
Abstract
BACKGROUND:
Chronic stroke can impair cardiopulmonary function, mobility, and daily activities. This study assessed the impact of robot-assisted gait training (RAGT) on such impairments.
OBJECTIVE:
To investigate the effects of robot-assisted gait training on cardiopulmonary function, walking ability, lower extremity function and strength, activities of daily living (ADLs), and blood test results among individuals with chronic stroke.
METHODS:
A multicenter, prospective, single-blinded, randomized controlled trial with 22 chronic stroke participants compared RAGT against a control exercise regimen. RAGT involved three days weekly sessions of high-intensity interval training for 8 weeks (24 sessions) with a Morning Walk® device. The control group also performed home exercises. (24 sessions) Measures included VO2max, Functional Ambulatory Category, 2-minute walk test, 10-meter walk test, Motricity Index-Lower, Korean version of the Fugl-Meyer Assessment Scale, Modified Barthel Index, Berg Balance Scale, muscle strength, InBody body composition, and blood tests (cholesterol, lipid, glucose).
RESULTS:
RAGT significantly improved VO2max, gait, balance, and lower limb strength compared with controls, with significant improvements in 2-minute walk test, 10-meter walk test, Motricity Index-Lower, and Fugl-Meyer Assessment outcomes. No changes were seen in muscle mass or blood markers.
CONCLUSION:
RAGT enhances cardiopulmonary function and ambulatory capacity in chronic stroke patients, underscoring its potential in stroke rehabilitation.
Introduction
Motor function recovery post-stroke progresses swiftly within the initial week, with the recovery curve plateauing typically between 3 and 6 months after the stroke event [1]. Longitudinal studies focusing on patients at 2-year post-stroke follow-up are scarce [2].
Patients with chronic stroke face challenges, such as gait disability, diminished capacity for daily activities, limited potential for returning to work or school, increased socioeconomic costs, and a decline in quality of life [3]. Maximal oxygen uptake (VO2max), walking speed, and endurance capacity have been shown to be halved in stroke survivors compared with healthy counterparts. Impaired cardiovascular or pulmonary function on the affected side manifests as cardiac insufficiency and impaired ventilation and perfusion [4]. Physical inactivity further constrains the ability to perform aerobic exercises, thus limiting activities of daily living (ADLs) [5]. Recent research has shown that aerobic training can improve cardiorespiratory function in individuals with stroke sequelae. Additionally, aerobic training has the potential to increase physical activity levels among stroke patients [6]. A study conducted with gradient treadmill walking found that aerobic exercise improved cardiorespiratory function, reduced blood pressure, decreased heart rate (HR), increased walking speed, improved lower muscle strength, and improved quality of life in stroke patients [5]. Thus, improvement in cardiopulmonary function is a critical therapeutic goal for stroke survivors, as it can lead to improvements in walking ability and other important outcomes [7].
Robot-assisted gait training (RAGT) has the benefits of providing repetitive, intensive, and task-oriented training, which are the representative principles of gait rehabilitation [8]. Research has shown that Lokomat-assisted aerobic training outperforms traditional physical therapy in improving cardiopulmonary function and lower extremity muscular strength in acute stroke patients [9]. Another study found that high-intensity RAGT at 70% of HR reserve is an effective aerobic training method for chronic stroke survivors [6]. High-intensity interval training (HIIT) has been shown to provide similar or even superior outcomes to moderate-intensity continuous exercise training but with the advantage of improved time efficiency [10]. RAGT has been employed to enhance cardiopulmonary capacity, especially to improve walking function in individuals with incomplete spinal cord injury. However, there has been a lack of research exploring the impact of RAGT incorporating high-intensity interval exercises on cardiopulmonary function and walking ability in individuals with chronic stroke [11].
This study investigated the effects of RAGT on cardiopulmonary function, walking ability, lower extremity strength, ADLs, and blood test outcomes at least 2 years post-stroke.
Materials and methods
Study design and patients
A multicenter, prospective, single-blind, randomized controlled trial was conducted in the Republic of Korea from February 2020 through March 2022. The physical therapist responsible for pre- and post-assessments was blinded to participant group assignments.
Ethics
This study was approved by the relevant institutional review board (IRB 2020-0146) and was registered with the Clinical Research Information Service (cris.nih.go.kr), number KCT0004810.
Inclusion and exclusion criteria
Chronic stroke patients were screened for eligibility by physicians at our center. The inclusion criteria were as follows: (1) unilateral motor weakness after ischemic stroke or vascular cerebral hemorrhage over 2 years prior, (2) Functional Ambulation Category (FAC)]
Sample size
The sample size was derived from the within-group standard deviations of maximum oxygen uptake values in a prior study [12] With a standard deviation of 1.5 in the experimental group and 1.0 in the control group, ten participants per group would yield an 80% power to detect a 20% difference in improvement between groups at a significance level of 5% (
Rehabilitation program
The “MORNING WALK” rehabilitation device in use.
Exercise intensity control protocols for rehabilitation.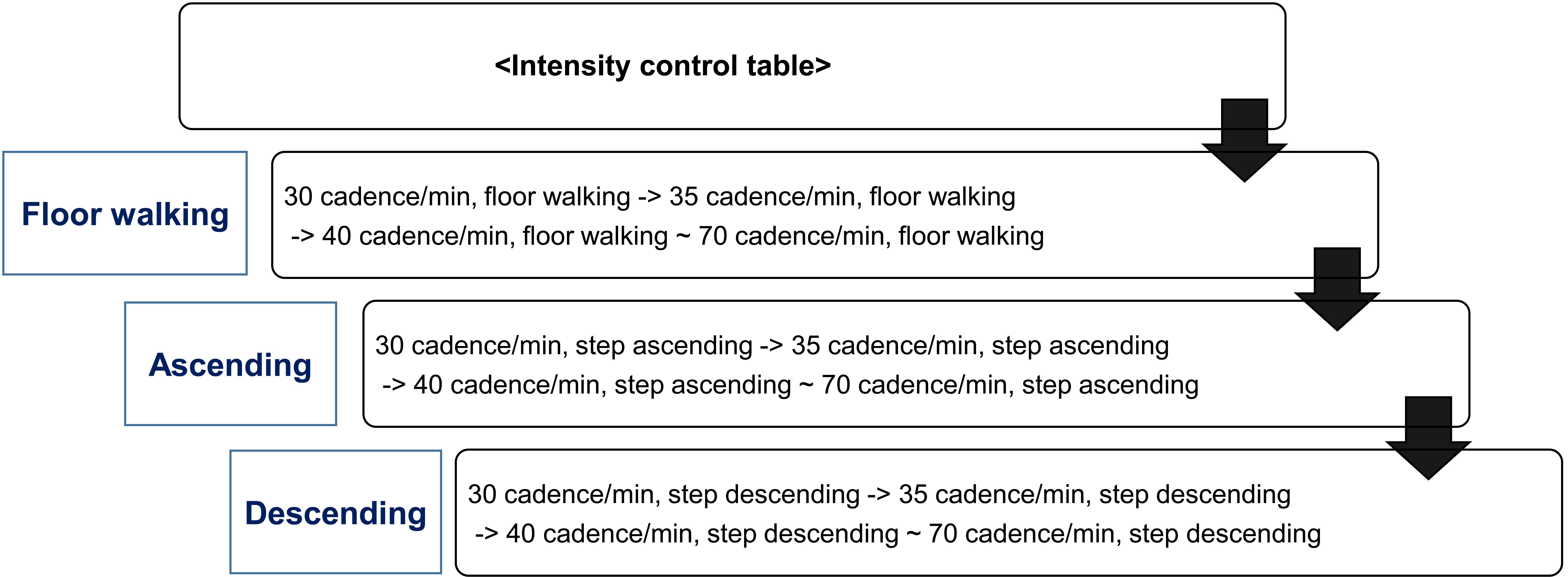
The RAGT group underwent 20-minute sessions of robot-assisted walking using the Morning Walk® thrice weekly for eight weeks, totaling 24 sessions. Each session included 5-minute stretching exercises for warm-up and cool-down. The Morning Walk®, an end-effector-type lower limb rehabilitation robot developed in Korea, facilitates gait via foot plates that produce walking trajectories while allowing free hip and knee movement. It features visual feedback for weight-bearing and a virtual reality screen depicting scenes like walking in a park or forest (Fig. 1). Training intensity was tailored at the outset to each patient’s characteristics (age, height, weight, stroke onset date) and ambulation level (FAC), with speeds incrementing up to 30–70 steps per minute. Intensity adjustments involved shifting modes from ascending to descending stairs and incrementing intensity according to the control table (Fig. 2). Training parameters were guided by a previous study [13].
Subjective intensity monitoring was performed using the Borg scale, a 20-point scale that is commonly used for stroke patients [14]. We used pulse oximeters to monitor HR and oxygen saturation during exercise. The intensity of the exercise was adjusted according to the rating of perceived exertion (RPE), as measured using the Borg scale.
The HIIT strategy involved 3-minute bursts of exercise at an RPE
The control group received one set of home exercise education. The home program included aerobic, balance, stretching, and strengthening exercises. Participants also engaged in outpatient physical therapy twice weekly. The patients’ adherence to the exercise regimens was assessed using an exercise diary, which was reviewed at the final evaluation.
We evaluated primary outcomes, including VO2max, at baseline and after 8 weeks. Secondary outcomes assessed by a ability to perform physiotherapist included the FAC, 2-minute walk test (2MWT), 10-meter walk test (10MWT), Berg Balance Scale (BBS), Motricity Index-Lower (MI-L), Korean version of the Fugl-Meyer Assessment Scale (K-FMA), Modified Barthel Index (MBI), muscle strength tests (knee extensor and knee flexor), body composition, and blood tests (cholesterol, lipid, and glucose). Detailed observations were made using various measurement indicators. We also monitored for adverse events (any undesirable or harmful outcomes).
VO2 max analysis
VO2max at maximum exertion was measured using cardiopulmonary motion measurement equipment and a stationary bicycle, applying the Modified Bruce protocol to capture values indicative of anaerobic threshold levels [16].
Functional ambulatory category (FAC)
The FAC score, which assesses patients’ ambulatory function, categorizes walking ability into six levels based on the degree of physical support needed, ranging from 0 (cannot walk) to 5 (can walk independently anywhere) [17].
2MWT (2-minute walk test)
The distance traveled during 2 minutes of walking was measured to determine functional walking ability. This is particularly useful for minimizing patient fatigue and is more reliable than the 6-minute walk and 12-minute walk tests [18].
10-meter walk test (10MWT)
Walking speed was measured while patients walked for 10 m. The 10MWT test is highly reliable for evaluating the walking speed of stroke patients [19].
Berg balance scale (BBS)
The BBS is a useful measure of balance impairment for use in post-stroke assessment. On a scale from 0–56 points, the higher the score, the higher the balance ability [20].
Motricity index-lower (MI-L)
The MI-L tool was used to evaluate lower limb function. On a scale from 0–100 points, higher scores reflect better lower limb function. Severe paralysis is defined by scores of 0–32, moderate by 33–64, and mild by 65–99 [21].
Korean version of the Fugl-Meyer assessment scale (K-FMA)
Functional recovery of the lower limbs was evaluated using the K-FMA [22].
Modified barthel index (MBI)
ADLs were evaluated using the MBI (scored from 0–100). Higher scores indicate higher independence levels in daily life [23].
Muscle strength testing (knee extensors, knee flexors)
Knee extensor and flexor muscle strength were measured using an isokinetic leg dynamometer (InBody Co. Ltd., Seoul, Korea). Patients exerted maximum force for a duration of 3–5 seconds, and the isometric force was recorded. This procedure was repeated three times to ensure reliability, and the highest measurement was documented [24]. Assessing the strength of the knee extensors alone is considered to be indicative of overall lower limb strength in individuals with chronic stroke sequelae [25, 26].
Baseline demographic characteristics by group
Baseline demographic characteristics by group
BMI: body mass index; MMSE: Mini-Mental State Examination; FAC: functional ambulatory category; RAGT: robot-assisted gait training.
Body composition analysis was based on bioelectrical impedance with the patient in a supine position [27]. The InBody S10 was used to evaluate muscle mass and fat content [28].
Blood testing
We analyzed blood levels of cholesterol, lipids, and glucose. Blood collection was performed by a clinical pathologist in the hospital’s pathology department.
Statistical analysis
Statistical analyses were performed using PASW Statistics for Windows, version 18.0 (SPSS Inc., Chicago, IL, USA). Distributional normality was assessed using the Kolmogorov-Smirnov and Shapiro-Wilk tests. Continuous and categorical variables are expressed as mean
Results
Initially, 25 participants were screened for inclusion in the study. However, one individual did not fulfill the inclusion criteria, leading to the randomization of the remaining 24 participants into two groups of 12. Subsequently, one participant from each group opted not to participate, resulting in 11 patients in the RAGT group and 11 in the control group (Fig. 3) Throughout the study, no adverse events, such as pain, were reported. Among the participants, the 11 who completed RAGT demonstrated good adherence to the program. The mean post-stroke intervals were 88.0 months for the RAGT group and 81.5 months for the control group. When comparing baseline characteristics, including Mini-Mental State Examination scores, underlying causes of stroke, and FAC scores, no significant intergroup differences were found (Table 1).
Primary outcome
In the primary outcome assessment, the RAGT group demonstrated a significant improvement in VO2max (2.2
Comparison of mean values obtained from baseline to after 8 weeks in both groups
Comparison of mean values obtained from baseline to after 8 weeks in both groups
VO2max: maximal oxygen consumption; 2MWT: 2-minute walk test; 10MWT: 10-meter walk test; BBS: Berg Balance Scale; MI-L: Motricity Index-Lower; K-FMA: Korean version of the Fugl-Meyer Assessment Scale; FAC: Functional Ambulatory Category; MBI: Modified Barthel Index; RAGT: robot-assisted gait training. *Significant difference between pre-intervention and post-intervention outcomes within group (
Flowchart of participant enrollment.
Comparison of meaningful results between the Morning Walk group and control group
VO2max: maximal oxygen consumption; MI-L: Motricity Index-Lower; K-FMA: Korean version of the Fugl-Meyer Assessment Scale; 2MWT: 2-minute walk test; 10MWT: 10-meter walk test; FAC: Functional Ambulatory Category; BBS: Berg Balance Scale; MBI: Modified Barthel Index. *Significant difference between pre-intervention and post-intervention outcomes within group (
After the completion of 8 weeks of training, the RAGT group exhibited significantly improved outcomes in terms of the 2MWT, 10MWT, MI-L, K-FMA, BBS, and non-paretic and paretic knee extensor/flexor strength. The control group exhibited improved BBS scores. There were no significant intergroup differences in muscle mass or fat indices. There were also no intergroup differences in blood values in cholesterol and glucose levels in both groups, and lipid indices showed a significant increase in the control group. (Table 2). In the RAGT group, MI-L (5.0
Discussion
A Cochrane review analyzing 62 studies with 2440 patients provides high-level evidence supporting the efficacy of RAGT in improving independent gait in acute stroke patients [29]. Furthermore, a 2020 literature review analyzed 10 studies with a total of 591 participants and reported that end-effector RAGT is effective in improving walking ability among stroke patients [30]. However, chronic stroke patients were included in only three studies in our literature review.
In our study, the RAGT group exhibited a statistically significant increase in maximal oxygen intake per body weight from 12.08 mL/kg/min pre-exercise to 15.0 mL/kg/min post-exercise. Conversely, the control group showed a minimal increase from 16.3 mL/kg/min to 16.6 mL/kg/min In our findings, the Vo2max showed non-significant increase in the within-group comparison, however, in the between- group comparison (Table 3), the VO2max is markedly increased in RAGT group in comparison to control one [6] Our results support the use of RAGT for improving cardiovascular fitness in chronic stroke survivors and align with Gjellesvik et al., who found significant VO2max improvements post-treadmill training intervention [31] Bae et al. showed that high-intensity RAGT significantly improved VO2max and dynamic balance, maximally at an RPE rating of 15 [12] A recent systematic review revealed a significant difference in peak VO2 for participants engaging in HIIT relative to those undergoing continuous aerobic training. HIIT has been found to be more effective in enhancing cardiorespiratory fitness, balance, and gait speed in post-stroke patients. The control group in this study likely showed no such improvements due to the absence of HIIT [32].
Improvements in the K-FMA scores were significantly higher in the intervention group compared with those of the control group. This aligns with findings from Walkbot studies, which have indicated FMA score improvements in patients with subacute hemiparetic stroke. Despite some variations, studies have consistently reported that walking speed, single-limb stance time, and lower extremity motor scores on the FMA improve with robot-assisted therapies [9, 33].
Upon completing 8 weeks of RAGT, participants showed improvements in walking speed during the 10MWT. Bruni et al. [29] found that patients with subacute stroke gained more in terms of walking velocity when treated with end-effector devices, as opposed to those using exoskeletal robots The RAGT group also exhibited improvements in the 2MWT. These advancements are supported by recent research showing significant post-training improvements in 2MWT results for chronic stroke survivors. In our study, gait speed, stride length, and cadence also improved, suggesting that modifications in gait parameters through robot-assisted training contributed to these improvements [34].
Compared with robot-assisted training alone or conventional therapy, the combination of robot-assisted training with virtual reality is hypothesized to be the superior intervention for enhancing balance, and virtual reality may significantly aid in improving daily functions for post-stroke patients [35]. Functional recovery, as evidenced by increased MBI scores, typically manifests in acute stroke patients following robot walking training [36]. Additionally, a pilot study explored the effects of end-effector lower limb rehabilitation robot training on FAC, MI, FMA for lower extremities, 10MWT, BBS, and MBI outcomes in subacute stroke patients [37]. Another study found that MI and MBI outcomes improved in association with RAGT [38]. Considering the mean post-stroke duration of 19 months among the participants of that study, significant changes in ADLs were less likely due to the chronic nature of their conditions. Similar to our study, improvements were noted only in the MI post-intervention. Additionally, in our study, no changes were observed in FAC and muscle strength, which was likely attributable to the chronic post-stroke status of the participants.
Regarding balance, the RAGT group showed a mean improvement of 2.9 points on the BBS after 8 weeks. This aligns with previous studies wherein robotic locomotor retraining resulted in greater improvements in balance [39] RAGT may modify muscle activity in the lower extremities, consequently enhancing functional performance. It is also hypothesized that RAGT can increase the motoneuronal firing rate, potentially improving balance in stroke survivors [40].
The control group’s exercise regimen failed to cause significant changes in cardiorespiratory and gait functions or muscle strength, with the exception of improvements noted in the BBS [41]. It is crucial to identify and target the key elements of physical activity – such as intensity, frequency, and duration – to enhance intervention outcomes. Notably, lipid levels in the control group increased post-intervention, a factor recognized for its significant role in stroke risk [42].
Contrary to expectations based on existing literature suggesting that physical activity can boost cardiorespiratory fitness and decrease blood pressure, lipids, and body weight [43] our study did not observe improvements in glucose, cholesterol, or lipid levels post-intervention. Similarly, another study found no change in body mass index and blood values following home-based HIIT in patients with lacunar stroke [44].
Participants in this study were chronic stroke survivors, averaging over 80 months post-stroke onset. The progress observed through RAGT may reflect a recuperation from their compromised physical function.
To refine RAGT for chronic stroke, it is imperative to develop evidence-based, standardized rehabilitation protocols tailored to each patient’s clinical condition. A HIIT protocol within RAGT may prove beneficial for enhancing cardiopulmonary function, muscle strength, and lower extremity function in these patients.
This study had several limitations. First, exercise intensity was subjectively gauged using the Borg scale. While high-intensity RAGT targeting 70% of HR reserve was associated with better cardiopulmonary outcomes than a control group adjusted to a Borg scale rating of 15 [12]the Borg scale’s strong correlation with HR (
Conclusions
To the best of our knowledge, this multicenter, single-blind randomized controlled trial was the first clinical study to illustrate, in individuals with chronic stroke, the effects (on cardiopulmonary function and on the function and strength of lower extremities) of end-effector RAGT that incorporates HIIT. The observed improvements in cardiopulmonary function in the RAGT group were attributable to increased HR, blood volume, and oxygen consumption. Similarly, the improvements in lower extremity function and muscle strength likely stem from intensified muscle activity and enhanced muscular strength.
Given that RAGT, which includes high-intensity interval exercises, has been proven to be a safe and effective modality to improve functional outcomes, it warrants consideration as a novel therapeutic approach for chronic stroke patients seeking to enhance their cardiopulmonary function, lower extremity function, and muscle strength.
Author contributions
All authors drafted the protocol. JH Do, DY Kim, MH Ko and EJ Ko made substantial contributions to the conception and design of the research; WT Lim and DY Kim revised the paper carefully; GW Kim and JH Kim selected materials and extracted data. JH Do wrote this manuscript; SB Kim and H Kim selected which protocol to include. All authors read and approved the final manuscript.
Data availability
The data used in this study are not publicly available due to the data protection policy of the authors’ institution. Researchers who wish to access the data can request it by contacting the corresponding author.
Ethical approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Asan Medical Center (IRB 2020-0146).
Funding
This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI15C1529); the Market Creation Robot Supply Project 2020 through the Ministry of Trade, Industry and Energy of the Republic of Korea and Korea Institute For Robot Industry Advancement (Business support program for rehabilitation robots 2020); and the Translational Research Center for Rehabilitation Robots (#NRCTR-EX22003), National Rehabilitation Center, Ministry of Health and Welfare, Korea.
Informed consent
All participants in this study were fully informed about the purpose of the research, the procedures, and the potential risks involved, and signed a consent form.
Footnotes
Acknowledgments
This research was supported by the Bio&Medical Technology Development Program of the National Research Foundation (NRF) funded by the Korean government (MSIT) (No. RS-2023-00236157); and the Translational Research Center for Rehabilitation Robots (#NRCTR-EX22003), National Rehabilitation Center, Ministry of Health and Welfare, Korea.
Conflict of interest
The authors declare that they have no conflicts of interest.