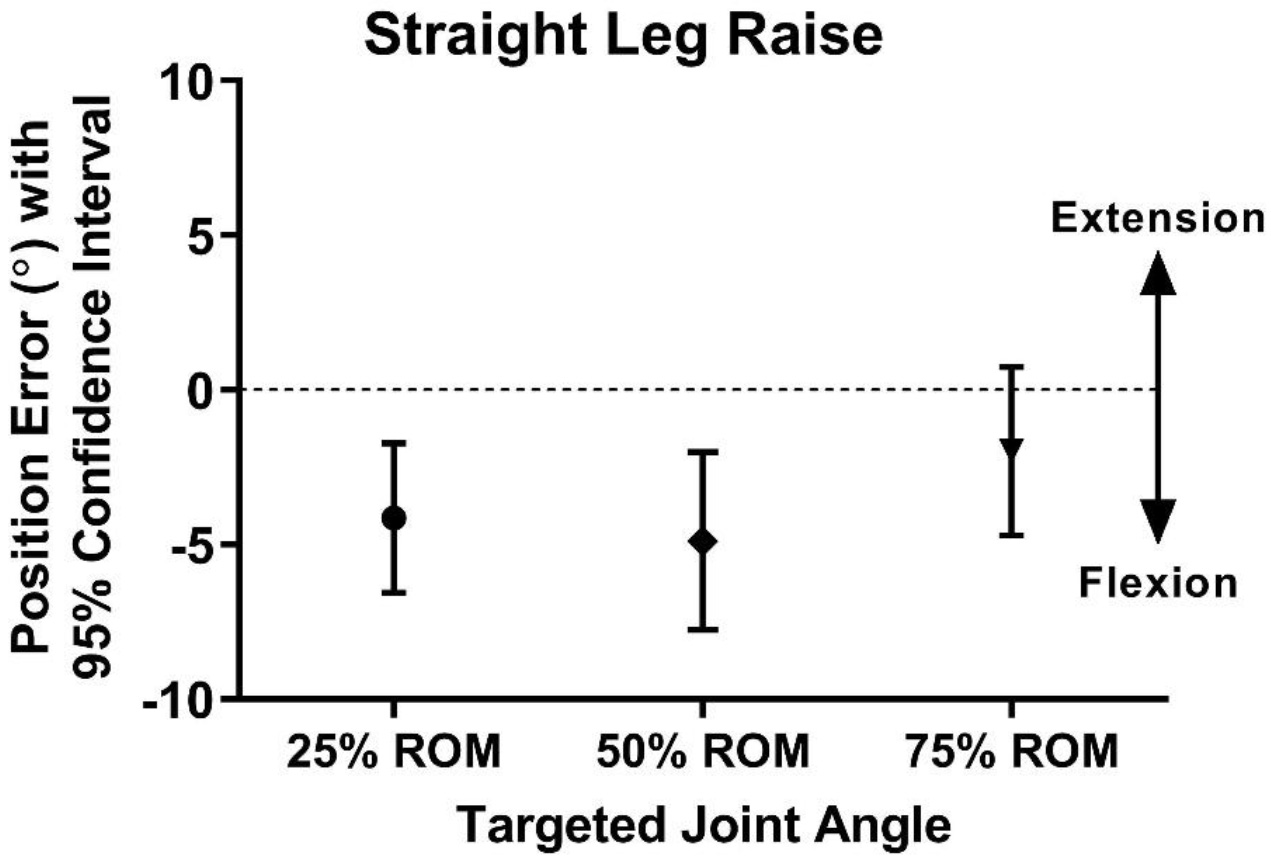
The difference between the targeted angle and the reproduced angle in the active knee extension position.ROM, range of motion.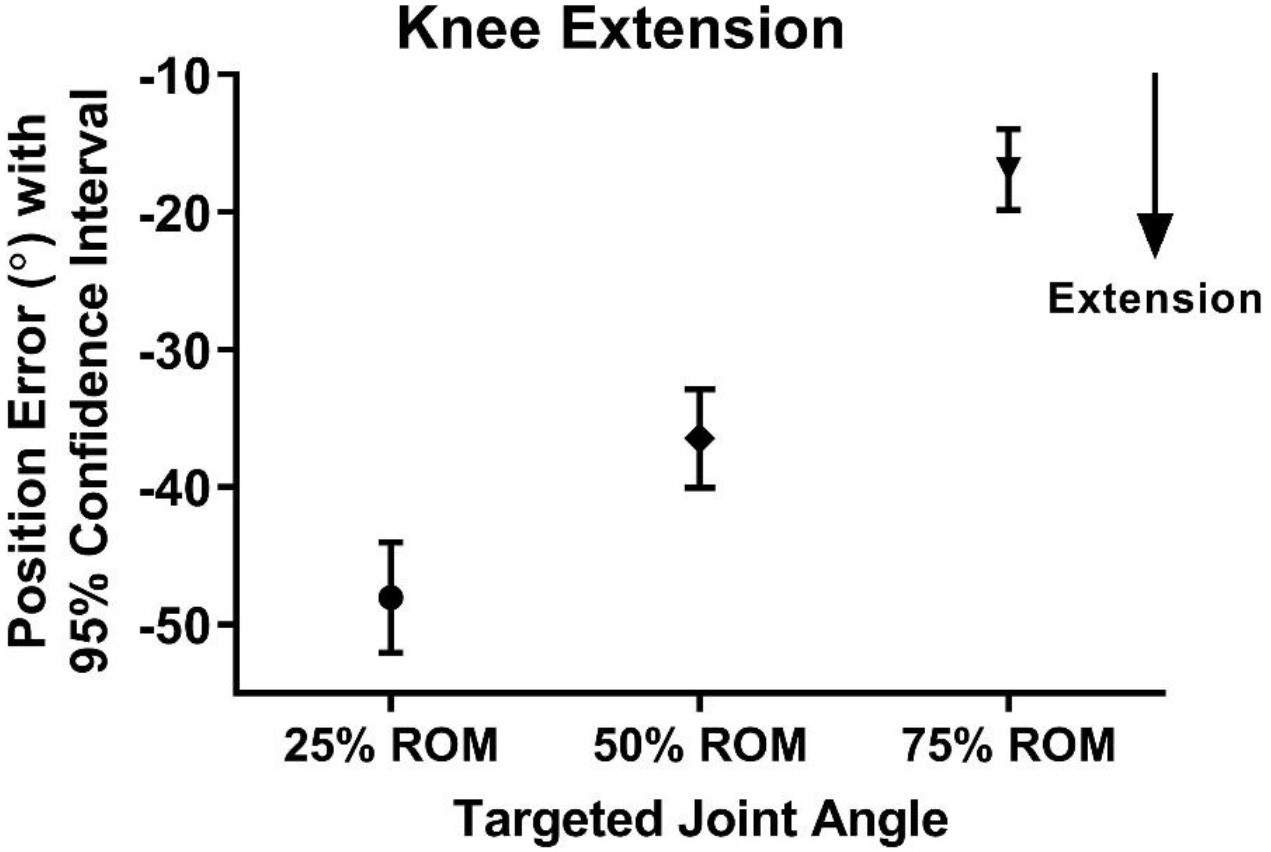
The difference between the targeted angle and the reproduced angle in modified active knee extension position.ROM, range of motion.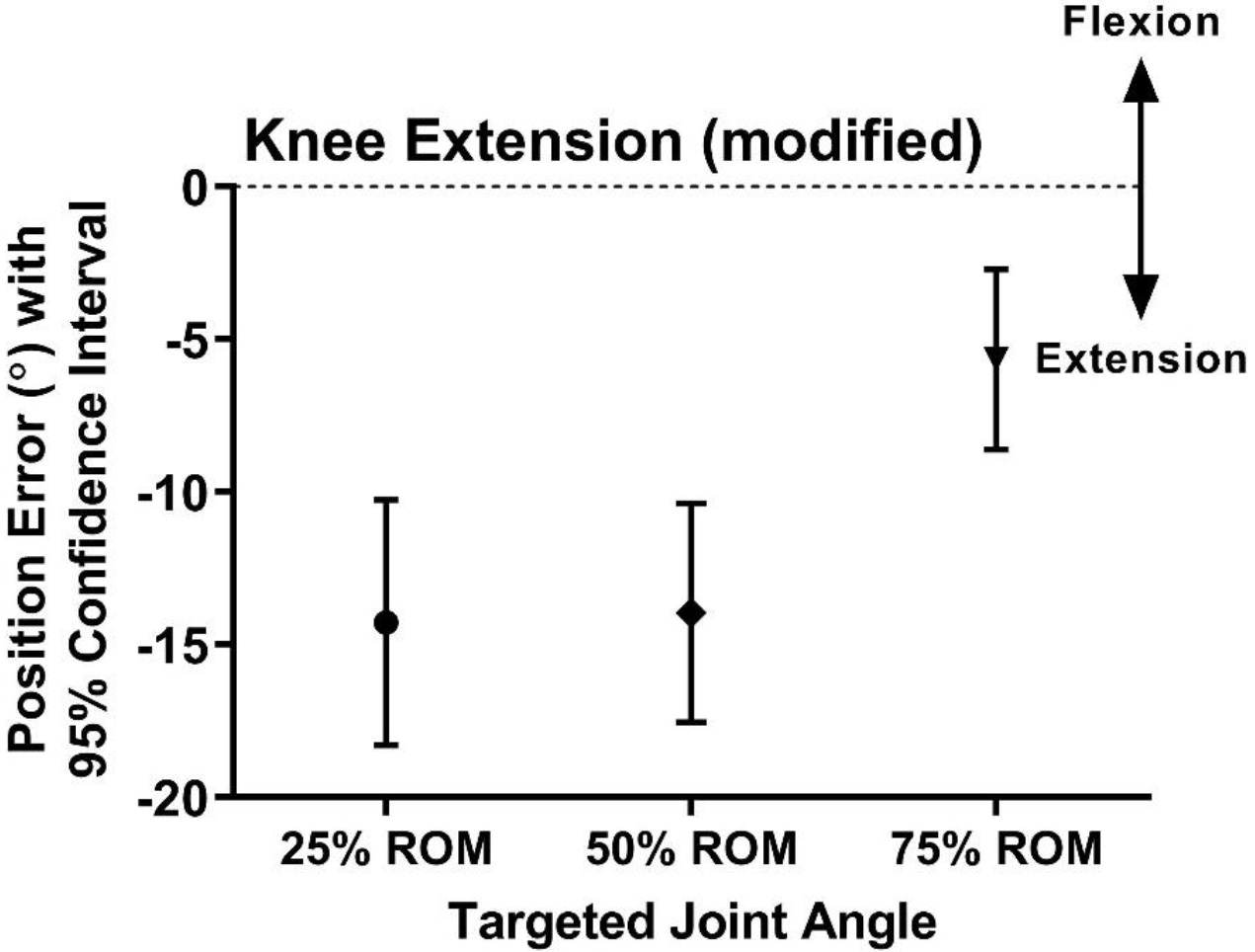
In the AKE position, reproduced angles at 75%, 50%, and 25% of the maxROM were significantly higher than the targeted angle, respectively (
The objective of this study was to assess joint position sense at three different targeted joint angles derived from the maxROM, without offering a reference angle for each targeted joint angle. Joint position sense was evaluated in two distinct positions (SLR and AKE positions).
In the SLR position, the reproduced joint angle at 75% of the maxROM was 2.0
In the AKE position, the reproduced joint angle at 75%, 50%, and 25% of the maxROM was 16.9
This aligns with the understanding that proximal joints generally possess superior proprioception compared to distal joints [28, 29]. Moreover, in the context of joint position reproduction (JPR), it is a recognized fact that joint position error tends to be more pronounced in the knee as opposed to the hip [30]. The plausible explanation for this observation may be linked to the higher muscle activity required during hip motion. Muscle activity governing both the upper and lower legs is likely higher than that which solely controls the lower legs. As a result, the effort required to maintain the position increases, contributing to a reduction in joint position error [22]. Furthermore, in the SLR position, the starting position is at 0
In both positions, estimating the targeted joint angle based on the maxROM without a reference angle lowered position sense acuity. In particular, compared with the hip joint, the knee joint showed greater position error. However, these findings cannot be used to conclude that the knee joint has poor proprioceptive function compared with the hip joint. Proprioception is achieved through a complex interaction of physiological and psychological processes [42, 43], and sensory input, central procession, and motor output must be involved appropriately in a closed loop. Given this, currently available methods do not fully represent proprioception. Instead, they only show partial characteristics of proprioception. In addition to active JPR, active movement extent discrimination assessment is commonly used to evaluate proprioception; however, these two methods often show significant differences in results under identical conditions [44].
This study had limitations. The limited number of participants and the exclusive focus on healthy adults in this study may impose limitations on generalizing the results. In addition, the sequence of the presented targeted joint angles may have affected the results. In another study that measured perceived pain intensity, a gradual increase in the targeted joint angle from 25% to 75% of the maxROM led to no changes in perceived pain. However, when the targeted joint angle was gradually decreased from 75% to 25% of the maxROM, perceived pain tended to decrease [31]. Therefore, in future studies, the sequence of the three targeted joint angles needs to be randomized to minimize such effects.
Conclusions
Unlike the sense of force, estimating the targeted joint angle based only on the maxROM without a reference angle decreased position sense acuity. Overall, position errors in the AKE position were higher than those in the SLR position. Consequently, providing reference angles or guidance during active motion can be beneficial in enhancing the precision of motion reproductions.
Author contributions
Wootaek Lim: Conceptualization, Methodology, Validation, Formal analysis, Investigation, Resources, Data Curation, Writing, Visualization, Funding acquisition.
Data availability statement
Not applicable.
Ethical approval
This study was approved by the Institutional Review Board of Woosong University (1041549-221011-SB-149).
Funding
This research was supported by 2022 Woosong University Academic Research Funding.
Informed consent
Informed consent was obtained from subjects prior to their participation.
Footnotes
Acknowledgments
The author has no acknowledgments.
Conflict of interest
The author has no conflicts of interest to report.