
Abstract
Background
Cognitive functional therapy (CFT) aims to address low back pain (LBP) comprehensively by considering physical, psychological, and social factors.
Objective
The objective was to evaluate the effectiveness of CFT in reducing pain and disability in individuals with LBP over various time intervals.
Method
A comprehensive literature search was conducted to identify relevant randomized controlled trials (RCTs) assessing the effects of CFT on LBP.
Results
In this study, 1510 records were initially identified, and 7 studies were included in the analysis. Disability scores were significantly reduced after CFT had been applied for 6 to 8 weeks (SMD
Conclusion
CFT showed potential for improving disability scores for individuals with LBP across various time intervals. However, its impacts on pain scores varied.
Keywords
Introduction
Millions of individuals in the world suffer from low back pain (LBP), a musculoskeletal condition [1, 2]. This condition not only puts immense strain on healthcare infrastructures but also is a principal cause of disability. Those afflicted by LBP frequently face both physical and psychological challenges, which can drastically diminish their overall well-being [3, 4]. Historically, treatment approaches for LBP predominantly focused on physical remedies. However, recent studies have highlighted the importance of acknowledging the cognitive and emotional facets of pain. In response to this, cognitive functional therapy (CFT) has emerged as a promising approach; the aim is to integrate the management of physical symptoms with the preservation of psychological well-being, thereby facilitating a comprehensive path to recovery [5, 6]. This multidisciplinary approach underscores the need for treating LBP with well-developed methods, acknowledging the complex interplay between the mind and body in the healing process [7, 8, 9].
Traditional therapies have generally addressed anatomical and structural issues, and their efficacy has been determined by monitoring pain levels and their relief [10]. CFT has adopted a complementary strategy by acknowledging the interplay of the physical, psychological, and social elements that contribute to a person’s perception of pain and impairment. CFT seeks to empower patients by addressing these many components, assisting patients in regaining control over their lives and enhancing their capacity to function [11, 12].
CFT focuses on the role of cognitive factors in managing LBP. These factors include negative beliefs, catastrophic thoughts, and distorted perceptions that can worsen pain and hinder recovery. By addressing these cognitive aspects, CFT helps patients develop more adaptive ways of thinking about their condition, reducing the impact of pain on their daily lives [13, 14, 15]. CFT also emphasizes improving functional abilities and physical performance through targeted exercises and movement-based interventions, allowing patients to lead more active and fulfilling lives [16, 17]. The effectiveness of CFT is significantly influenced by its patient-centered methodology [18].
CFT tailors therapies to meet patients’ unique requirements, preferences, and objectives rather than using a one-size-fits-all strategy. This method promotes patient self-management, which improves treatment results and long-term adherence to self-management techniques [8]. Additionally, CFT acknowledges the need to manage the mental discomfort often linked to persistent LBP. CFT gives patients coping mechanisms with which they can handle anxiety and depression and also offers psychological therapies such as cognitive-behavioral approaches and relaxation training that can enhance a patient’s overall well-being. According to practitioners of CFT, the patient’s social milieu, alongside the patient’s individual traits, influences his or her perceptions of pain and disability. Elements such as familial dynamics, occupational pressures, and societal views on pain can also affect a person’s recovery process. CFT integrates strategies to manage these social factors, with the aim of fostering an environment that is conducive to enhancing rehabilitation outcomes [12, 14].
The evidence for CFT’s efficacy in treating LBP is encouraging and continues to develop. Clinical studies and thorough analyses have shown that patients who received CFT therapies had considerable pain relief, gains in their functional capacity, and a reduction in their level of impairment [19, 20, 21]. It is crucial to remember that CFT does not aim to replace conventional medical therapies. Instead, there may be room for combining CFT with already-used methods to provide patients with LBP with a more thorough and all-encompassing therapy regimen. Our meta-analysis rigorously examined and synthesized the relevant evidence to better understand how CFT can be used as a therapeutic option for people with LBP.
Materials and methods
This meta-analysis followed the guidelines outlined in the Cochrane Handbook for Systematic Reviews of Interventions [22] and adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standards [23]. The study was registered at the PROSPERO International Prospective Register of Systematic Reviews (accession number CRD42024522668).
Study selection
A comprehensive literature search was conducted to identify relevant studies for inclusion in the meta-analysis. PubMed, Scopus, Cochrane Library, Embase, and Web of Science were searched using appropriate keywords related to “cognitive functional therapy” and “low back pain”. We included all eligible trials from inception to July 2023.
Inclusion and exclusion criteria
To ensure the validity and reliability of our findings, we applied specific inclusion and exclusion criteria to select relevant studies for this meta-analysis. Only RCTs were included so that the evidence would be of high quality. Studies must have assessed the effects of CFT (compared with an active or passive control method) on LBP. The CFT interventions included cognitive and behavioral strategies combined with movement-based interventions. It was essential for the studies to have a clearly defined control group, which could take part in traditional therapeutic exercises, group-based exercises and education, core exercises and manual therapy, or usual care (Table 1). Additionally, studies were required to report outcomes related to pain intensity and/or degree of disability using standardized measures such as the Visual Analogue Scale (VAS), Numeric Rating Scale (NRS), Numeric Pain Scale (NPS), Oswestry Disability Index (ODI), or Roland-Morris Disability Questionnaire (RMDQ). We included only studies published in English, without restrictions on publication date, and focused on participants with chronic low back pain (CLBP) or non-specific chronic low back pain (NSCLBP), while also considering studies on LBP caused by specific conditions such as scoliosis if they met the other criteria.
Baseline and summary of the included studies.
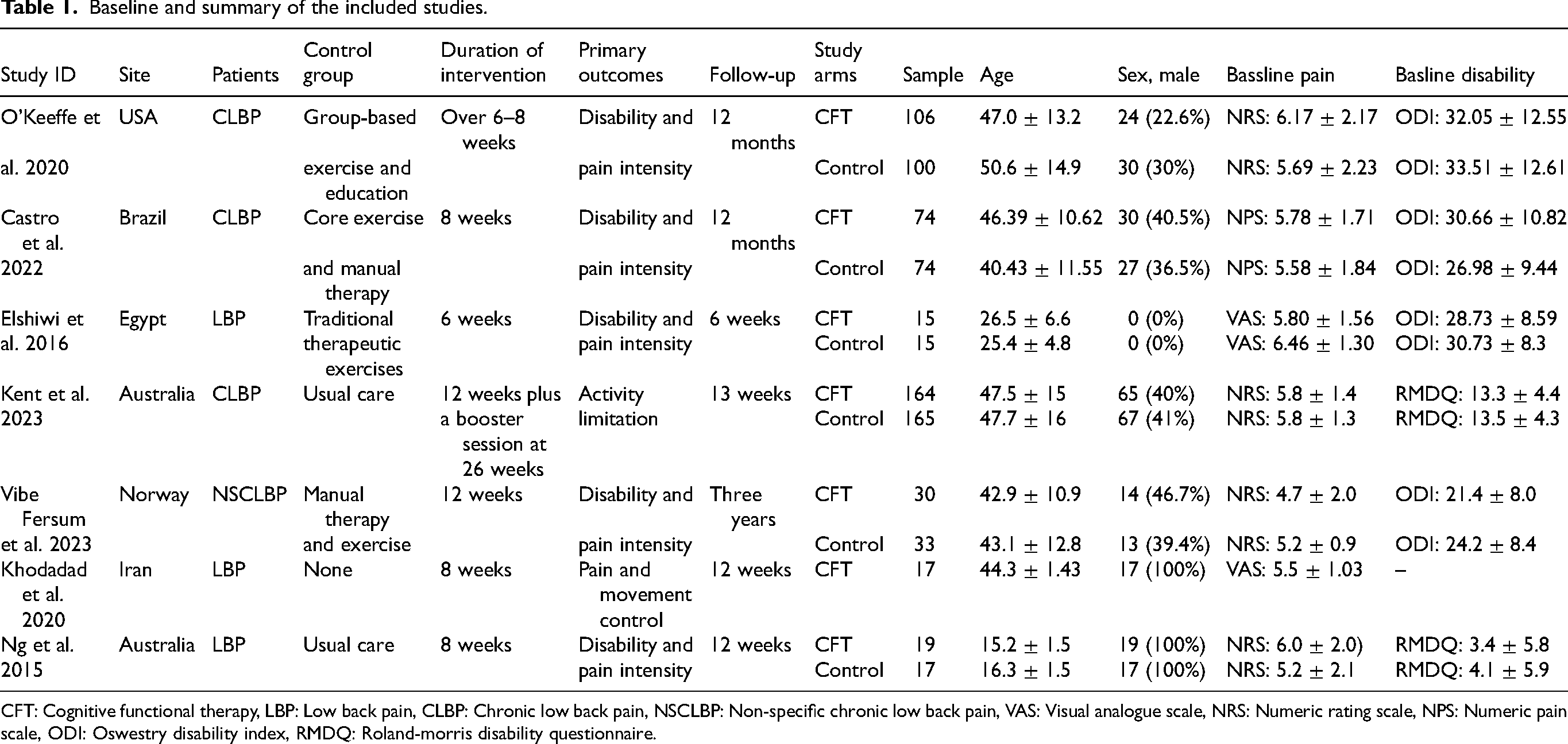
Baseline and summary of the included studies.
CFT: Cognitive functional therapy, LBP: Low back pain, CLBP: Chronic low back pain, NSCLBP: Non-specific chronic low back pain, VAS: Visual analogue scale, NRS: Numeric rating scale, NPS: Numeric pain scale, ODI: Oswestry disability index, RMDQ: Roland-morris disability questionnaire.
Exclusion criteria were applied to maintain the robustness of our analysis. Studies that were not RCTs, such as observational studies, case reports, or reviews, were excluded. We also excluded studies that did not provide sufficient data from which estimates of effects could be derived, and animal studies were excluded as well because we wanted to focus on human clinical trials.
Data from each qualifying study were gathered by two separate reviewers, who focused on details such as the characteristics of the study (e.g., the authors and the year of publication), the traits of the participants (e.g., the number of participants and their ages), and the results (e.g., the average level of pain intensity and level of disability). Differences in opinion between the reviewers were settled by conversations lasting until an agreement was reached.
Quality assessment
The quality of the included studies was evaluated with suitable tools, including the Cochrane Collaboration’s Risk of Bias Tool version 2 for RCTs. The evaluation focused on aspects such as the process of randomization, deviations from planned interventions, unreported outcome data, how outcomes were measured, and the choice of outcomes that were reported.
Statistical analysis
To perform the analysis, we employed RevMan 5.4. The effect size was assessed using the mean difference (MD) and standardized mean difference (SMD) with 95% confidence intervals (CIs) for continuous outcomes (e.g., pain intensity and degree of impairment). A random-effects model was used to aggregate the effect estimates from many studies while considering the potential for study heterogeneity. To illustrate the effect sizes and their 95% CIs for each outcome measure graphically, forest plots were created. The
Results
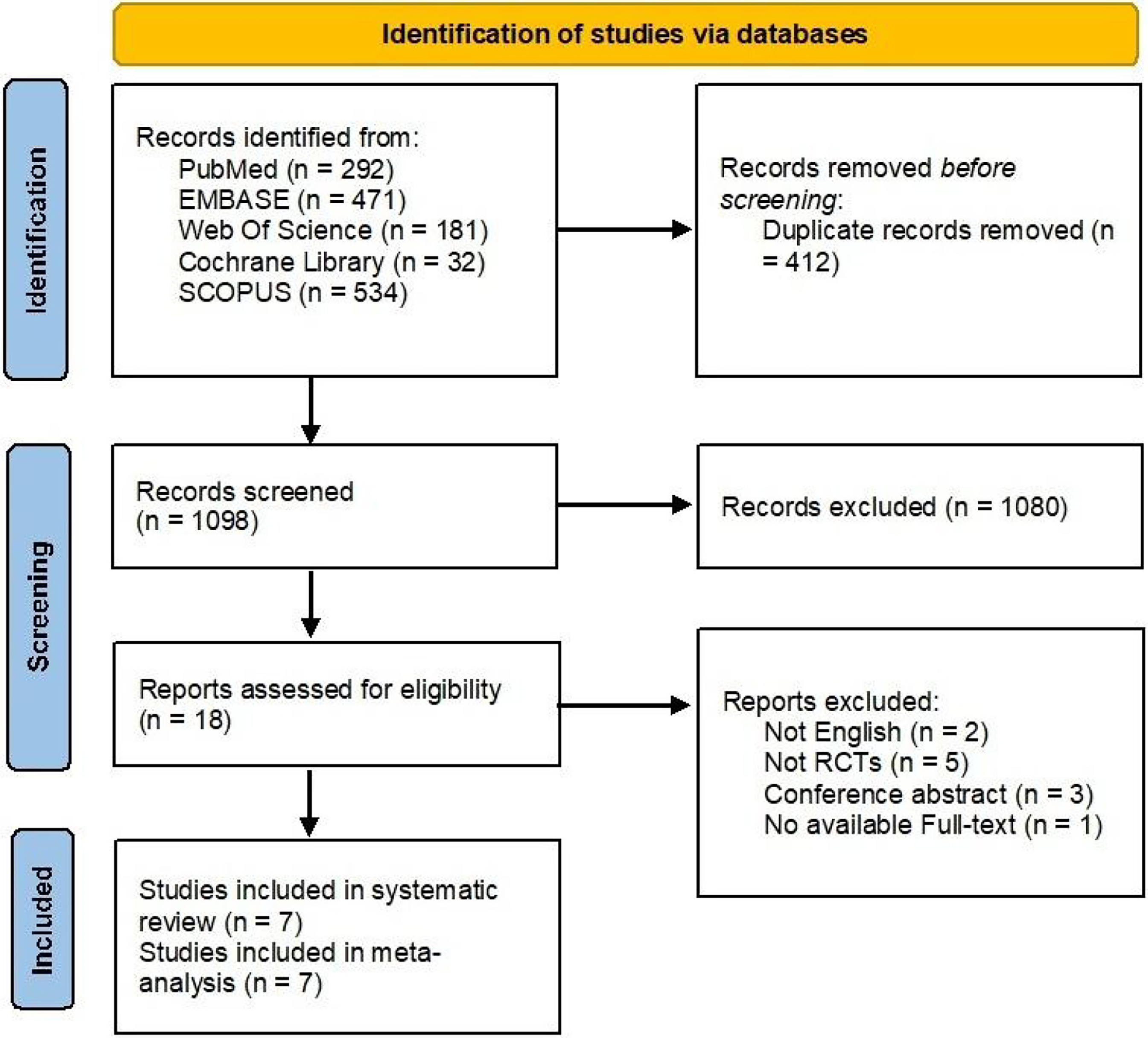
PRISMA flow diagram.
In this study, 1510 records were initially identified through a comprehensive literature search. After removing duplicate records (
The included RCTs were conducted in various countries, including USA, Brazil, Egypt, Australia, Iran and Norway. These studies focused on different types of LBP, CLBP, and NSCLBP. Sample sizes varied widely, from 15 to 165 participants per group. The mean age of participants was 15.2 to 50.6 years, with most studies including middle-aged adults. The proportion of male participants varied considerably across studies, from 0% to 100%. Baseline pain scores were reported using different scales, including the VAS, NRS, and NPS, and they generally indicated moderate pain levels, ranging from 4.7 to 6.46 out of 10. Baseline disability scores, where reported, ranged from 21.4 to 33.51 on the ODI. Follow-up periods ranged from 6 weeks to 3 years, with most studies having a follow-up duration of 12 weeks to 12 months (Table 1).
Quality assessment
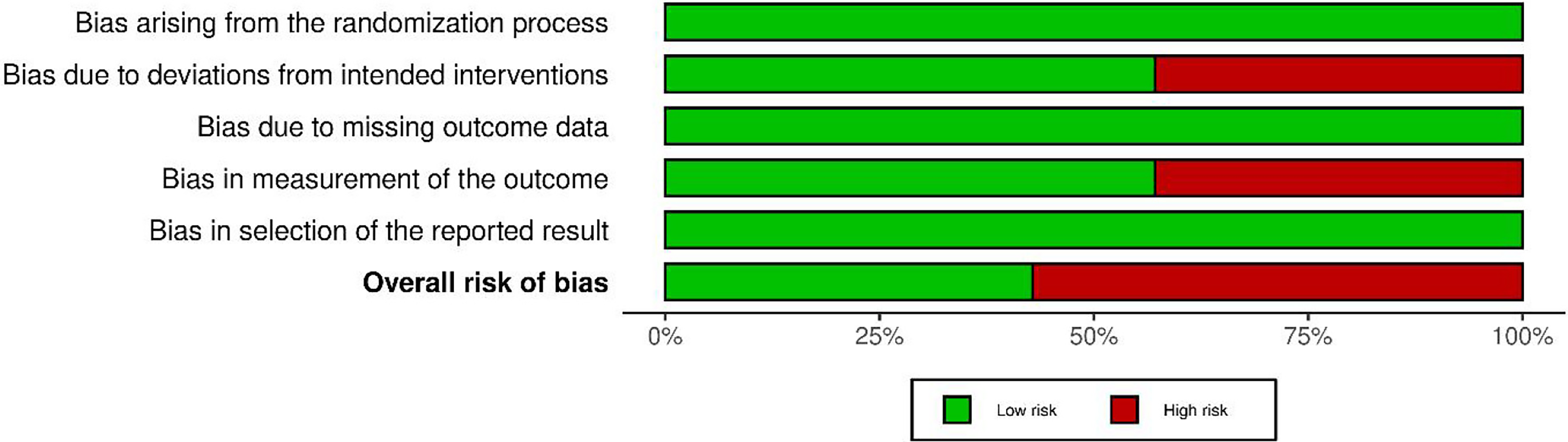
Risk of bias graph.
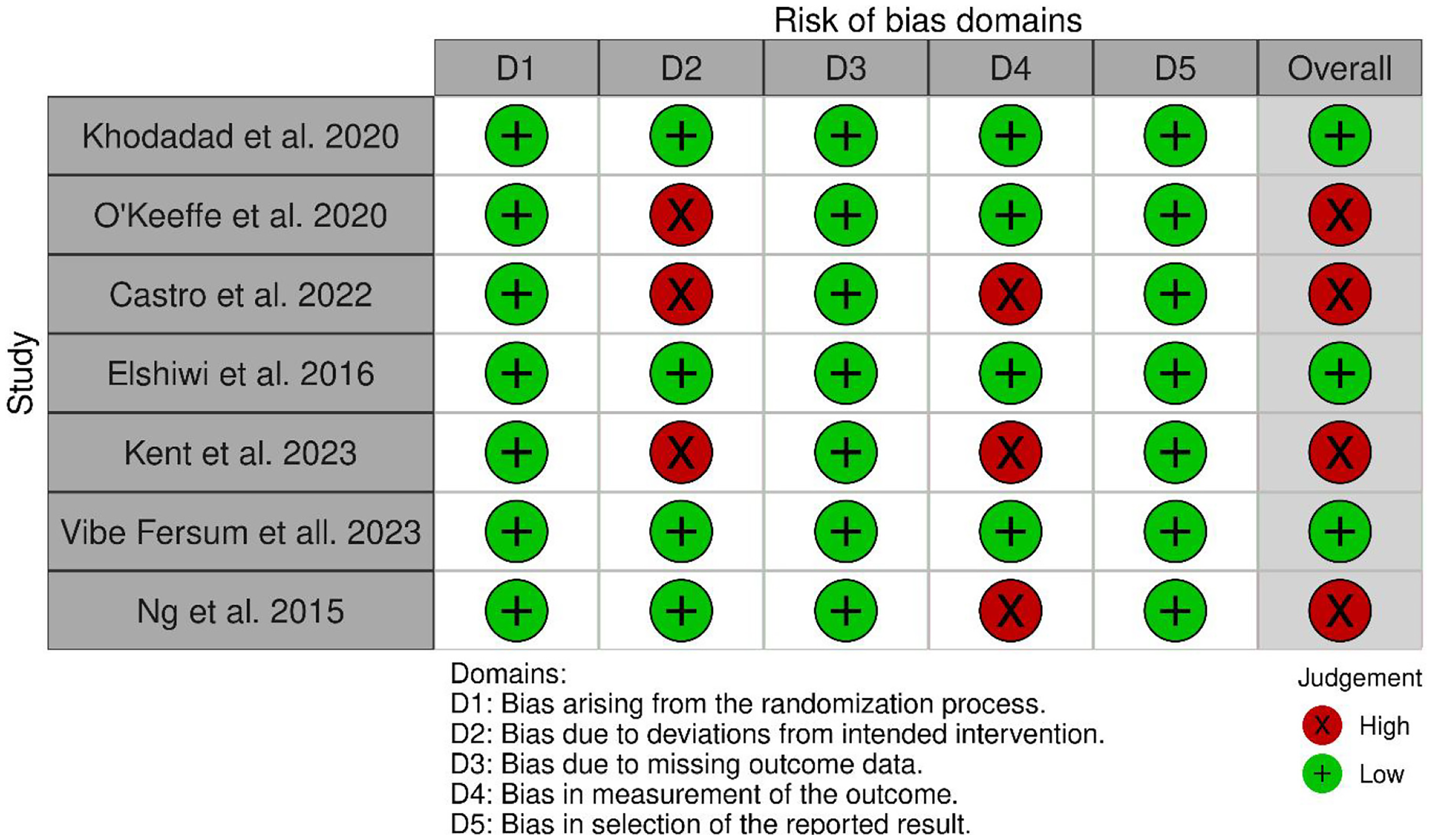
Risk of bias summary.
All studies showed a low risk of bias in domains D1 (randomization process), D3 (missing outcome data), and D5 (selection of reported result). However, variability was observed in domains D2 (deviations from intended interventions) and D4 (measurement of the outcome). Three studies (Khodadad et al. 2020, Elshiwi et al. 2016, and Vibe Fersum et al. 2023) demonstrated a low risk of bias across all domains and overall. The remaining four studies (O’Keeffe et al. 2020, Castro et al. 2022, Kent et al. 2023, and Ng et al. 2015) were judged to have a high risk of bias overall, primarily due to issues in domain D2 or D4, or both (Figures 2 and 3).
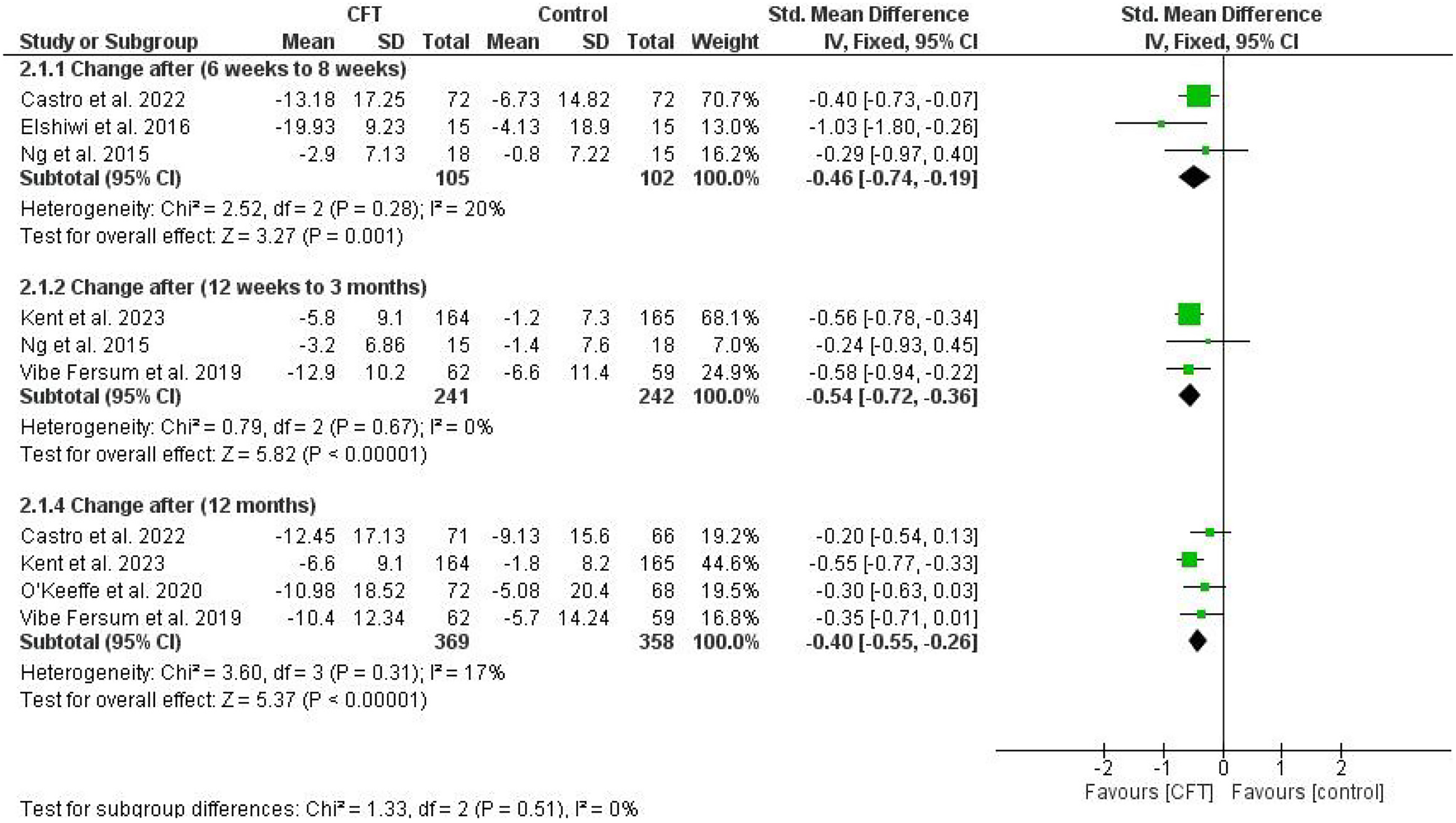
Forest plot shows the summary of the pooled SMD and the corresponding 95% CI for the Change in disability score with subgrouping according to the time of follow-up. Size of the square is equivalent to the statistical weight of each trial. The black diamond represents the pooled points estimate. The position of both diamond and squares relevant to the vertical line aligns with the significance of the results.

Forest plot shows the summary of the MD and the corresponding 95% CI for the Change in disability score after 6 months of treatment. Size of the square is equivalent to the statistical weight of each trial. The black diamond represents the pooled points estimate. The position of both diamond and squares relevant to the vertical line aligns with the significance of the results.
At 6 to 8 weeks [21, 24, 27], 12 weeks to 3 months [25, 26, 27], and 12 months [20, 21, 25, 26] after an intervention, a significant reduction in disability scores was observed in the CFT group as compared with the control group, with an SMD of

Forest plot shows the summary of the MD and the corresponding 95% CI for the Change in pain score after 6–8 weeks of treatment. Size of the square is equivalent to the statistical weight of each trial. The black diamond represents the pooled points estimate. The position of both diamond and squares relevant to the vertical line aligns with the significance of the results.
The pooled analysis of three RCTs [21, 24, 27] that included 207 patients showed a significant reduction in disability scores in the CFT group compared with the control group (SMD
Disability scores after 12 weeks to 3 months
Similarly, in a more extended period, CFT significantly decreased the disability score compared with the control group score in the pooled analysis of three RCTs [25, 26, 27] with a total of 483 patients (SMD
Disability scores after 6 months
After 6 months [20, 21], CFT significantly decreased the disability score compared with the score of the control group in the pooled analysis of two RCTs with a total of 290 patients (MD
Disability scores after 12 months
The pooled analysis of four RCTs [20, 21, 25, 26] that included 727 patients showed a significant reduction in disability scores in the CFT group compared with the control group (SMD
Pain scores
Pain scores after 6 to 8 weeks
The pooled analysis of three RCTs [19, 21, 24] that included 209 patients showed no significant reductions in pain scores for the CFT group from scores for the control group (SMD
Pain scores after 12 weeks to 3 months
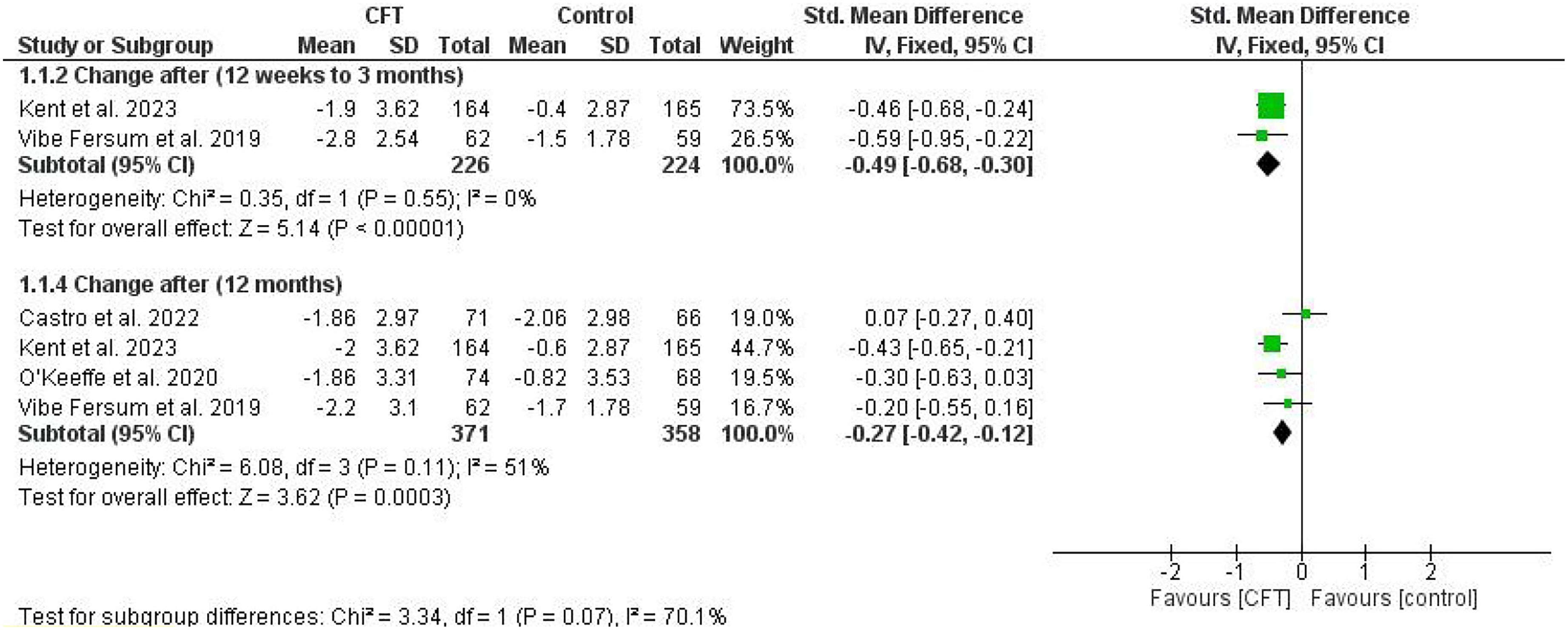
Forest plot shows the summary of the pooled SMD and the corresponding 95% CI for the Change in pain score with subgrouping according to the time of follow-up. Size of the square is equivalent to the statistical weight of each trial. The black diamond represents the pooled points estimate. The position of both diamond and squares relevant to the vertical line aligns with the significance of the results.
CFT significantly decreased the pain score compared with the score of the control group in the pooled analysis of two RCTs [25, 26] with a total of 450 patients (SMD

Forest plot shows the summary of the MD and the corresponding 95% CI for the Change in pain score after 6 months of treatment. Size of the square is equivalent to the statistical weight of each trial. The black diamond represents the pooled points estimate. The position of both diamond and squares relevant to the vertical line aligns with the significance of the results.
Similarly, after 6 months, CFT significantly decreased the disability score compared with the control group score in the pooled analysis of two RCTs [20, 21] with a total of 290 patients (MD
The pooled analysis of four RCTs [20, 21, 25, 26] that included 729 patients showed a significant reduction in disability scores in the CFT group compared with the control group (SMD
Discussion
In this systematic review and meta-analysis, we aimed to evaluate the effectiveness of CFT in managing LBP based on the findings of seven RCTs. The meta-analysis results indicated that CFT significantly improved disability scores across various time intervals. The pooled analysis of the impact of CFT after 6 to 8 weeks, 12 weeks to 3 months, 6 months, and 12 months revealed a significant reduction in disability scores for all time spans. However, the effects on pain scores were more varied. Our meta-analysis did not show significant differences in pain reduction after 6 to 8 weeks of CFT intervention. In contrast, we demonstrated a significant decrease in pain scores after 12 weeks to 3 months, 6 months, and 12 months of CFT intervention. These varying results suggested that the effect of CFT on pain scores may have been more apparent with longer-term interventions.
The observed improvements in disability scores with CFT might be attributed to several underlying mechanisms. CFT addresses both physical and cognitive aspects of LBP, potentially enhancing patient outcomes through a combination of pain management strategies and functional re-training [8]. By focusing on reducing fear-avoidance behaviors and improving physical function, CFT could facilitate a better adaptation to pain and promote more effective coping strategies. This multifaceted approach may contribute to sustained functional improvements, as seen in our meta-analysis results. Additionally, the emphasis on patient education and self-management in CFT could empower patients to engage more actively in their treatment, leading to better adherence and overall effectiveness [8].
In contrast to our findings, Devonshire et al. reported that CFT may not be more effective than other common interventions in reducing pain and disability for adults with chronic LBP. They emphasized the uncertainty surrounding the effectiveness of CFT, stressing the need for higher-quality studies to provide more definitive evidence [7]. Similarly, Miki et al. included three studies but found the quality of evidence to be very low. While they observed some statistically significant differences, they suggested that a re-evaluation of the effectiveness of CFT is warranted in future research [14]. On the other hand, our study demonstrated significant reductions in disability scores with CFT, highlighting its potential benefits for managing LBP.
The results of this meta-analysis and comprehensive review have important therapeutic implications for treating LBP. The findings imply that CFT may be effective in lowering disability ratings in people with LBP. The observed statistically significant decreases in disability ratings over periods ranging from 6 to 8 weeks to 12 months suggested that CFT may provide long-lasting and sustained improvements in functional outcomes. This demonstrated the potential of CFT as a powerful non-pharmacological strategy that could improve patients’ levels of daily functioning and overall quality of life [28, 29]. However, the effects on pain levels were more inconsistent, with a considerable decline in pain scores seen over some time intervals in some studies and no changes in these scores in the CFT and control groups in other studies. This implied that the duration of a CFT intervention and the severity of the condition causing the pain may influence how CFT affected the pain, and this may have made its measurement more complicated [28, 30]. The results highlighted the significance of using a thorough, multifaceted strategy to manage LBP. When one is attempting to provide comprehensive and patient-centered therapy, CFT could be helpful because of its emphasis on treating both physical and cognitive manifestations. For patients with LBP, particularly those with persistent or chronic symptoms, healthcare professionals, particularly physiotherapists, and other rehabilitation experts may want to consider adding CFT to their therapies [30, 31, 32]. Additionally, healthcare practitioners may modify CFT therapies to meet each patient’s unique requirements and preferences, so that their adherence to a therapy and its overall results would be improved. Integrating psychological interventions such as cognitive-behavioral techniques could address patients’ negative ideas and views of pain. This would help to further optimize patient recovery [33]. The study by Elshiwi et al. explored CFT for scoliosis-related LBP [24], but the principles of CFT are broadly applicable to various types of LBP, including CLBP. Future research should further explore CFT’s impact on different subtypes of LBP to strengthen the evidence base.
This study had several strengths, including a thorough literature search, incorporation of RCTs, analysis of consistent data, examination of various time frames, and evaluation of multiple outcomes. The presented meta-analysis systematically synthesized evidence from RCTs to evaluate the effectiveness of CFT in managing LBP at various time points. This research stands out for its incorporation of multiple outcomes; it evaluated both disability and pain scores to present an extensive view of CFT’s impacts. By examining effects at diverse time intervals, including 6 to 8 weeks, 12 weeks to 3 months, 6 months, and 12 months, this analysis provided insights into the temporal effectiveness of CFT. The inclusion of varied RCTs augmented the generalizability and statistical power of the findings, offering a heterogeneous yet coherent view across different populations and settings. The predominance of homogenous data in the selected studies ensured the reliability of the pooled results. The meta-analysis, by emphasizing the clinical implications of CFT, pointed toward its potential utility in patient-centered therapy. However, significant variability in pain score analyses and discrepancies in CFT interventions between studies warranted attention because different interventions were used for the different control groups. Further research is essential to corroborate the findings and investigate CFT’s long-term effects on LBP.
This meta-analysis had several specific limitations, including variability in intervention implementation, heterogeneity in outcome measures, and limited selected time points that might have missed nuances in treatment evolution. The exclusive selection of RCTs ensured high-quality evidence but may have limited the generalizability of the findings by excluding real-world and observational studies. The results highlighted a need for more standardized and rigorous RCTs and further exploration of real-world evidence. Future research is recommended to focus on comprehensive outcome reporting, standardized intervention implementation, and the ways in which various intervention durations and the severities of conditions causing pain affect pain levels so that these identified limitations can be mitigated.
Conclusions
This study rigorously evaluated the efficacy of CFT in managing LBP by scrutinizing results from seven RCTs. The meta-analysis concluded that CFT was significantly effective in reducing disability scores across different time intervals, from 6 to 8 weeks to 12 months, implying that it could induce sustained improvements in functional outcomes, providing a compelling non-pharmacological alternative for managing LBP. It especially emphasized the benefits of CFT in improving patients’ daily functionality and overall quality of life. However, the effectiveness of CFT in pain management was variable. While there were substantial reductions in pain scores at intervals of 12 weeks to 3 months, 6 months, and 12 months, no significant differences were observed in the time frame of 6 to 8 weeks. These inconsistencies suggested that the effects of CFT on pain levels possibly contingent on the duration of intervention and the severity of LBP and the condition causing it. The study substantiated the validity of incorporating CFT into therapeutic regimes, particularly by healthcare professionals focusing on rehabilitation. The multifaceted and inclusive approach of CFT, which emphasizes both the cognitive and physical aspects of LBP, can potentially offer a more effective and patient-centric treatment paradigm for LBP. Moreover, integrating cognitive-behavioral techniques to modify negative beliefs and perceptions about pain might optimize patient outcomes.
Footnotes
Acknowledgments
The authors extend their appreciation to the King Salman center For Disability Research for funding this work through Research Group no KSRG-2023-136.
Ethical approval
Not applicable.
Author contributions
Conceptualization, M.K. and M.A.M.; methodology, M.K.; software, M.K.; validation, M.K., K.M.A. and S.A.; formal analysis, M.K.; investigation, K.M.A. and S.A.; resources, M.K.; data curation, M.K., K.M.A. and S.A.; writing – original draft preparation, M.K.; writing – review and editing, M.A.M., K.M.A. and S.A.; funding acquisition, M.K. All authors have read and agreed to the published version of the manuscript.
Funding
The authors extend their appreciation to the King Salman center For Disability Research for funding this work through Research Group no KSRG-2023-136.
Conflict of interest
The authors have no conflict of interest to report.