
Abstract
AIMS:
Critical limb ischemia (CLI) patients are characterized by intractable pain in spite of medication, non-healing ulcers, and gangrene. The objective of this study was to investigate whether or not isovolemic hemodilution treatment can reduce the rate of major amputations in CLI.
METHODS:
28 patients were studied who had tissue loss on Rutherford Grade III, Category 5 or 6. The subjects were divided into two arms: standard-of-care, conventional therapy (CT) (n = 15) as a control group and hemodilution therapy (HT) (n = 13) as a study group. For the HT group, weekly isovolemic hemodilution was performed over 4 consecutive weeks, removing 250 ml of whole blood with the infusion of hydroxyl-ethyl starch solution. Blood viscosity, hematocrit, hemoglobin, ankle-brachial index, VA pain scale, time-to-amputation from admission, and survival time were measured.
RESULTS:
The mean Hct gradually decreased from 36.6 to 35.1, whereas the WBV at a shear rate of 1 s–1 significantly decreased from 18.2 to 10.5 during the same period. Subsequently, tissue oxygen delivery index, defined as the ratio of Hct to WBV at a shear rate of 1 s–1, increased from 24.4 to 37.0 by 51.7%, suggesting improvements in oxygen delivery in the patients. The average rate of lower limb major amputation in the control group was 93% (14/15), whereas that in the study group was 31% (4/13) (p = 0.001). Amputation-free median survival time and amputation-free 5-year survival rate in the control group were 1.2 months and 7%, while those in the study group were 30.2 months and 44% (p = 0.001). There were no adverse effects from repetitive hemodilution in the study group.
CONCLUSIONS:
Isovolemic hemodilution treatment of CLI patients was found to be well-tolerated and reduced the rate of major amputation resulting from the deterioration of CLI.
Keywords
Introduction
According to ACC/AHA Guidelines for the management of peripheral arterial obstructive disease (PAOD) patients, critical limb ischemia (CLI) is defined as intractable limb pain that occurs at rest or impending limb loss that is caused by severe compromise of blood flow to the affected extremity [1]. In general, any patient with chronic ischemic resting pain, ulcers, or gangrene attributable to objectively proven PAOD can be considered to have CLI [2]. As a disease state, PAOD is generally characterized by chronically inadequate blood flow, resulting in inadequate oxygen delivery to the limbs, whereas CLI presents after chronic impairment of blood supply, setting off a cascade of pathophysiologic events that ultimately lead to resting pain, tissue loss in the legs, or both [3]. CLI patients often have ankle pressure less than 50 mmHg and toe pressure less than 30 mmHg. Ankle-to-brachial indices (ABI) for ischemic resting pain and impending tissue necrosis are 0.3±0.1 and 0.1±0.1, respectively [4]. Patients with CLI experience significant morbidity, typically requiring major amputation within 6 months to 1 year [3] with cardiovascular event rates surpassing those in patients with symptomatic coronary artery disease [5], usually leading to 50% mortality among the major amputation patients. Their 5-year survival rate is only about 20%, which are very poor expected outcomes comparable to those of pancreatic cancer patients.
Treatments of CLI include revascularization surgery, thrombolytic therapy, antithrombotic therapy, heparin-induced extra-corporal LDL precipitation, and hemodilution therapy [6–8]. Both isovolemic and hypervolemic hemodilutions have been used in PAOD (Fontaine stage II) patients by a number of investigators [9–11]. In general, hemodilution resulted in increased resting blood flow at lower extremities and pain-free walking distance [7, 10–12], phenomena that could be attributed to reduced hematocrit, fibrinogen, plasma viscosity, and erythrocyte aggregation [9, 13–15]. In particular, Wilhelm et al. reported that hemodilution resulting in improved plasma viscosity and erythrocyte aggregation could have a positive effect on microcirculation [14].
However, since hemodilution reduces hematocrit, it also reduces the oxygen carrying capacity of blood. Thus, in order for the hemodilution to improve oxygen delivery at tissue, one needs to compare the rate of decrease in whole blood viscosity (WBV) with that of hematocrit. In this regard, Ernst et al. proposed the following as a necessary condition of successful hemodilution: the rate of decrease in the low-shear WBV should be substantially larger than that of the hematocrit after hemodilution, as they found that the rate of decrease in the high-shear WBV was about the same as that of the hematocrit [12].
In spite of a large number of studies reporting the benefits of hemodilution observed in CLI and PAOD, it has not been clearly demonstrated whether or not isovolemic hemodilution can improve intractable pain and non-healing ulcers in CLI patients diagnosed as Rutherford classification (Grade III, Category 5 or 6, or Fontaine stage IV), with the endpoints of reducing or delaying major amputation.
The primary hypothesis of the present study was that the oxygen delivery to tissues would be increased by reducing WBV through isovolemic hemodilution, thus improving CLI symptoms and clinical outcomes including amputation. The proposed mechanisms by which isovolemic hemodilution reduces WBV are reductions in hematocrit and erythrocyte aggregation as well as the reductions in fibrinogen and plasma viscosity [15]. Therefore, the objective of the present study was to investigate the efficacy of isovolemic hemodilution therapy in CLI patients and to determine the association of hemorheological parameters to CLI outcomes. In addition, the study examined the safety of isovolemic hemodilution in critically ill CLI patients.
Methods
Twenty-eight patients were recruited for the present study and divided into two arms: standard-of-care, conventional therapy (CT) (n = 15) as a control group and hemodilution therapy (HT) (n = 13) as a study group. Both groups’ Rutherford classifications were equal, i.e., Grade III, category 5 (tissue loss below the metatarsal joint) or category 6 (tissue loss above metatarsal joint). The patients in both groups had end-stage peripheral obstructive vascular disease resistant to maximal medical therapy or had surgical revascularization therapy which either proved insufficient, was contra-indicated, or declined surgery by the patient due to old age or poor general condition. The computed tomography angiographic findings in both groups were similar, i.e., long segment obstruction of iliac and/or superficial femoral and/or below arterial lesions (Fig. 1). Although the HT group had more bed-ridden patients than the CT group as shown in Table 1, the severities of both groups were similar. Angiosome concept based on vascular mapping was also matched in both groups.
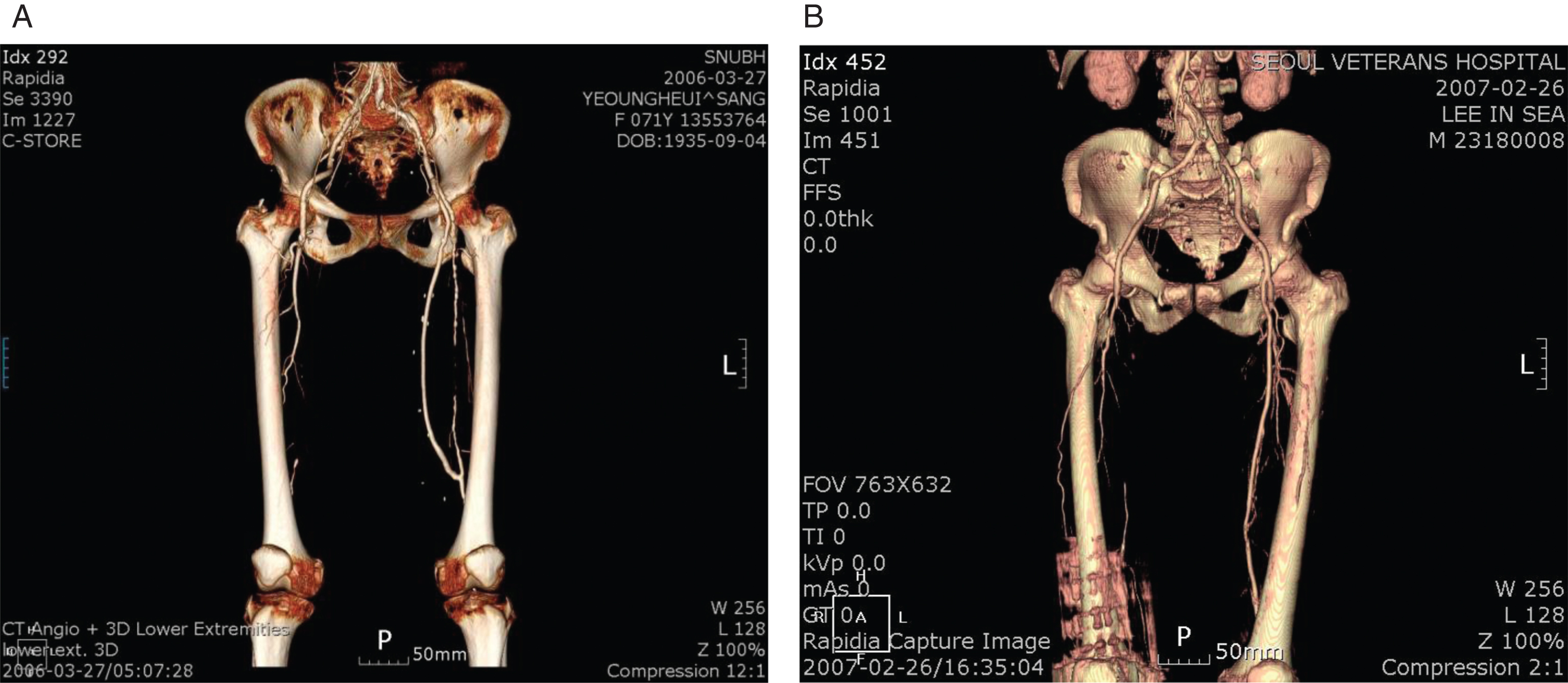
Computed tomogram angiography of the control (A) and study (B) patients who had similar long segment obstruction of right superficial femoral arteries and right toe discoloration (A) and gangrene (B). They were admitted via emergency department for severe pain and limb tissue loss. The control patient (CT patient No.8) was 72 years old, female, who was self-ambulatory status, having left limb bypass surgery previously, underwent coronary artery bypass surgery and then right above knee amputation at 3.3 months and finally expired due to sepsis at 5.7 months since emergency department admission. The study patient (HT patient No.9) was also 72 years old, male, bed-ridden status, had repetitive hemodilutions and a limb bypass surgery, with delayed right below-knee amputation till 30.2 months, and expired at 59 months due to lung cancer terminal.
Characteristics of critical limb ischemia (CLI) patients in hemodilution therapy (HT) and conventional therapy (CT) groups before treatment. There were no statistically significant differences between two groups
HT; hemodilution therapy, CT; conventional therapy, ER; emergency room; t-test and chi-square or Fisher’s exact test were used.
Patients in the CT group were treated by medications, which include combinations of anti-platelets, vasodilators, statin derivatives, and anti-oxidant drugs. For HT group, four isovolemic hemodilutions were planned over four consecutive weeks, each time removing 250 ml of patient’s blood with the infusion of an equal volume of hydroxyl-ethyl starch (HES) solution (Pentaspan, Bristol-Myers Squibb). Of note is that Pentaspan consists of 10% Pentastarch (Mw ∼50,000) in 0.9% sodium chloride solution, approved as a plasma volume expander. Since most previous hemodilution studies in CLI and PAOD removed 250–500 ml per week over 4–6 week period [6–11], the present study chose a similar volume and frequency of hemodilution. The HES solution used in the present study as a plasma volume expander has also been utilized in prior clinical studies of isovolemic hemodilution in PAOD [9, 12]. The institutional ethics committee (institutional review board, IRB) approved the research protocol, and all procedures were in accordance with institutional guidelines. Study-assistant nurse performed hemodilution procedure under physician supervision in accordance with the IRB protocol.
The aforementioned medications were administered under the same guidelines for dosing and formulation for two groups. In addition, the same criteria for surgery and limb amputation were applied to patients in both groups. The indication for the primary major amputation of the lower extremity was an advanced distal ischemia with uncontrollable pain or infection, which included un-reconstructable arterial occlusive disease, necrosis of weight-bearing portion, fixed flexion contracture of the leg, and terminal illness or limited life expectancy. In short, the amputation criterion was when the gangrene aggravated to sepsis or having severe intractable pain in spite of maximal medical opioid analgesia. In cases where gangrene was stabilized, such as with no aggravation and with tolerable pain, biologic dressing was applied with the aim of achieving wound healing. Complete wound healing is defined as no purulent or serous discharge from wound and complete epithelialization achieved with or without minor amputation. When existing gangrene did not worsen or improved, standard-of-care, conventional therapy was then utilized in both groups. In the HT group, medical decision for amputation was made after the completion of hemodilution.
In both groups, revascularization surgery was performed based on the judgment of the primary investigator, when feasible. In order to minimize the subjective judgment of the researchers involved in the present study, the clinical decisions for amputation and the scope of amputation were made by an independent orthopedic physician who was blinded to the present study.
Whole blood viscosity (WBV), hematocrit (Hct), hemoglobin (Hg), ankle-brachial index (ABI), visual analog (VA) pain scale [16], complete wound healing, mortality, cause of death, time-to-major amputation from admission, and median survival time were recorded. The WBV was measured with a scanning capillary tube viscometer (SCTV), (Bio-Visco, Inc., Korea). Viscosity μ is mathematically defined as the ratio of wall shear stress τ
w
to wall shear rate
The wall shear stress τ
w
was determined from the pressure drop, ρg [h1 - h2], across a capillary tube positioned between two vertical tubes of the U-tube section in the SCTV [18]. The pressure drop was obtained from the height difference, [h1 - h2], between the two vertical tubes. The wall shear rate
In addition to WBV, the present study utilized a hemodilution parameter which represents the deliverability of blood and oxygen to tissue called the tissue oxygen delivery index (TODI), which was defined as the ratio of hematocrit to the WBV measured at a wall shear rate of 1 s–1 (μ1):
Note that TODI is similar to the oxygen delivery index, a parameter that has been introduced by other researchers [19], but different in using low-shear WBV instead of high-shear WBV as its denominator.
In addition, the parameter % TODI change is suggested as a hemodynamic marker for comparing the trends in HT groups, as a possible predictor of clinical outcomes in CLI or PAOD patients, and is calculated as follows;
We conducted student t-tests for the numerical variables and Chi-square or Fisher’s exact test for the categorical variables as a nonparametric statistical test between the groups. Survival analyses were calculated using the Kaplan-Meier method for overall and amputation-free survivals, and the date of admission was used as the starting time; statistical comparisons were made using the log-rank test. According to the variable factors–including the following: age, male sex, body weight, height, BMI, bed-ridden status at admission, ER admission, surgical revascularization, wound healing, ABI improvement and group–, a Cox’s proportional hazards model was used for the risk analysis to evaluate the independent prognostic roles of these factors in overall and amputation-free survival. The level of significance was set at 5% (p < 0.05). We used SPSS 12.0KO for Windows, Release 12.0.1 statistical software for analysis.
Table 1 shows the characteristics of CLI patients in the two groups. There were no statistically significant differences in age, male sex, body weight, height, body mass index, bed-ridden status at admission, emergency room admission and surgical revascularization to the affected limb between the two groups (p > 0.05) (Table 1). CT groups had a tendency of older but more ambulatory status than HT groups, however the differences were not statistically significant.
For the patency and distal run-off of revascularization surgery, the CT group had seven revascularization operative procedures, such as abdomino-bi-femoral arterial bypass in one case, axillo-bi-femoral arterial bypass in two cases, femoro-popliteal arterial bypass in one case, thrombo-embolectomy in two cases and femoral angioplasty in one case, respectively, whereas the HT group had five operative procedures during the study period, such as abdomino-bi-femoral arterial bypass in three cases and femoro-popliteal arterial bypass in two cases, respectively. All of the surgical procedures conducted for revascularization to the ischemic limbs in the two groups and long segment arterial obstruction were similar features between the two groups. Of note is that some patients or their families refused revascularization surgery for reason of unwillingness, poor general condition, old age, etc. However, the number of surgeries was not statistically different in the 2 groups, 7/15 in the CT group and 6/13 in the HT group (p = 0.479).
Although 4 hemodilutions over 4 consecutive weeks were originally planned in the HT group patients, the planned hemodilution schedule was dropped for certain HT patients due to underlying disease progression to sepsis (HT patient No.10), refusal during hemodilution (HT patient No.14), etc. On the average, the mean frequency of hemodilution was 3.23 per patient (eight patients had 4 hemodilutions over 4 consecutive weeks, 1 patient had 3 hemodilutions in 3 weeks, 3 patients had 2 hemodilutions in 2 weeks, and 1 patient had 1 hemodilution, respectively.) WBV was measured at 2.64 times per patient (Five times in one patient, four times in two patients, three times in three patients, two times in two patients, and one time in three patients, respectively.)
In spite of limited patient dropout from hemodilution in this study, there were significant differences in 5-year outcomes. Table 2 summarizes the results of hemodilution therapy of CLI patients. The ABI was improved in 46% (6/13) of patients in the HT group and the VA pain scale [16] was improved in 77% (10/13). Complete wound healing was achieved in only one (7%) in the CT group, in contrast with 77% (10/13) of patients in the HT group (p = 0.000). The remaining 23% of patients in the HT group were observed to have small improvements in wound healing or stabilization of disease. With respect to the endpoints of major amputation: 93% (14/15) of the patients in the CT group had major amputations, in contrast to only 31% (4/13) in the HT group (p = 0.001) as of May 2012. Furthermore, the average time-to-amputation was 2.7±3.5 months in the CT group, whereas it was 11.1±13.0 months in the HT group (p = 0.290). There were no statistically significant differences in the follow-up duration, median survival time, 5-year survival rate, and mortality rate between the two groups. However, amputation-free median survival time and amputation-free 5-year survival rate were 1.2 months and 7% in the control group, while they were greater than 30.2 months and 44% in the HT group (p = 0.001) (see Table 2).
Summary of the results of the hemodilution therapy (HT) of critical limb ischemia (CLI) patients in comparison with those from the conventional therapy (CT), and the causes of death in the two groups
Summary of the results of the hemodilution therapy (HT) of critical limb ischemia (CLI) patients in comparison with those from the conventional therapy (CT), and the causes of death in the two groups
Mortality cases in HT group: 1) HT patient No.2: Ulcer bleeding, Acute Renal Failure, Shock at 82 days 2) HT patient No.5: Cardiac death at 104 days 3) HT patient No.8: Cerebral hemorrhage, Brain death at 287 days 4) HT patient No.9: Lung cancer terminal at 1,754 days 5) HT patient No.10: Chronic pancreatitis, Pan-peritonitis, Sepsis at 24 days; Mortality cases in CT group: 1) CT patient No.1: Lung cancer terminal at 488 days 2) CT patient No.2: Lung cancer terminal, sepsis at 83 days 3) CT patient No.7: Congestive heart failure, acute renal failure, sepsis at 696 days 4) CT patient No.8, 12 and 14: Sepsis at 172 (No.8), at 308 (No.12) and at 282 (No.14) days 5) CT patient No.15: Hopeless at 162 days NA; not available, MST; median survival time, YSR; year survival rate, *MST not reached yet.
Figure 2 shows variations of the mean values of Hg averaged over 13 patients in the HT group, which gradually decreased with repeated hemodilutions. The mean values of Hg and Hct dropped from 11.8±1.6 g/dl and 36.7±4.7% (before the first hemodilution) to 10.5±1.2 g/dl and 33.1±3.3%, respectively, over 4 weeks during the hemodilution period without serious adverse effect. According to the simple regression analysis, regression equations were y = –0.3475x + 11.907 in Hg and y = –0.9192x + 36.742 in Hct.
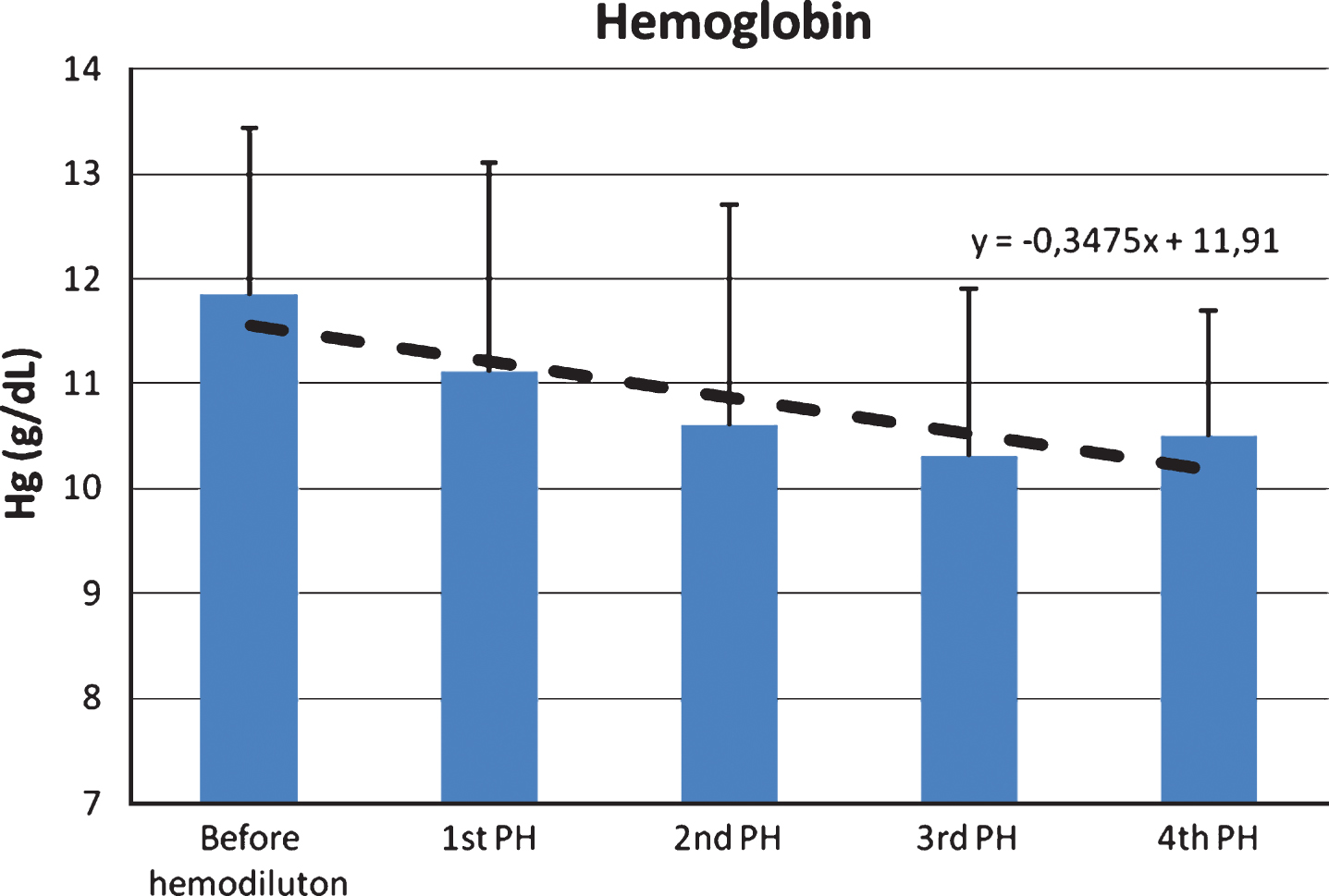
Variations of the mean values of hemoglobin (Hg) averaged over 13 patients in the hemodilution therapy (HT) group over 4 weeks. PH; phlebotomy for hemodilution.
Figure 3 shows changes in the mean values of Hct, WBV, and Tissue Oxygen Delivery Index (TODI) over 4 weeks in the 7 patients who had available dataset in the HT group. The mean Hct gradually decreased slightly over time from 36.56% to 35.13%, whereas the rate of decrease in the WBV at a shear rate of 1 s–1 was relatively much greater than the mean Hct, from 18.20 to 10.52. With TODI defined as the ratio of Hct to WBV at a shear rate of 1 s–1, there was a significant increase in this parameter observed in the third week from 24.41 to 37.03, a 51.7% increase in mean values for TODI. After the third week, the mean TODI leveled off to 27.26, which was 11.2% greater than baseline levels, and were maintained during the rest of the hemodilution period. In general, the mean TODI values significantly increased during the first 3 weeks in HT patients and demonstrated greater sensitivity than hemodilution-induced changes in Hct and WBV.
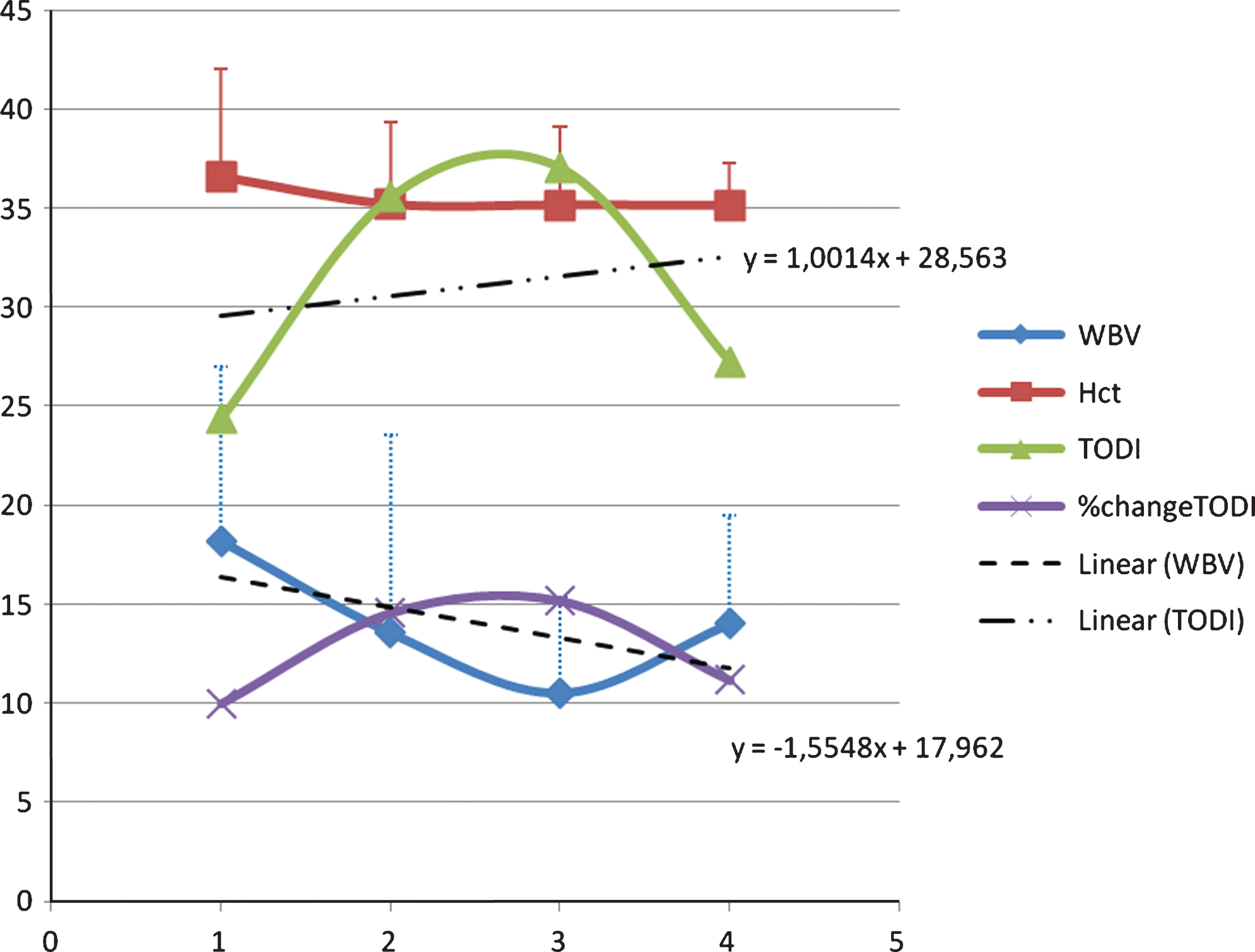
Changes in the mean values of hematocrit (Hct), whole blood viscosity (WBV), and tissue oxygen delivery index (TODI) over 4 weeks in the seven patients who had available dataset in HT group. The mean Hct gradually decreased over time, whereas the rate of decrease in the WBV was much greater than the mean Hct, resulting in a significant increase in the oxygen deliver to the tissue in the second week and in the following 2 weeks.
Another interesting finding in TODI was the different trend between the amputated and the salvaged subgroups within the HT arm, when the initial and subsequent values of TODI were compared along the time sequences. Figure 4A shows negative trends of % TODI change along the time sequences from three amputated subgroup in the HT group. Their final TODI value was lower than the initial TODI value or markedly decreased. Their mean slope over time was – 11.807. Figure 4B shows positive trends from six salvaged subgroup. Their final TODI value was higher than the initial value and the slope over time was +11.35. Based on these observations, it may be possible to use % TODI change as a hemodynamic marker for predicting the outcome of limb ischemia and for providing additional information that whether they could be amputated or salvaged in CLI patients.

Changes in the % TODI value along time sequence between two subgroups in the HT group: three amputated (A) and six salvaged (B). The % TODI change was calculated as follows; [(each TODI value – initial TODI value)/initial TODI value] x100. In the amputated subgroup (A), the % TODI change increased initially about two fold, but decreased rapidly and finally converted the minus values so that their slope over time was – 11.807. However, in the salvaged subgroup (B), the % TODI change increased initially similar to the amputated subgroup (A). Then, the pattern of the % TODI change went down and up again, and finally sustained as positive higher values than the initial one. Their slope over time was +11.35.
Figure 5 shows overall survival and amputation-free survival curves for both groups. In terms of overall survival, the HT group had superior tendencies in 3 and 4 year survival to CT group, but the difference was not statistically significant (p = 0.8151). In amputation-free survival, only 7% (1 out of 15) in the CT group survived without major amputation after 60 months (amputation-free 5-year survival rate), whereas in the HT group, 44% (8 out of 13) survived without major amputation, suggesting a beneficial effect of HT (p = 0.0008). In the CT group, the tissue loss of CLI was found to be generally unchanged in spite of conventional therapy with the aforementioned medications and revascularization surgery. In other words, the clinical outcome for unhealing limb ischemia for the CT group was major amputation and/or death.
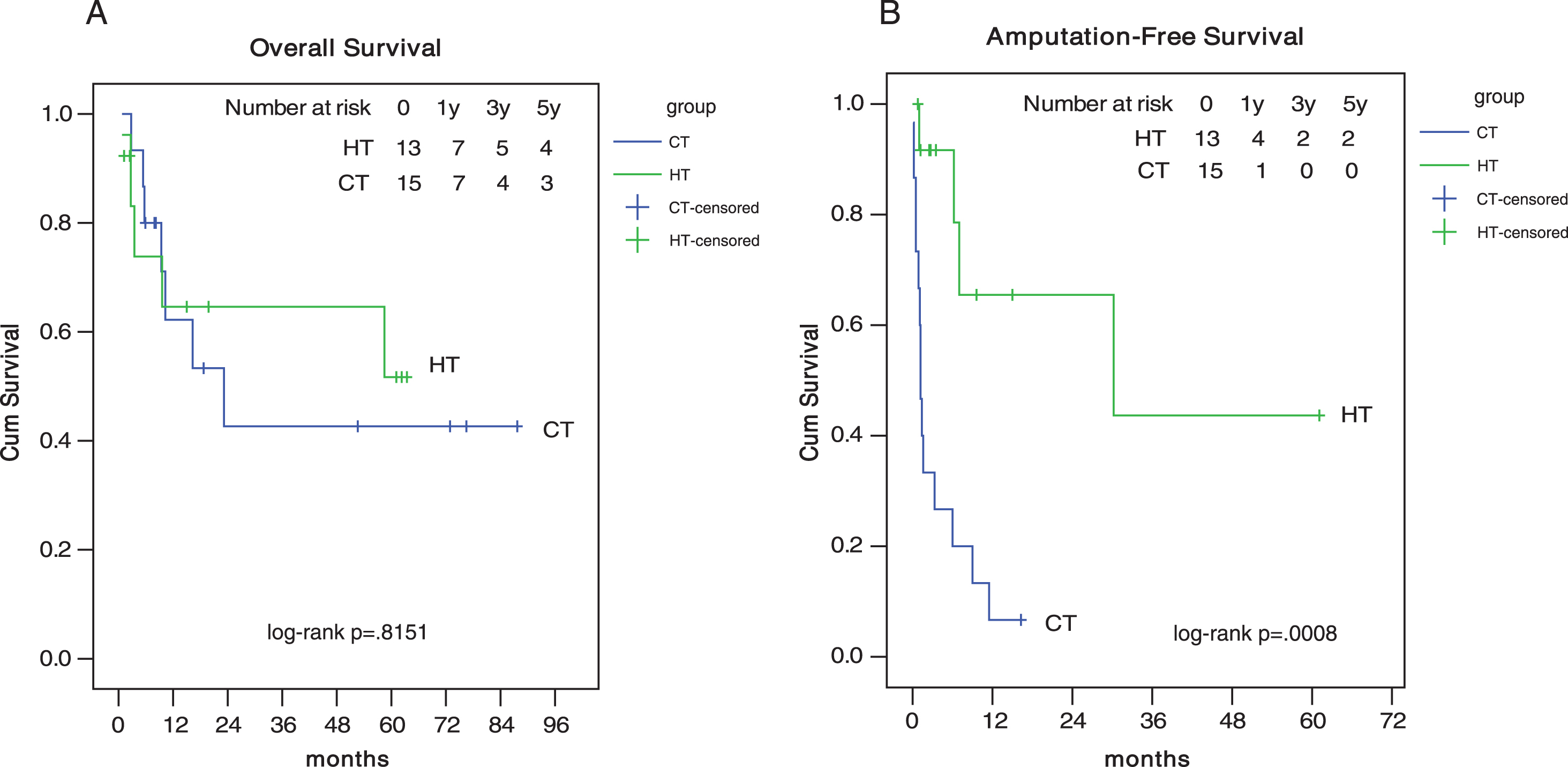
Overall and Amputation-free survival curves for both hemodilution therapy (HT) and conventional therapy (CT) groups. In the CT group, only 7% survived (amputation-free 5-year survival rate), whereas in the HT group, 44% survived without major amputation after 60 months (p = 0.0008), indicating a beneficial effect of HT. Amputation-free median survival time is 1.2 months in CT group and 30.2 months in HT.
In Cox regression analysis, among the variables, such as age, male sex, body weight, height, BMI, bed-ridden status at admission, ER admission, surgical revascularization, wound healing, ABI improvement and group, only the bed-ridden status was an independent prognostic factor of overall survival (p = 0.046, OR = 3.418, 95% CI 1.019∼11.461) and wound healing in amputation-free survival (p = 0.002, OR = 0.039, 95% CI 0.005∼0.305).
Table 2 also provides the causes of death in the two groups. To confirm the safety issue of hemodilution therapy in critically ill CLI patients, we examined the cause of death in detail as follows. The CT group had 7, whereas the HT group had 5 all-cause follow-up mortalities. In the 5 mortalities in the HT group, one patient (HT patient No.2) had complete wound healing after the hemodilution treatment. However, 82 days after admission, the patient of 59 years of age experienced shock caused by peptic ulcer bleeding and subsequent acute renal failure. Another patient of 76 yrs of age (HT patient No.5), who had cardiac valvular disease, also had complete would healing after the hemodilution therapy but had cardiac death 104 days after admission. A third patient (HT patient No.8) received coronary artery bypass graft for ischemic heart disease and aorto-bi-femoral artery bypass for limb ischemia then underwent minor toe amputation and skin graft for CLI. His lower limb ischemia was healed completely, and he was discharged. However, this patient was discovered at home at 287 days having expired due to brain death caused by cerebral hemorrhage. A fifth patient (HT patient No.9) had experienced pain improvement and complete wound healing and discharged. However, his wound aggravated again and was amputated at 906 days, and this patient expired due to lung cancer terminal at 1,754 days. The last patient (HT patient No.10), who had a history of psychiatric medication, suffered chronic pancreatitis and limb traumatic injury pain due to previous accidental fall, which led to pan-peritonitis and then sepsis, and finally expired.
Since the four patients expired after 82 days from the enrollment in the present study, these events were not related to the hemodilution treatment. The last patient’s death occurred on the 24th day after the enrollment in the study, i.e., after the second hemodilution treatment. However, as his cause of death was peritonitis and sepsis, it was not directly related to the hemodilution therapy. As such, in this study, it could be concluded that no direct adverse events or complications were observed to be caused by the hemodilution therapy in the HT group.
The present results demonstrated isovolumic hemodilution yielded greater improvements in low-shear WBV than in high-shear WBV. For example, mean low-shear WBV was observed to decrease by approximately 39% after the first hemodilution and remained at that level for the next 3 weeks, whereas mean high-shear WBV decreased by approximately 16% after the first hemodilution and remained at that level for the next 3 weeks. Hemodilution has been reported elsewhere to cause erythrocytes to be less prone to aggregation [13, 20] and also to reduce fibrinogen and plasma viscosity levels, which are among the key determinants of the low-shear WBV [21]. Hence, substantial changes in the low-shear WBV in the HT group may have been due to reduced erythrocyte aggregation as well as reduced fibrinogen and plasma viscosity.
Since hemodilution decreases hematocrit (and hemoglobin), which is also one of the primary determinants of WBV [21], it is useful to compare the relative percent changes in hematocrit and WBV. The percentage drop in the hematocrit was in the range of 3.5–13.6% after hemodilution. Thus, the decrease in the hematocrit was relatively smaller than the decrease in the low-shear WBV at a shear rate of 1 s–1 (i.e., 39%). According to Ernst and his colleagues [12, 22], this is a necessary condition for hemodilution therapy to improve oxygen delivery at micro-vessels. Note that the blood flow velocity corresponding to the low-shear WBV in the SCTV (scanning capillary tube viscometer) at a shear rate of 1 s–1 was 0.01 cm/s, which is in the range of the flow velocity in micro-vessels [23, 24]. Thus, the significant improvement (i.e., reduction) in low-shear WBV after hemodilution may be indicative of enhanced flow in the micro-vessels.
Oxygen delivery index (ODI) is a parameter that has been previously used to evaluate the amount of oxygen delivered by blood flow. When ODI was calculated using the high-shear WBV in this study, ODI did not show any increase after hemodilution because the changes in the hematocrit and high-shear WBV were approximately comparable. Furthermore, high-shear WBV which was obtained with a flow velocity of 3 cm/s at SCTV [18] would not be expected to be clinically meaningful for the extremely slow flow (i.e., <0.01 cm/s) at micro-vessels. Thus, the present study introduces the parameter of TODI (tissue oxygen delivery index), see Equation (2). As one can see in Fig. 4, TODI increased by 50–60% after hemodilution, indicating improved oxygen delivery at micro-vessels. Of note is that the flow at micro-vessels is primarily controlled by the viscous forces rather than the inertial force of blood as the ratio between the inertial to viscous forces is about 0.001 [24–26]. Thus, any changes in the viscous property of blood critically influence the overall flow characteristics in micro-vessels.
In the present study, TODI was found to be the hemodynamic marker with a potential for predicting adverse clinical outcomes in CLI patients, as compared with Hct and WBV alone. Hence, the trends of % TODI change could be an interesting finding between the amputated and salvaged subgroups among the HT patients.
Another interesting finding in the present study was the long-lasting effect of hemodilution. Although a maximum of four hemodilutions over one month were conducted in CLI patients, the rheological benefit of hemodilution appeared to persist for a longer duration in some patients. A similar duration effect was observed by Wolf et al. [27] in a hemodilution study with central retinal vein occlusion patients, which reported a significant reduction in plasma viscosity and a significant increase in visual acuity lasting for 12 months in spite of one 10-day trial of hemodilution therapy. In addition, Mirhashemi et al. [28] reported that hemodilution was particularly effective in increasing oxygenation in ischemic tissue, while it had a comparatively small effect under normal conditions. Hence, one may speculate that once the hemodilution restores perfusion in a once-ischemic limb by improving the rheological properties of blood, further administration of hemodilution therapy may have little incremental than the initial one.
In the present study, CLI patients in both groups had relatively low BMI (19.7±4.1 and 20.0±3.5 kg/m2 for HT and CT groups, respectively, p = 0.613, see Table 1). Accordingly, due to CLI and other underlying conditions, these subjects might be expected to tolerate hemodilution poorly relative to healthy subjects, and the effect of repeated hemodilutions could be expected to affect them more adversely than healthy subjects. In spite of the fact that most patients in the present study were anemic with a mean initial Hct of 36.8±5.5%, repeated hemodilutions of 250 ml over 4 consecutive weeks or less did not produce any adverse signs during the 4-week period and for the next 60-month period.
There are several limitations in the present study. First, there was significant patient dropout in this study: originally four hemodilutions and WBV measurements over four consecutive weeks had been planned in each patient. However, in these critically ill patients, only 3.23 hemodilutions and 2.64 WBV measurements per patient were performed. Second, the WBV data were obtained only in the patients in the HT group, but not obtained in the patients in the CT group due to the limited resources in the WBV measurement. Third, this study was not a randomized controlled trial but a mixed comparative study. Therefore, increasing population size as well as adding randomization and blinding measures such as a sham therapy for the CT group may increase the impact of future studies on this topic.
Conclusions
Critical limb ischemia is a major concern in the elderly, who face high rates of major amputation and death in spite of maximal medical and surgical treatments. In Rutherford Categories 5 and 6 chronic CLI patients, repeated therapeutic hemodilution improved WBV, delayed major amputation, and significantly altered endpoints for limb salvage. Tissue oxygen delivery index, a hemodilution parameter emphasizing the deliverability of blood to tissues, was correlated with the endpoint. Future studies are needed to analyze WBV and tissue oxygen delivery index with a larger group of CLI or PAOD patients to elucidate the effect of hemodilution and mechanisms of action clearly. In addition, the present study did not identify any adverse effect directly attributable to the repeated hemodilutions.