
Abstract
BACKGROUND:
Cervicogenic headache is characterized by chronic posterior neck pain radiating to one side of the head, resulting from cervical spine bone or soft tissue diseases. Cervical ganglioneuroma (GN), a rare benign neuroblastic tumor, especially in the cervical spine, may cause cervicogenic headache-like symptoms.
OBJECTIVE:
We report a case of GN which was surgically removed successfully to relieve the symptom.
CASE REPORT:
A 68-year-old male presented with right posterior neck pain with referred pain to the ipsilateral occipital area in May 2020. Despite administration of medications, physical therapy, and spine interventions, the symptoms intermittently recurred over one year. In July 2021, the patient complained of painful limitation of neck motion, especially on right-sided bending; no motor or sensory deficits, except for subjective numbness of the finger tips, were detected. Plain radiography of the cervical spine showed moderate degenerative changes in the mid-cervical spine. Cervical MRI revealed a cystic mass (1.5 cm
CONCLUSION:
GN of the upper cervical spine should be considered when persistent cervicogenic headache is refractory to conservative management. In such a case, advanced imaging studies such as MRI should be performed for early diagnosis and appropriate treatment.
Introduction
Cervicogenic headache is a type of headache usually associated with chronic neck pain and stiffness, originating from the bony structures or soft tissues of the cervical spine [1]. It is often a sequela of head or neck injury, such as neck strain and cervical fracture or dislocation. However, it may be non-traumatic in origin [2].
Ganglioneuroma (GN) is an uncommon benign neurogenic tumor arising from neuroblastic cells of either the central or peripheral parts of the autonomic nervous system, such as the adrenal glands, paraspinal retroperitoneal ganglia, and mediastinum. It is predominantly found in the posterior mediastinum (60%–80%) or retroperitoneum (10%–15%) and rarely involves the cervical region (5%–8%) [3, 4, 5]. GN is most frequently diagnosed in children under the age of 18 years. The most prevalent clinical manifestation is a painless mass (29.3%), which may become tender as the tumor enlarges. Clinical symptoms vary depending on the size and location of the tumor, with dysphagia (17.2%) and hoarseness (10.3%) being the most commonly reported symptoms [6, 7]. Surgical resection is the treatment of choice [8], and the prognosis is typically positive, provided the adjacent structures are not involved [3].
In this study, we report a case of chronic cervicogenic headache due to a GN affecting the C2 dorsal root ganglion (DRG), which is an unusual site of involvement. Emphasis was placed on the early investigation of uncommon causes of cervicogenic headache with a high level of suspicion when standard management was ineffective.
Written informed consent was obtained from the patient for the publication of this report. The institutional review board of Daejeon St. Mary’s Hospital, The Catholic University of Korea approved this case report (IRB number: DC23ZISI0066).
Case report
In May 2020, a 68-year-old man with underlying hypertension, coronary artery disease, diabetes mellitus, and chronic kidney disease presented to the Neurosurgery Outpatient Clinic with chronic posterior neck pain and referred pain to the right occipital area with dizziness for two weeks. A complete neurological examination, including cranial nerve examination, manual muscle test, sensory test with light-touch and pin-prick test, muscle stretch reflex, long tract signs, and pathologic reflexes, demonstrated no deficits. Brain MRI, performed because of dizziness, yielded no specific findings. Given the mild-to-moderate nature of the pain, the patient was followed up several times with intermittent administration of nonsteroidal anti-inflammatory drugs and synthetic opioids such as tramadol.
In February 2021, the patient slipped on a wet bathroom floor without any preceding neurological symptoms such as dizziness. He developed a small right-sided parietal subgaleal hemorrhage, which was confirmed by a brain CT obtained in the emergency room. The neurosurgeon examined the patient and recommended follow-up visits for monitoring symptom changes. In May 2021, the patient reported increased pain in the right occipital region as well as the posterior part of the neck, especially when rotating the neck or bending it to the right side. The increase in pain was accompanied by right-sided shoulder blade and scapular pain. Physical examination revealed stiffness of the posterior neck muscles, and a neurological examination did not reveal any motor and/or sensory deficits in the extremities. The patient refused to undergo electrodiagnostic studies. Because of the persistent cervicogenic headache, MRI of the cervical spine were recommended. However, the patient refused MRI examination.
In a cervical MRI study, a cystic mass, measuring 2 cm 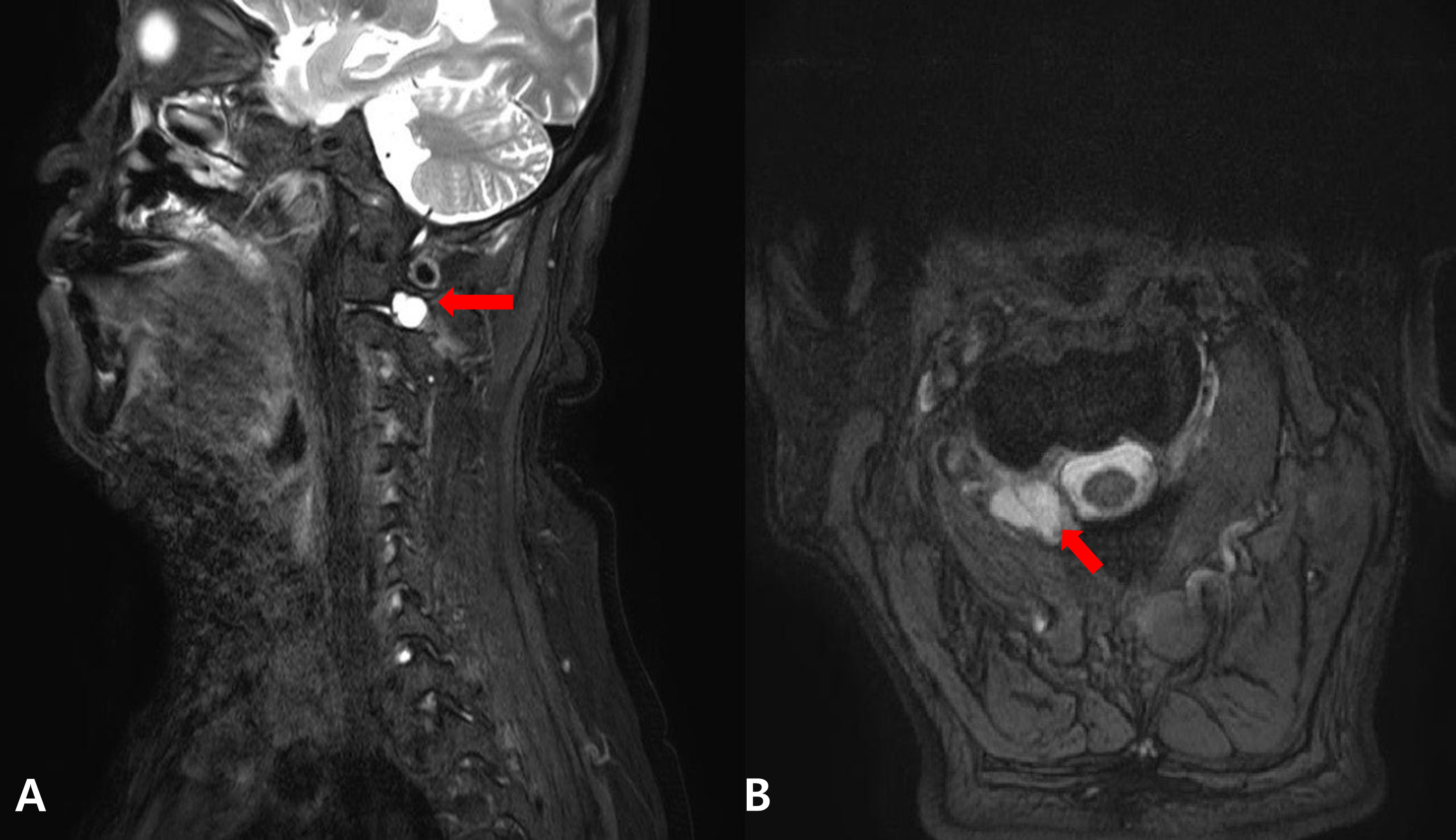
In June 2021, the patient was hospitalized in the Department of Nephrology for the management of elevated serum creatinine levels. During the admission, a non-contrast brain MRI with magnetic resonance angiography (MRA) of the neck was performed because of the persistent headache. The study did not yield any abnormal findings. Two weeks later, a cervical spine MRI was ordered by the Department of Rehabilitation Medicine. The sagittal T2-weighted images and axial T1-gradient echo images of non-enhanced cervical spine MRI (3-mm slices) revealed a cystic mass measuring 2 cm
Before the cystic mass was identified, the patient’s symptoms had not been relieved despite pharmacotherapy with analgesics, nonsteroidal anti-inflammatory drugs, and synthetic opioids as well as physical therapy for several months. Thus, the patient was referred to the Pain Clinic for image-guided spine interventions. A couple of ultrasound-guided blocks to the greater occipital nerve and third occipital nerve at the fascial plane between the inferior oblique capitis and semispinalis capitis muscles provided only temporary pain relief. Once the cystic lesion was identified on the cervical MRI study, its surgical removal was recommended to relieve the symptoms. The patient also expressed a preference for surgical treatment.
During the surgical procedure, the C1 vertebra, vertebral artery, C1–C2 facet joint, and dural sac were identified. After their meticulous identification, the right C2 DRG along with the nerve was completely excised. This procedure was performed with strict adherence to the principle of preserving the surrounding anatomical structures, ensuring minimal impact on it. Intraoperative monitoring was performed using the median, ulnar, and posterior tibial nerve somatosensory evoked potential study as well as motor evoked potential study to those nerves innervated muscles.
Illustrate of the pathology of a C2 dorsal root ganglioneuroma, characterized by an admixture of mature ganglion cells which are identifiable by their large nuclei and abundant eosinophilic cytoplasm, and Schwann cells (Hematoxylin and Eosin). A. x40; Encapsulated ovoid nodule. B. x200; Mature ganglion cells (red arrow) admixed with Schwann cells (blue arrow).
Histopathological examination of the hematoxylin and eosin-stained cyst specimen revealed mature ganglion cells interspersed with Schwann cells, which confirmed the diagnosis of GN. Additional immunohistochemical staining, including S-100 and neuron-specific enolase for Schwann cell and ganglionic components, respectively, was performed to corroborate the diagnosis. No mitotic figures were identified, indicating that the lesion was benign (Fig. 2). At the postoperative one-week follow-up, the patient reported significant symptomatic relief without any complication.
Cervicogenic headache originates from the cervical spine and typically manifests as unilateral pain [1, 2]. The underlying mechanism involves the convergence of the nociceptive afferent neurons from the C1–C3 structures such as spinal nerves and facet joints, and the sensory inputs of the trigeminal nerve at the trigeminocervical nucleus [9], which also leads to afferent nerves from adjacent cervical nerves. Cervicogenic headache is characterized by chronic and recurring pain on neck movements, which is often accompanied by a reduction in the neck range of motion, as seen in our patient [2]. The patient did not report any neuropathic pain. Cervicogenic headache can mimic other types of headaches, such as tension-type headache or migraine. Tension-type headaches are characterized by a dull pressing pain that occurs simultaneously on both sides of the head, resembling the tightening of a band around the head. Migraines are usually described to have a pulsating quality, which is localized to one side of the head and is often accompanied by nausea, vomiting, or sensitivity to light and sound.
GN is a rare benign neurogenic tumor originating from the neuroblastic cells of the autonomic nervous system. GNs typically develop in the posterior mediastinum or retroperitoneum; cervical lesions are rare (1%–8%) [3, 4, 5]. GNs in the cervical region commonly from the larynx, pharynx, or ganglion nodosum of the vagus nerve [10].
Cervical GNs are commonly solitary, painless, and slow-growing masses, occur in approximately 29.3% of cases. Other associated symptoms include dysphagia (17.2%) and hoarseness (10.3%) [6, 7]. If the cervical sympathetic chain is involved, symptoms of Horner’s syndrome may manifest [5]. These symptoms appear due to the compression of the adjacent structures by the tumor. Therefore, identifying the physical characteristics of the tumor, such as size, location, and orientation to anatomical structures, especially nerves, is crucial [11].
The diagnosis of cervical GN involves various imaging studies, such as neck ultrasonography, CT, and MRI [5, 6]. Ultrasonography commonly reveals a solid, hypoechoic, and well-encapsulated mass [12]. CT and MRI play essential roles in determining the size, location, composition, and relationship of the mass with adjacent structures. On CT, the lesions demonstrate low or intermediate attenuation, and approximately 30% of the tumors exhibit calcification. On MRI, the tumors demonstrate low signal intensity on T1-weighted images and markedly high signal intensity on T2-weighted images, as was seen in our patient [13].
Distinguishing GN from other neurogenic tumors, including neurofibroma, Schwannoma, neuroblastoma, ganglioneuroblastoma, and pheochromocytoma, or soft tissue lesions based solely on imaging characteristics can be challenging. The signal intensity characteristics of GNs on MRI are similar to those of these lesions. Therefore, histopathological confirmation is essential [5, 6, 13]. The most prominent histological feature of GN is the presence of mature ganglion cells with compact eosinophilic cytoplasm, distinct cell borders, an eccentric nucleus, and prominent nucleoli; these cells are typically accompanied by satellite cells [14]. These pathological findings were observed in our patient.
Fine needle aspiration (FNA) can be used a diagnostic tool; however, it must be approached with caution. FNA samples may not always yield reliable results, potentially leading to misdiagnosis. Pathological findings, especially when immature components are present in the FNA samples, necessitate further confirmation via surgical biopsy post-FNA [14, 15].
Approximately 37% of mediastinal GNs in the pediatric population are associated with an increase in vanillylmandelic acid or homovanillate levels in the serum and urine. These also reportedly secrete catecholamines, causing redness, hypertension, secretory diarrhea, sweating, flushing, and renal acidosis [4]. Thus, laboratory tests can be considered a part of the diagnostic evaluation.
Surgical resection remains the treatment of choice for GNs; total excision is preferred. Subtotal resection is considered when complete excision poses significant risks to the surrounding structures [6, 7]. Approximately 25% of GNs coexist with malignant lesions. Thus, the tumor’s benign status should be confirmed via frozen section examination using samples obtained from multiple sites when incomplete resection is performed. Symptoms of Horner’s syndrome are often detected postoperatively, and they typically resolve completely within several months [6]. Prognosis of GNs is generally favorable with successful management and low morbidity, which is achieved by complete tumor resection without damage to the surrounding nerves or vascular structures [4]. Recurrence is uncommon after complete resection, and adjuvant treatments such as chemotherapy or radiotherapy are not typically required, even with partial excision [6, 12]. Although no established guidelines exist for the follow-up period, close monitoring is recommended when slight immaturity is observed in the GN.
Conclusion
Our case highlights the importance of understanding the uncommon causes of cervicogenic headache refractory to conservative management and of performing advanced imaging studies such as MRI in time to properly manage treatable cases.
Author contributions
Eunjin Park drafted the initial manuscript, including the introduction, case description, and discussion. Eunseok Choi provided critical revisions to the manuscript, focusing on the analysis and interpretation of the patient’s condition in relation to existing literature. Yeon Soo Lee was responsible for obtaining and interpreting the patient’s radiographic images for inclusion in the report. Jin-Seok Yi performed the successful surgical removal of the tumor. All authors reviewed and approved the final version of the manuscript.
Data availability
The data that support the findings of this study are available from the corresponding author (Eunseok Choi) upon reasonable request.
Ethical approval
The institutional review board of Daejeon St. Mary’s Hospital, The Catholic University of Korea approved this case report (IRB number: DC23ZISI0066).
Funding
The authors report no funding.
Informed consent
Written informed consent was obtained from the patient for the publication of this case report and accompanying images.
Footnotes
Acknowledgments
The authors thank Dr. Jeong-eui Lee, Associate Professor at the Department of Pathology, Konyang University Hospital, and Dr. Jong-ok Kim, Professor at the Department of Pathology of Daejeon St. Mary’s Hospital, The Catholic University of Korea, for reviewing the pathologic findings in Fig. ![]() of this article.
of this article.
Conflict of interest
The authors declare that they have no conflict of interest.