
Abstract
BACKGROUND:
Osteoporosis is the most common disease in postmenopausal women and the elderly, which can lead to vertebral compression fracture.
OBJECTIVE:
To investigate the related factors of severe osteoporotic vertebral compression fracture (SOVCF) and evaluate the long-term outcomes of percutaneous kyphoplasty (PKP) for treating SOVCF through comparison with mild OVCF (MOVCF).
METHODS:
From September 2015 to March 2019, 294 osteoporotic vertebral compression fracture (OVCF) patients treated with PKP were analyzed. Compression of the anterior margin of the fractured vertebral body beyond 2/3 of the original height was defined as SOVCF. Baseline data, clinical and imaging findings before and after surgery and at the last follow-up were recorded. Numerical Rating Scale (NRS) was used to evaluate low back pain, the Oswestry Disability Index (ODI) was used to evaluate activity of daily life. Anterior vertebral height (AVH) and local kyphosis angle (LKA) was used to evaluate radiographic outcomes. During the follow-up, patients with recurrent back pain were examined by MRI to identify new fractures and the incidence of adjacent vertebral fracture (AVF) was recorded. Age, sex, body mass index (BMI), dual energy X-ray absorptiometry based T value, duration of symptom, history of trauma, steroid use, and fracture site were collected for univariate logistic regression analysis Variables with a
RESULTS:
Logistic regression analysis indicated that longer duration of symptom (OR
CONCLUSION:
Lower
Introduction
Osteoporosis is the most common disease in postmenopausal women and the elderly and can lead to vertebral compression fracture, which not only causes severe pain and reduced mobility, but also increases the disability rate and mortality of patients, thereby bringing economic burden to families and society [1]. Most osteoporotic vertebral compression fracture (OVCF) patients only suffer local pain which can be relieved by staying in bed, external fixation using braces, and anti-osteoporosis treatments. If the conservative treatment for OVCF with intractable pain is failed, percutaneous kyphoplasty (PKP) is the most common surgical procedure [2]. Compared with percutaneous vertebroplasty (PVP), PKP can better restore vertebra height and reduce cement leakage through balloon dilatation [3, 4]. Svedbom et al. performed a cost-effectiveness analysis of hospitalized acute OVCF patients, and revealed that PKP had at least 60% likelihood of being cost-effectiveness compared with conservative and PVP treatments [4]. In addiiton, a small group of OVCF patients suffer severe OVCF (SOVCF) with severe collapse of vertebral body. The clinical manifestations of SOVCF are varied, including acute pain, organ compression caused by kyphotic deformity, and chronic fatigue pain caused by sagittal imbalance [5]. SOVCF is usually complicated with multiple medical conditions and severe oeteoporosis, and conservative treatment is ineffective [6]. Although invasive surgery can improve kyphotic deformity by restoring vertebral height, the incidence of internal fixation-related complications is high [7]. Due to the limited vertebral height, percutaneous vertebral augmentation techniques are difficult to perform, and have a high cement leakage rate [8]. However, so far, percutaneous vertebral augmentation is still the most commonly used procedure due to its minimally invasive nature [9].
Few studies have reported on comparing clinical efficacy of PKP for SOVCF with that of PKP for mild OVCF (MOVCF). Additionally, factors associated with the development of SOVCF are also unknown. Since the clinical manifestations of SOVCF is complex, and the therapeutic effect is uncertain, it is of great significance to explore its related factors, which might provide reference for subsequent prevention and treatment in the future. Therefore, this retrospective study aimed to investigate the related factors of SOVCF, and evaluate the long-term clinical outcomes, imaging results, and complications of PKP in treating SOVCF via comparing with those in treating MOVCF.
Materials and methods
Patients
The institutional review board of Xuzhou Central Hospital approved this retrospective study. A total of 490 patients with OVCF undertaking PKP from September 2015 to March 2019 in our hospital were included.
Inclusion criteria: (1) dual energy X-ray absorptiometry (DEXA) showed bone mineral density T value
Exclusion criteria: (1) patients suffered non-osteo-porotic spinal fractures caused by tumor, inflammation, violence, etc.; (2) patients had comorbid nerve injury; (3) patients were diagnosed with multiple OVCF; (4) patients were follwed up without enough time or not fllowed up; (5) patients suffered severe internal diseases or psychoneurotic abnormalities, so that they were unable to follow-up.
According to the previous criteria [5], patients with anterior vertebral height (AVH) compression exceeding 2/3 of the original vertebral height were diagnosed with SOVCF. OVCF patients were divided into the SOVCF and MOVCF groups according to the degree of vertebral compression.
Surgical procedure
All procedures were performed under local anesthesia and in the prone position, and their spines were extended by chest and pelvic bolsters. First, anteroposterior view of fluoroscopy was performed to identify the fractured vertebra. Second, the distance between the needle insertion point and the midline was measured according to the preoperative CT or MRI, and the insertion point on the skin was marked. Third, 1% lidocaine was used from the skin to the junction between the upper facet base and the transverse process, and a guide needle entered the vertebra through this site. Fourth, the trocar was implanted when the guide needle entered into the anterior one-third of the vertebra confirmed by the lateral view; at the same time, in the anteroposterior view, the needle exceeded the center of the vertebral body; then a balloon was placed under fluoroscopy to dilate the compressed vertebra; fianlly, the balloon was removed and bone cement was injected through the trocar. Last but not least, after the bone cement was dried and fixed, the trocar was removed, and the puncture site was wrapped with sterile dressing.
The criteria for stopping bone cement injection were as follows: 1) lateral fluoroscopy showed that the bone cement filled the anterior three-quarter of vertebra, and anteroposterior view showed that bone cement touched or exceeded the bilateral pedicles; 2) lateral fluoroscopy showed that the bone cement exceeded the posterior 1/4 of vertebra, with the risk of involvement of the spinal canal or foramen; 3) bone cement leakage with unstoppable trend after waiting for about 1 minute.
Postoperative treatment
Patients in both SOVCF and MOVCF groups were allowed to get out of bed 6 hours after surgery, and did moderate lumbar and back muscle function exercise. X-ray examinations were conducted before discharge. After discharge, osteoporosis-related knowledge was given along with long-term oral anti-osteoporosis drugs. Outpatient and/or telephone follow-up were performed every 3 months after discharge.
The measurement method diagram of local kyphosis angle (LKA) and anterior vertebral height (AVH).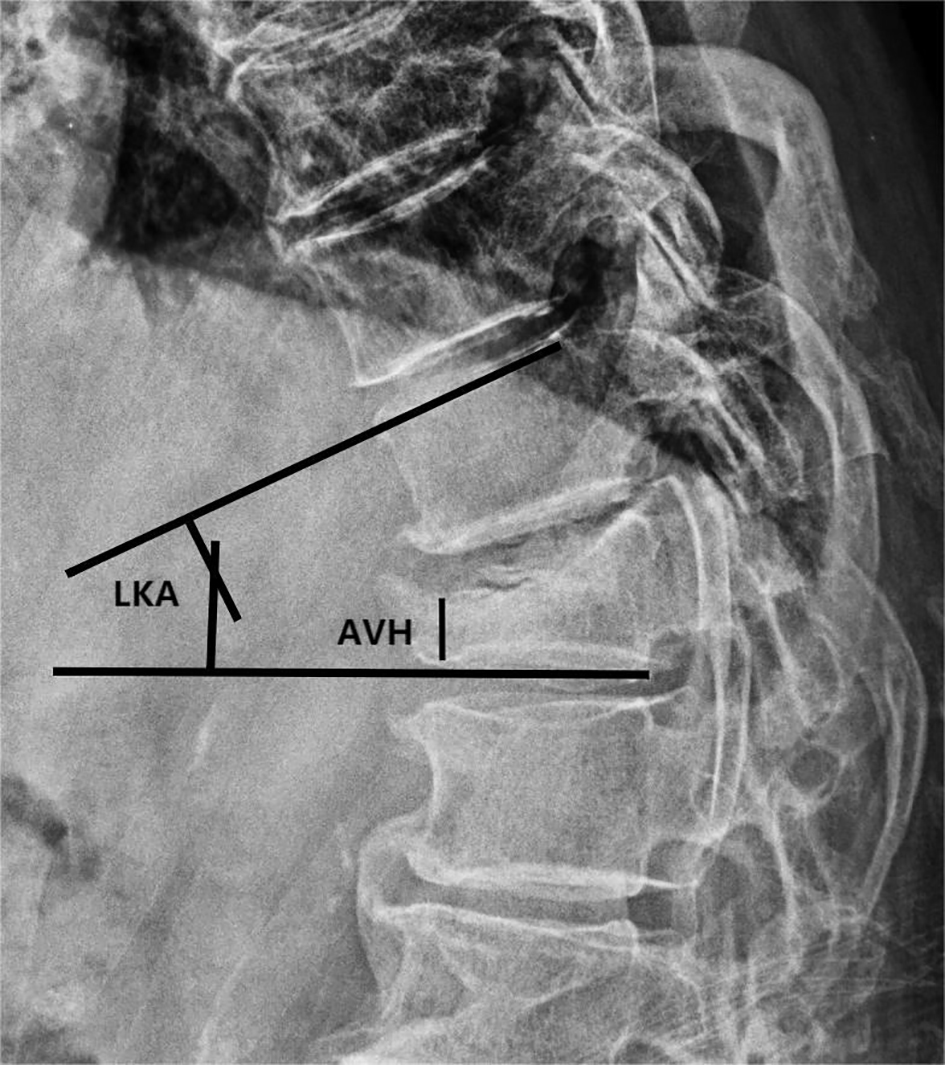
General information
General information was collected, including age, gender, duration of disease, steroid use (i.e., exceeding physiological dose of steroid for more than 90 days), history of trauma, body mass index (BMI, kg/m2),
Clinical results
Pain evaluation: We recorded preoperative and postoperative Numerical Rating Scale (NRS) scores [10], and back pain during the follow-up back, in which 0 point indicated no pain and 10 points indicated the most severe pain.
Functional evaluation: We recorded preoperative, postoperative, and follow-up Oswestry Disability Index (ODI). ODI is consisting of 10 questions, there are 6 options for each question, and 0 point is scored for the first choice and 5 points for the last choice. The total score of ODI
Imaging examination
X-ray, 2D-CT and MRI were performed before operation. X-rays were conducted again after operation and at the last follow-up. All imaging data were analyzed by two senior physicians (Xue and Zhang) to make a diagnosis of MOVCF or SOVCF. The relevant parameters were measured, and the results were averaged between the two authors. The detailed measurement methods are shown in Fig. 1.
AVH: The distance between the upper and lower endplate of the anterior edge of the fractured vertebra in the lateral X-ray view.
Local kyphosis angle (LKA): In the lateral X-ray view, if the fracture was located at the upper part of the vertebra, the angle between the upper endplate of the vertebra above the fractured vertebra and the lower endplate of the injured vertebra was measured. If the fracture was located at the lower part of the vertebra, the angle between the upper endplate of the fractured vertebra and the lower endplate of the lower vertebra was meausred. If the fracture involved the upper and lower endplates, the angle between the upper endplate of the vertebra above the fractured vertebra and the lower endplate of the vertebra below the fractured vertebra was meausred.
A 61-year-old woman presented with lumbar and back pain without obvious cause 7 days before visiting our hospital. Preoperative X-ray (A and B) and lumbar MRI (C) indicated compression fracture of L2 vertebra. Percutaneous kyphoplasty (PKP) surgery was performed under local anesthesia. Postoperative X-ray (D and E) showed that vertebral height recovered, and bone cement filled adequately without leakage. At the last follow-up (42 months after surgery), X-ray (F and G) showed no significant change in vertebral height, and the bone cement remained in place.
A 69-year-old woman presented with low lumbar and back pain after fall to the ground 3 months before visiting our hospital. Preoperative X-ray (A and B) and lumbar MRI (C) indicated compression fracture of T12 vertebra. Percutaneous kyphoplasty (PKP) surgery was performed under local anesthesia. Postoperative X-ray (D and E) suggested no significant recovery of vertebral height, and leakage of bone cement in both upper and lower vertebral spaces. Lumbar back pain recurred 8 months after surgery. Lumbar MRI (F) reexamination revealed a compression fracture of L1 vertebra. PKP surgery (G and H) was performed again under local anesthesia.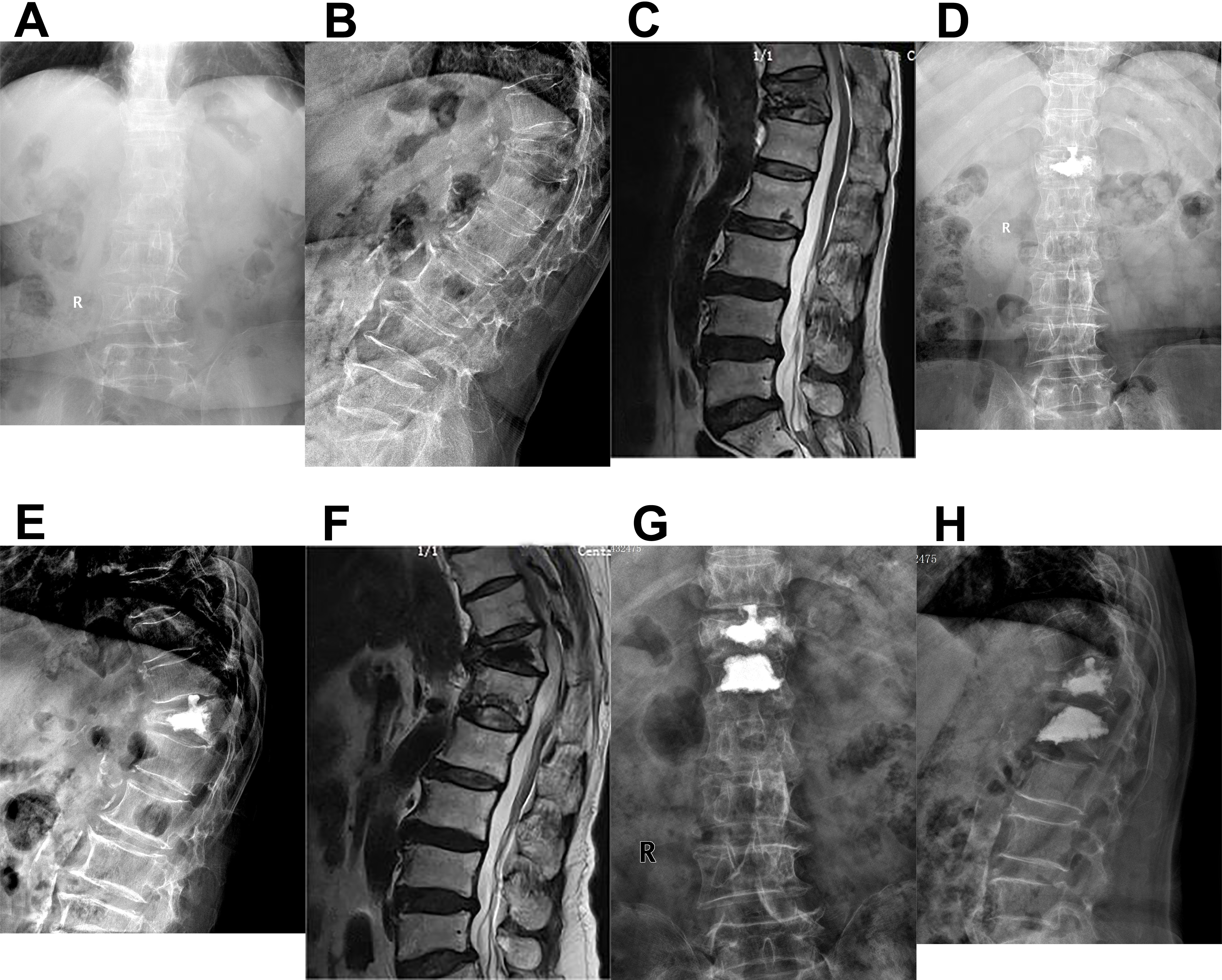
Loss of correction: Calculated at the last follow-up and expressed as the LKA at the last follow-up minus the postoperative LKA.
Patients with recurrent back pain during the follow-up was re-examined by MRI to confirm new fracture, and the incidence of adjacent vertebral fracture was recorded.
Continuous variables were expressed as mean
Based on our clinical experience and previous studies, age, sex, BMI, dual energy X-ray absorptiometry based
Results
General information
There were 43 cases in the SOVCF group, including 10 males (23.26%) with an average age of 72.5 years. The average duration of symptom was 50 days. The average BMI and
There were 251 cases in the MOVCF group, including 47 males (18.73%) with an average age of 72.9 years old. The average duration of symptom was 18 days. The average BMI and T value were 23.23 kg/m2 and
Univariate analysis of demographic data between the two groups
Univariate analysis of demographic data between the two groups
SOVCF: severe osteoporotic vertebral compression fracture, MOVCF: mild osteoporotic vertebral compression fracture, BMI: body mass index.
Multivariate Logistic regression analysis of the factors related to SOVCF
SOVCF: severe osteoporotic vertebral compression fracture, BMI: body mass index, BMD: bone mineral density.
Univariate analysis suggested no differences in age, gender, BMI, and the history of trauma between SOVCF and MOVCF groups (Table 1). Differences were found in the duration of symptom,
Comparison of imaging examination results before and after operation and at the last follow-up
Comparison of imaging examination results before and after operation and at the last follow-up
Osteoporosis compressive fracture, MOVCF: mild osteoporosis compressive fractures, LKA: local kyphosis angle, AVH: anterior vertebral height.
Compared with the MOVCF group, the SOVCF group had significantly higher LKA and lower AVH before and after surgery, and at the last follow-up. Compared with preoperative results, AVH significantly increased, and LKA significantly decreased in both groups after surgery and at the last follow-up. At the last follow-up, degree of loss of correction in the SOVCF group was significantly higher than that in the MOVCF group (6.47
Comparison of clinical examination results before and after operation and at the last follow-up
Comparison of clinical examination results before and after operation and at the last follow-up
NRS: numerical rating scale, ODI: Oswestry Disability Index, SOVCF: severe osteoporosis compressive fracture, MOVCF: mild osteoporosis compressive fractures.
The operation time, radiation exposure, bone cement leakage rate and adjacent vertebral fracture rate was compared between the two groups
SOVCF: severe osteoporosis compressive fracture, MOVCF: mild osteoporosis compressive fractures.
Compared with preoperative results, NRS and ODI significantly decreased in both groups after surgery and at the last follow-up. No significant differences were found in NRS and ODI at one week a fter surgery between the two groups. Compared with the MOVCF group, the SOVCF group had significantly higher NRS (2.28
Complications
There was significant difference in postoperative cement leakage rate between the SOVCF and MOVCF groups (55.81% vs 18.73%,
Discussion
Compared with MOVCF, SOVCF has more complicated symptoms, and more severe osteoporosis, which is more difficult to perform surgery with higher risks and poorer surgical outcomes [11]. In recent years, with the improvement of surgical techniques and filling materials, reports on vertebral augmentation surgery for SOVCF have gradually increased. Although the long-term outcome for SOVCF remains uncertain, this surgery is remarkably effective in relieving acute pain and early mobility [5].
The results indicated that the duration of symptom, lower T value, and steroid use were independent related factors of SOVCF. Some elderly patients with OVCF have no history of trauma, are insensitive to pain, only have mild symptoms of low back pain, and have abdominal distention and intercostal neuralgia as the first symptoms, so that the physicians are easy to misdiagnose as gastrointestinal diseases, thereby delaying the treatment [12]. In this study, the longest duration of symptom in the SOVCF group was 135 days due to no regular treatment in the early stage, and during these days, the fractured vertebra was continuously subjected to gravity load. In addition, OVCF patients always experienced osteoporosis, so that they often suffer slow healing of fractures and even nonunion. Thus, continuous reduction of vertebra height, and even linear vertebral compression happened in some cases.
Bone mineral density (BMD) is the most important indicator of osteoporosis, and previous studies have shown that the degree of osteoporosis is an independent related factor leading to OVCF and re-fracture after vertebral augmentation [13]. Osteoporosis can lead to loosen of the vertebral trabecular structure, and reduce the mechanical strength of the vertebrae.This study further verified roles of BMD in SOVCF, that was, the decreased BMD could result in a significant increase in the risk of SOVCF.
We found that steroid use was also a related factor of the occurrence of SOVCF. Steroids are widely used in clinical practice, but long-term use can trigger a series of dose-dependent adverse reactions, such as osteoporosis and muscle atrophy. In addition to acting directly on bone tissue cells and molecular signaling pathways, steroids also have impacts on the whole body, thereby indirectly affecting bone health. For example, steroids can reduce intestinal calcium absorption, and inhibit renal calcium reabsorption, which leads to negative calcium balance, therby affecting bone calcification. High-dose steroids cause bone loss and the increased risk of fractures by inhibiting gonadal function [14]. Proximal muscle weakness caused by muscular atrophy reduces stress stimulation on the bone, resulting in the decrease of bone strength, and a significant increase of the risk of fractures [15].
Another objective of this study was to compare the clinical efficacy of PKP in the treatment of MOVCF and SOVCF. OVCF patients in previous studies might include some SOVCF patients, while our study clearly divided the cases into the SOVCF and MOVCF groups according to the imaging diagnostic criteria, and compared the effects and complications of PKP treatment for SOVCF and MOVCF at the same time, which is rarely reported in similar studies in the past. The results showed no significant differences in pain relief and functional recovery at one week after surgery between the two groups, but the NRS and ODI at the last follow-up in the SOVCF group were significantly higher than those in the MOVCF group. Besides, the vertebral height recovery and local kyphosis improvement in the MOVCF group were superior to those in the SOVCF group after surgery and at the last follow-up. The incidences of bone cement leakage and adjacent vertebral fracture in the SOVCF group were both higher than those in the MOVCF group. Boonen et al. [3] performed a randomized controlled trial to compare PKP with conservative treatment for OVCF, and do a 2-year follow-up, the results of which suggested that PKP could significantly reduce pain and improve life quality without increasing the chance of refracture, which was consistent with our results.
Sagittal alignment balance is essential for quality of life and daily activities. Restoration of sagittal alignment can reduce local stress, decrease the occurrence of re-fracture, and alleviate low back pain due to kyphosis under chronic fatigue, thereby enhancing quality of life and mobility. In this study, the recovery of AVH and LKA after surgery and at the last follow-up in the SOVCF group was significantly poorer than those in MOVCF group, which was consistent with previous studies [16]. Both groups achieved significant pain relief and functional improvement immediately after surgery. However, NRS and ODI in the SOVCF group were significantly higher than those in the MOVCF group at the last follow-up and the recovery of vertebral body height and improvement of kyphotic deformity in the SOVCF group were significantly worse than those in the MOVCF group.
Young et al. [9] used PKP to treat SOVCF, and proved that PKP could significantly alleviate pain and improve function, but the icidence of cement leakage rate, especially disc leakage was high. Wang et al. [5] used PKP to treat 35 SOVCF cases with high compression of more than 2/3 and achieved satisfactory pain relief and functional improvement after an average follow-up of 34 months. Similar results were obtained in this study.
Bone cement leakage is the most common complication after PKP and endplate fracture, intravertebral fissure sign, use of low-viscosity bone cement, and large amount of bone cement are considered as high risk factors for bone cement leakage [17, 18, 19]. SOVCF is complicated with endplate injury in almost all cases due to severe collapse of the vertebra. Furthermore, for SOVCF, vertebral cortical defects and intravertebral fissure signs are also common, so bone cement easily leaks from the defective cortex and injured endplate. In this study, the incidence of bone cement leakage in the disc space was most frequent, which was similar to previous studies [18, 19]. Refractures after vertebral augmentation include operaed vertebral fractures, adjacent vertebral fractures, and distal fractures. Refractures of the operated vertebra are mainly related to inadequate distribution of bone cement, and additonally, the adjacent vertebra is the most common site of the refracture, which is mainly related to the changes of local stress after vertebral augmentation, and osteoporosis. The reasons for the higher incidence of adjacent vertebral fracture (AVF) in the SOVCF group might be as follows:
Poor recovery of local kyphotic angle. The thoracic vertebrae have strong ribcage, and the lumbar vertebrae have physiological lordosis, so severe kyphotic deformity secondary to OVCF in these segments is rare. Thoracolumbar vertebrae are located at the junction of the thoracic vertebrae and lumbar vertebrae, they have a large range of motion, and their physiological curvature is straight, which is the most common site of SOVCF. If the vertebra is severely compressed, large kyphosis is present even after PKP surgery. Kyphotic deformity leads to local stress concentration, which can promote vertebral fracture adjacent to the augmented vertebra. Intervertebral space is the most common site of bone cement leakage, for which the early clinical symptoms are not obvious, but it will accelerate disc degeneration and change the local stress distribution, thereby increasing the risk of adjacent vertebral fractures [20]. Therefore, many researchers recommend prophylactic vertebroplasty of adjacent vertebrae to reduce the risk of AVF in cases of intervertebral space cement leakage [21]. Severe osteoporosis. Several studies have confirmed that the degree of osteoporosis is not only an important factor of the incidence of OVCF, but also is one of the most significant related factors for adjacent vertebral fracture after vertebral augmentation [22]. In this study, the degree of osteoporosis in the SOVCF group was much more severe than that in the MOVCF group (
At the last follow-up of this study, LKA in both SOVCF and MOVCF groups increased, and the degree of loss of correction in the SOVCF group was significantly higher than that in the MOVCF group (6.47
This study is not without limitations. First, this study adopted a retrospective design with a small sample size and a short follow-up time. Second, anti-osteoporosis drugs are very important to improve symptoms and prognosis, many new drugs are targeted at osteoporosis at present [25, 26], and patients in this study were not given the same anti-osteoporosis drugs which might bias the clinical results. Last but not least, the procedures were not performed by the same surgical department, even if all of them are senior surgeons (Xue, Zhang and Dai).
Conclusions
Lower
Author contributions
Youdi Xue and Zhaochuan Zhang conceived and designed the study; Youdi Xue, Jihua Xia, Chao Ma and Weixiang Dai collected the data; Youdi Xue, Jihua Xia, Chao Ma and Weixiang Dai analyzed and interpreted the data; Youdi Xue wrote the manuscript; Zhaochuan Zhang provided critical revisions important for the intellectual content. All authors approved the final version of the manuscript.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Ethical approval
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethic committee of Xuzhou Central Hospital (approval no. XZXY-LK-20200301-041). Written informed consent to publish the clinical details and images was obtained from all participants.
Funding
The study was supported by the Innovation Project of Science and Technology of Xuzhou (KC21206).
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors declare that they have no conflict of interest.