
Abstract
BACKGROUND:
An evaluation of scapula position is important to predict spine curvature and shoulder function in patients with adolescent idiopathic scoliosis (AIS). Therefore, a reliable scapula position is required to assess posture in patients with AIS.
OBJECTIVE:
This study investigated the reliabilities of scapula position tests and differences in scapula position and shoulder function between individuals with and without AIS.
METHODS:
The study compared 18 patients with AIS and 18 healthy controls to identify differences in scapula position and shoulder function. The acromion-table distance, lateral displacement of the scapula, acromion depression, winged scapula, upward rotation of the scapula, and anterior tilt of the scapula were measured. Scapula position test reliabilities were assessed using the intraclass correlation coefficient (ICC), standard error of measurement (SEM), and minimum clinically important difference (MCID). Shoulder function was measured using the Shoulder Pain and Disability Index.
RESULTS:
The reliabilities of scapula position tests (ICC 0.85–0.93, SEM 0.1–1.2, and MCID 0.2–2.5) were good. There were significant differences in scapula position and shoulder function between patients with AIS and healthy controls (
CONCLUSION:
Scapula position tests were highly reliable in patients with AIS; they can be used to evaluate scapula position during clinical assessment of posture in patients with AIS.
Keywords
Introduction
Scoliosis is the most common spine abnormality; it occurs in three planes and is defined as lateral displacement of the vertebrae with rotation
Subjects demographic characteristics
Subjects demographic characteristics
* p < 0.05. Abbreviations: SPADI, shoulder pain and disability index.
Adolescent idiopathic scoliosis is caused by trunk distortion-induced deformation of the spine and rib cage; abnormal postures that can predict trunk distortion in AIS include a pelvic bone slope, shoulder bone asymmetry, lateral spine movement, and scapula asymmetry [5, 6]. Among these, scapula position asymmetry is the best predictor of trunk distortion and overall spine curvature [5]. The scapulae are asymmetric on the convex and concave sides in individuals with AIS; this asymmetry is related to the curvature deformation, and resting scapula position is affected by the degree of the scoliosis curve [7]. Increases in the scoliosis curve cause the scapula to exhibit greater anterior tilt on the convex side [8]. Other studies have revealed elevated protracted [6, 9, 10], anterior tilted [10], and winged [11] scapulae in individuals with AIS. Additionally, individuals with AIS may exhibit changes in the length of periscapular muscles along with the changes in the scapula position at rest, which can lead to shoulder dysfunction arising from abnormal scapula motion [5, 8].
Many clinicians and therapists perform static scapula position tests, such as the acromion-table distance (ATD), scapula lateral displacement (SLD), acromion depression, and winged scapula tests; they also perform dynamic scapula position tests, such as the upward rotated scapula and anterior tilted scapula tests. The ATD is used to measure the forward shoulder (intraclass correlation coefficient [ICC] 0.88–0.94) [12]. The SLD is used to measure the protracted scapula (ICC 0.83–0.97) [13]. A winged scapula is identified (using a scapulometer) as the distance between the thoracic spinous process (SP) and inferior angle (ICC 0.87–0.97) [14]; acromion depression is used to assess scapula height [15]. Acromion depression below the value on the contralateral side indicates scapula depression or scapula downward rotation, which may contribute to shoulder dysfunction [16]. An upward rotated scapula is measured at resting and shoulder-elevation positions (ICC 0.81–0.94) [17, 18]. Scibek et al. reported significant moderate to good associations (
Measurements of scapula position are important for predicting spine curvature in AIS patients, but most researchers have focused on evaluating the pelvic and lumbar spine. In previous studies, the equipment used to measure resting scapula position had the limitations of high cost and requirement for a laboratory setting [5, 6, 7, 8, 9, 10, 11]. Although some methods can easily measure scapula position with high reliability in clinical practice [12, 13, 14, 15, 16, 17, 18, 19], no studies have evaluated their reliabilities in patients with AIS.
This study had two main objectives: to analyze the reliabilities of scapula position tests in patients with AIS and to compare differences in scapula position and shoulder function between individuals with and without AIS.
Subjects
This study enrolled 18 female patients with AIS and 18 age-, height-, and weight-matched participants without scoliosis (Table 1). The inclusion criteria were age 13–18 years and a major thoracic curve with a Cobb’s angle
The statistical package G*Power 3 was used to calculate the sample size for this study. The results of power analysis indicated that at least 16 participants were required to detect a difference in upward rotation at rest, using a two-tailed test with a power of 0.80 and an
CT image (A) when measuring the first scapular position and CT image (B) when measuring the second scapular position.
To evaluate baseline characteristics, all patients completed a questionnaire that included questions regarding demographics. Then, shoulder function was assessed using the Shoulder Pain and Disability Index (SPADI). Before scapula position tests were performed, the examiner used a grease pencil to mark the root of the scapular spine, inferior angle of the scapula, posterior border of the acromion, posterior acromion, seventh cervical SP, and thoracic SP corresponding to the root of the scapular spine. Then, all participants underwent the ATD, SLD, winged scapula, acromion depression, upward rotated scapula, and anterior tilted scapula position tests. They were evaluated twice with 1 week between sessions, at the same time of day, to assess the intraobserver reliabilities of the tests. There was no change in the subjects’ spinal curvature for one week (Fig. 1) and all tests were performed by the same examiner.
Measurement of scapular position
The scapula position measurements included static (ATD, SLD, scapula depression, and winged scapula) and dynamic (upward rotated and anterior tilted scapula) position tests. All tests were performed three times, and mean values were used for data analyses. Each patient was allowed a 1-min rest between tests, and a 10-s rest between consecutive trials.
Palpation meter (A) and the anterior (B) and posterior (C) views of the modified inclinometer.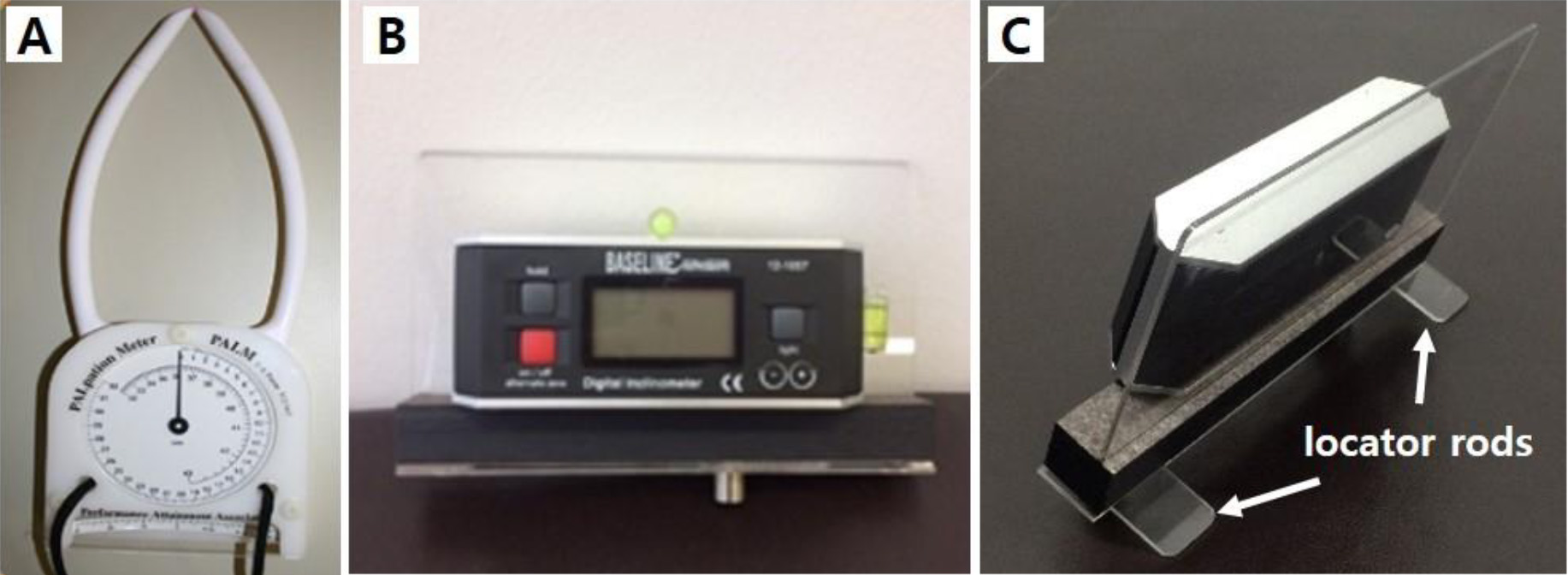
The ATD was measured to identify forward shoulder, rest, and scapula retraction positions, as described by Host [20]. To measure ATD in the rest position, participants were asked to lie relaxed in the supine position on a table, with the examiner standing beside the patient. In this position, the examiner measured the vertical distance between the posterior border of the acromion and the table using a tape. Then, the ATD in the scapula retraction position was measured when the participants actively performed scapula retraction.
Scapula lateral displacement (A) and acromion depression (B).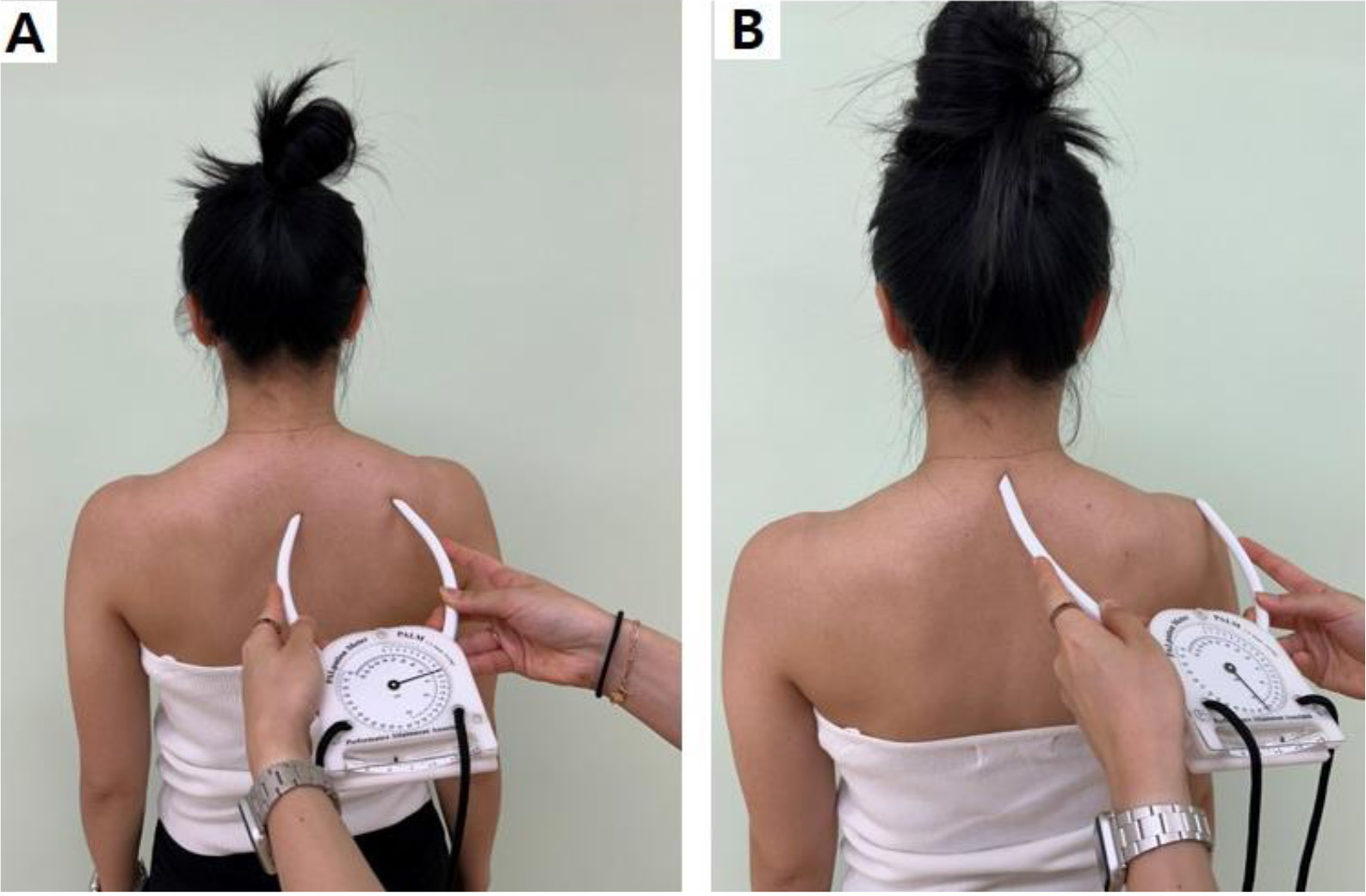
The SLD was measured at rest and in the scapula retraction position using a palpation meter (Fig. 2A), as described by Host [20]. To measure SLD, participants were asked to stand in a relaxed manner, with the examiner standing behind them. The examiner measured the SLD with one arm of the caliper placed on the scapula spine root and the other arm placed on the corresponding thoracic SP. This procedure was repeated with active scapula retraction (Fig. 3A).
Acromion depression was measured by combining the horizontal distance and slope between the acromion and C7 SP, as described by Park and Yoo [15]. To measure acromion depression, participants were asked to stand in a relaxed manner while the examiner stood behind them. The examiner measured the acromion depression with one arm of the caliper placed on the 7th cervical SP and the other arm placed on the acromion (Fig. 3B).
To measure a winged scapula, the examiner utilized the method described by Weon et al. [14]. Participants were asked to stand with their shoulders in the neutral position, elbow joints at 90∘ flexion, and forearms in a neutral position. A cuff weighing 5% of the patient’s body weight was placed on the distal wrist to measure the winged scapula. The examiner stood behind the participants and placed four pads on the posterior thoracic wall with a sliding board at the level of the inferior angle of the scapula. Next, the examiner shifted the sliding board until it met the inferior angle of the scapula, then measured the depth between the thorax and inferior angle of the scapula using a ruler on the fixed board.
Measurement of scapula upward rotation: (A) rest position and shoulder elevation at (B) 60∘, (C) 90∘, and (D) 120∘.
Upward rotated scapula was measured at rest and at 60∘, 90∘, and 120∘ of shoulder elevation in the scapula plane using a modified inclinometer (Fig. 2B and C) [17, 18]. This device has plastic palpation dowels attached to the bottom of the inclinometer for proper placement on scapula bony landmarks. To measure the upward rotated scapula at rest, participants were asked to stand with their arms relaxed at their sides while the examiner stood behind them. The examiner measured the angle between the scapula spine root and posterolateral acromion (Fig. 4A). The upward rotated scapula in shoulder elevation was measured when the participants elevated their shoulders 60∘, 90∘, and 120∘ (Fig. 4B–D). The range of motion (ROM) of shoulder elevation was measured using a digital inclinometer prior to measurement of scapula position.
The anterior tilted scapula was also measured at rest and at 60∘, 90∘, and 120∘ of shoulder elevation in the scapula plane using a modified inclinometer [19]. To measure the anterior tilted scapula at rest, participants were asked to stand with their arms relaxed while the examiner stood behind them. The examiner measured the angle between the scapula spine root and inferior angle of the scapula (Fig. 5A). The anterior tilted scapula in shoulder elevation was measured when the participants elevated their shoulders 60∘, 90∘, and 120∘ (Fig. 5B–D). The ROM of shoulder elevation was measured using a digital inclinometer prior to measurement of scapula position.
Shoulder function was evaluated using the SPADI, a 13-item self-administered questionnaire that is a valid reliable tool for assessing shoulder function; it consists of five items regarding pain and eight items regarding disability [21, 22, 23]. SPADI scores range from 0 to 130, with 130 indicating the greatest pain and disability level.
Statistical analyses
Independent
Differences in outcome variables between convex and dominant sides
Differences in outcome variables between convex and dominant sides
*p < 0.05; Abbreviations: AD, acromion depression; ATD, acromion-table distance; AT, anterior tilt; SLD, scapula lateral displacement; UR, upward rotation.
Measurement of scapula anterior tilt: (A) rest position and shoulder elevation at (B) 60∘, (C) 90∘, and (D) 120∘.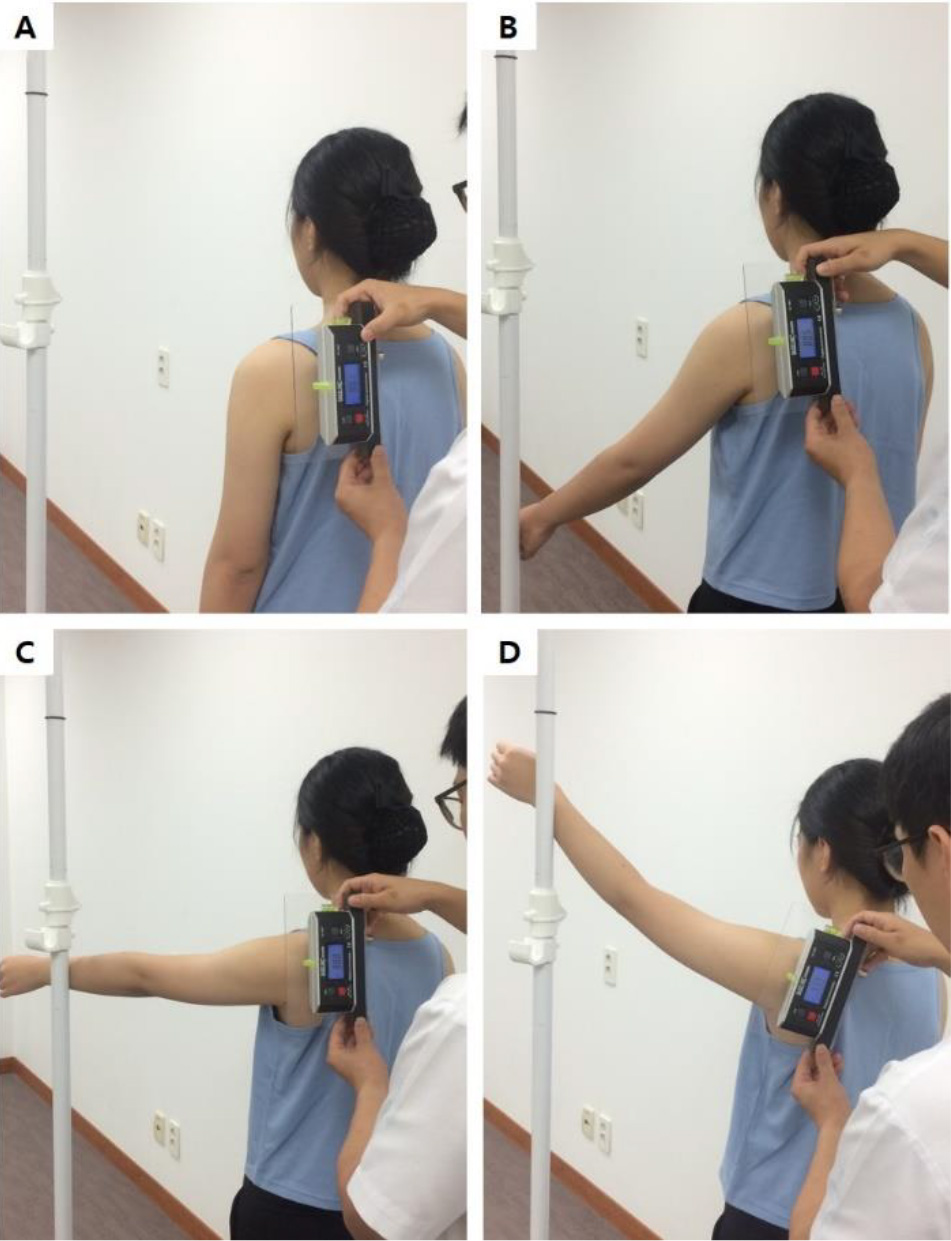
Differences in outcome variables between concave and non-dominant sides
Abbreviations: AD, acromion depression; ATD, acromion-table distance; AT, anterior tilt; SLD, scapula lateral displacement; UR, upward rotation.
Reliabilities of scapula position tests
Abbreviations: AD, acromion depression; ATD, acromion-table distance; AT, anterior tilt; Re, retraction; ICC, intraclass correlation coefficient; MCID, minimum clinically important difference; SEM, standard error of measurement; SLD, scapula lateral displacement; UR, upward rotation.
There was a significant difference between the AIS and control groups in terms of scapula position. The ATD at rest, winged scapula, and anterior tilt (shoulder elevation 60∘, 90∘, and 120∘) were significantly greater on the convex side than on the dominant side; acromion depression and upward rotation (shoulder elevation 0∘, 60∘, 90∘, and 120∘) were significantly lower on the convex side than on the dominant side (all
Table 4 shows the ICC, SEM, and MCID values for scapula position. In the AIS group, the ICCs on the convex side were excellent for ATD, SLD, winged scapula, upward rotation (0∘, 60∘, and 90∘), and anterior tilt (0∘, 60∘, and 90∘); they were high for acromion depression, upward rotation at 120∘, and anterior tilt at 120∘. The SEM and MCID for scapula position on the convex side ranged from 0.1 to 1.2 cm and from 0.3 to 3.3 cm, respectively. The ICCs on the concave side were excellent for ATD at rest, SLD, winged scapula, acromion depression, upward rotation (0∘, 90∘, and 120∘), and anterior tilt (0∘, 60∘, and 120∘); they were high for ATD with retraction, upward rotation at 60∘ and anterior tilt at 90∘ (0.86–0.89). The SEM and MCID for scapula position on the concave side ranged from 0.1 to 1.2 and from 0.1 to 3.3, respectively.
Discussion
This investigation of scapula position tests in patients with AIS revealed reliabilities ranging from high to excellent. Additionally, scapula position and shoulder function differed between the AIS and control groups. Our results showed that the AIS group had higher forward shoulder, winged scapula, and anterior tilted scapula and lower scapula upward rotation.
The ICCs of scapula position tests used in this study ranged from high to excellent. This result can be explained in two ways. First, in this study, the scapula position was measured via palpation of a scapula landmark. In previous studies, scapula position tests based on surface palpation reportedly demonstrated high validity [25]. The reliability may have been good because it is easier to palpate the scapula landmark due to structural changes in the AIS group. Second, the characteristics of the equipment may have contributed to high reliability. To measure upward rotation and anterior tilt, locator rods and cylinders were attached to a modified inclinometer, thereby minimizing errors that can occur during measurement of a rounded scapula. A previous study showed that the reliabilities of measuring upward rotation and anterior tilt using a modified inclinometer were high to excellent in patients with subacromial impingement syndrome [26]. The palpation meter used to measure SLD and acromion depression also has attached arms; thus, the effects of the erector spinae muscles can be minimized during SLD measurement. Furthermore, when measuring acromion depression, the distance and angle between C7 and the acromion can be measured directly, minimizing errors. Previous studies also demonstrated high reliability of SLD measurements via palpation meters [27]. These findings are consistent with our results. However, a high ICC for scapula position does not indicate clinical relevance. Therefore, we measured SEM and MCID, and most of the variables with significant differences were above SEM and MCID. These results suggest that our scapula position tests can be utilized to evaluate AIS.
The scapula positions significantly differed between the AIS and control groups. This is consistent with previous findings of asymmetric scapula positions with slight differences [5, 10]. This change in the AIS group may be explained by the altered spinal structure. Because the scapula is attached to the rib cage, scapula asymmetry is affected by trunk rotation [5]. On the thoracic convex side, the thoracic vertebrae rotate to the ipsilateral side, and lateral bending occurs on the opposite side. During ipsilateral rotation, the ipsilateral rib cage protrudes backward, causing the scapula to float on the rib cage; this leads to winged and anterior tilted scapulae. Additionally, contralateral lateral bending causes the acromion to be oriented in an upward direction. This orientation may shorten the levator scapulae muscles by bringing the superior angle of the scapula close to the transverse process of the cervical vertebrae. Therefore, elevated and downward rotated scapulae more frequently appear on the convex side than on the dominant side. On the concave side, contralateral rotation and ipsilateral lateral bending occur. In this position, the ipsilateral rib cage protrudes forward to create winged and anterior tilted scapulae. Additionally, ipsilateral lateral bending causes the medial scapula border to approach the SP of the thoracic vertebrae and the medial border of the scapula to approach the transverse processes of the cervical vertebrae. Thus, retracted, downward rotated, and winged scapulae more frequently appear on the concave side than on the non-dominant side. The change in scapula position appears to be associated with the altered spinal structure. Future studies should investigate the relationship between the change in scapula position and Cobb’s angle.
The AIS group had a significantly lower functional score compared with the controls, consistent with previous studies [8, 10]. Line et al. reported that patients with AIS had greater shoulder dysfunction compared with a control group; they also found that shoulder dysfunction was negatively correlated with scapula posterior tilt and lower trapezius activity during shoulder flexion [10]. Another study demonstrated that patients with AIS had greater shoulder dysfunction compared with a control group; although the dysfunction was greater, the difference was not clinically significant. Moreover, there were no significant correlations of shoulder function with scapulothoracic kinematics, scapula resting position, or curvature [8]. Although AIS patients have greater shoulder dysfunction compared with controls [8, 10], there has been minimal research concerning this aspect. Additionally, the degree of dysfunction varies among studies, and the causative mechanism is unclear. Therefore, further investigations are needed to confirm functional dysfunction in AIS patients.
Early diagnosis of scoliosis subjects is important for appropriate intervention and prevention of complications [28], and for this, various assessments must be performed. Skeletal maturity is an important factor in spinal curve progression, and subjects with early skeletal maturity need assessment because the severity of scoliosis was greater than subjects with complete skeletal maturity [29, 30]. Assessing spinal posture, such as Adam’s test, axial trunk rotation and plumb line test, which are useful for early diagnosis [28], and assessment of changes in lower extremities alignment (Q-angel, foot, etc.) should also be considered [31]. In addition, it is important to evaluate the scapula position in relation to predictors of the spinal curve among individuals with scoliosis. Our results demonstrated that the scapula position tests used in this study showed good reliability; we found differences in scapula position and shoulder function between the AIS and control groups. Our approach is easy to use in clinical practice; therefore, it can serve as a new paradigm for evaluating posture in patients with AIS, aiding posture evaluation.
There were some limitations in this study. First, the findings cannot be generalized to all patients because the study only included female patients and female controls. Future research should investigate differences in scapula position in male patients with scoliosis. Moreover, we did not measure the interrater reliabilities of the scapula position tests, which should be assessed in future studies of patients with idiopathic scoliosis. Finally, although there are objective descriptive methods to evaluate shoulder function (e.g., muscle strength, ROM, and muscle activity), we only used a self-administered questionnaire to evaluate shoulder function in AIS patients. In future studies, it will be necessary to measure shoulder muscle strength and ROM among patients with AIS.
Conclusions
We investigated the reliabilities of scapula position tests and differences in scapula position and shoulder function between AIS and control groups. The reliabilities of scapula position tests were good. Additionally, the AIS group had greater forward shoulder, winged scapula, downward rotated scapula, and anterior tilted scapula compared with the controls; it had a lower shoulder functional score compared with the controls. The results of this study may provide clinicians with useful information regarding the scapula during assessments of posture in patients with AIS.
Author contributions
Conception: Soo-Yong Kim, Tae-Gyu Kim, Young-Hoon Kim, Rui Ma; Performance of work: Soo-Yong Kim, Tae-Gyu Kim, Young-Hoon Kim, Rui Ma; Interpretation or analysis of data: Soo-Yong Kim, Tae-Gyu Kim; Preparation of the manuscript: Soo-Yong Kim, Tae-Gyu Kim, Young-Hoon Kim; Revision for important intellectual content: Soo-Yong Kim, Tae-Gyu Kim; Supervision: Soo-Yong Kim, Tae-Gyu.
Data availability
Not applicable.
Ethical approval
Ethical approval of our work was obtained from the Ethics Institutional Review Board of Inje University (INJE 2016-10-054-001).
Funding
None to report.
Informed consent
Informed consent was obtained from all participants involved in the study.
Footnotes
Acknowledgments
None to report.
Conflict of interest
None to report.